
Abstract
Objective
The objective of this report is to evaluate migraine, migraine characteristics, and underdiagnosis of migraine in a large population sample of Mexican women.
Methods
Participants are part of a prospective cohort of Mexican teachers. Between 2011 and 2013, 77,855 participants completed a detailed questionnaire on headache characteristics. Migraine was defined according to criteria of the International Classification of Headache Disorders (ICDH-II).
Results
We found lifetime migraine prevalence was 19%, prevalence peaked at 40–44 years (20.4%) and only 45.1% participants with migraine had a previous diagnosis of the disease.
Conclusion
Estimated lifetime prevalence of migraine was higher than previous reports in Latin America. Migraine may be underdiagnosed and undertreated in Mexico despite its considerable burden.
Introduction
Migraine is ranked as one of the 10 leading causes of disability worldwide (1) and is associated with a number of neurological, cardiovascular and psychiatric diseases (2–4).The prevalence of migraine among adults is 11% (16% in women and 6% in men) (5), and it is somewhat higher in Western countries as compared to other regions of the world. In Latin America it is estimated that fewer than 10% of adults are affected (6), yet, despite its considerable burden, migraine is underdiagnosed and undertreated (5). There is only limited information on the prevalence, diagnosis and characteristics of migraine in Mexico. In this study, we sought to evaluate migraine and migraine characteristics in a large population sample of Mexican women.
Methods
The Mexican Teachers’ Cohort (MTC, ESMaestras) is a prospective study of 115,343 Mexican female teachers who responded to a questionnaire on lifestyle, reproductive factors and medical conditions in 2006–2008. In the first follow-up cycle (2011–2013), 77,855 participants updated their information and completed a detailed questionnaire on headache and headache characteristics. After excluding 6807 (8.7%) participants with missing values in headache-related questions, the final study population was 71,048. Participants were first asked: Have you ever had a headache that was not caused by a head injury, hangover or an illness such as a cold or the flu? Participants who responded yes were asked to respond to the following set of questions: Have you had at least 5 attacks (in all of your life) fulfilling the following criteria: a) Lasts a minimum of 4 hours without treatment and a maximum of 72 hours; b) Pain is predominantly on one side of the head; c) Throbbing pain; d) Moderate or severe pain intensity (which limits normal daily activities or forces you to rest); e) Pain is worsened by physical activity (like walking or walking up stairs); f) Pain is associated to nausea or vomiting; g) Pain is worsened by light or noise. In addition to a positive answer to the first screening question, women were considered to have migraine if they answered yes to a) and either f) or g), and yes to at least one of b), c), d) or e). Aura episodes were self-reported according to the following question: How frequently do you experience changes in your vision (or auras) with this painful headache?, which was made after a small introduction to this section that stated: “Auras are changes in vision, numbness or tingling in the body, that are experienced with a headache or followed by it; however, sometimes they may be experienced without any headache.” Our definition of migraine is based on the International Classification of Headache Disorders (ICDH-II) criteria (7). The questionnaire also assessed attack frequency, age at first episode, medication use and medical diagnosis.
Results
The mean age (SD) of women with migraine was 43.7 (6.9) years, while that for women without migraine was 44.4 (7.5) and for women without migraine who reported headaches the mean age was 44.2 (7.3). Overall lifetime migraine prevalence was 19% (14.1% with aura and 4.9% without aura) (Figure 1).The lifetime prevalence among women less than 30 years of age was 18% and among those 60 years and older 9.3%. The highest lifetime prevalence (20.4%) was observed among women between 40 and 44 years. Figure 2 shows the distribution of symptoms among women with migraine. The most frequent symptom was throbbing pain (91.4%), while pain worsened by physical activity was observed in only 64.7%.
Prevalence of migraine by age in Mexican women from the Mexican Teachers’ Cohort. Distribution of symptoms among Mexican women with migraine from the Mexican Teachers’ Cohort.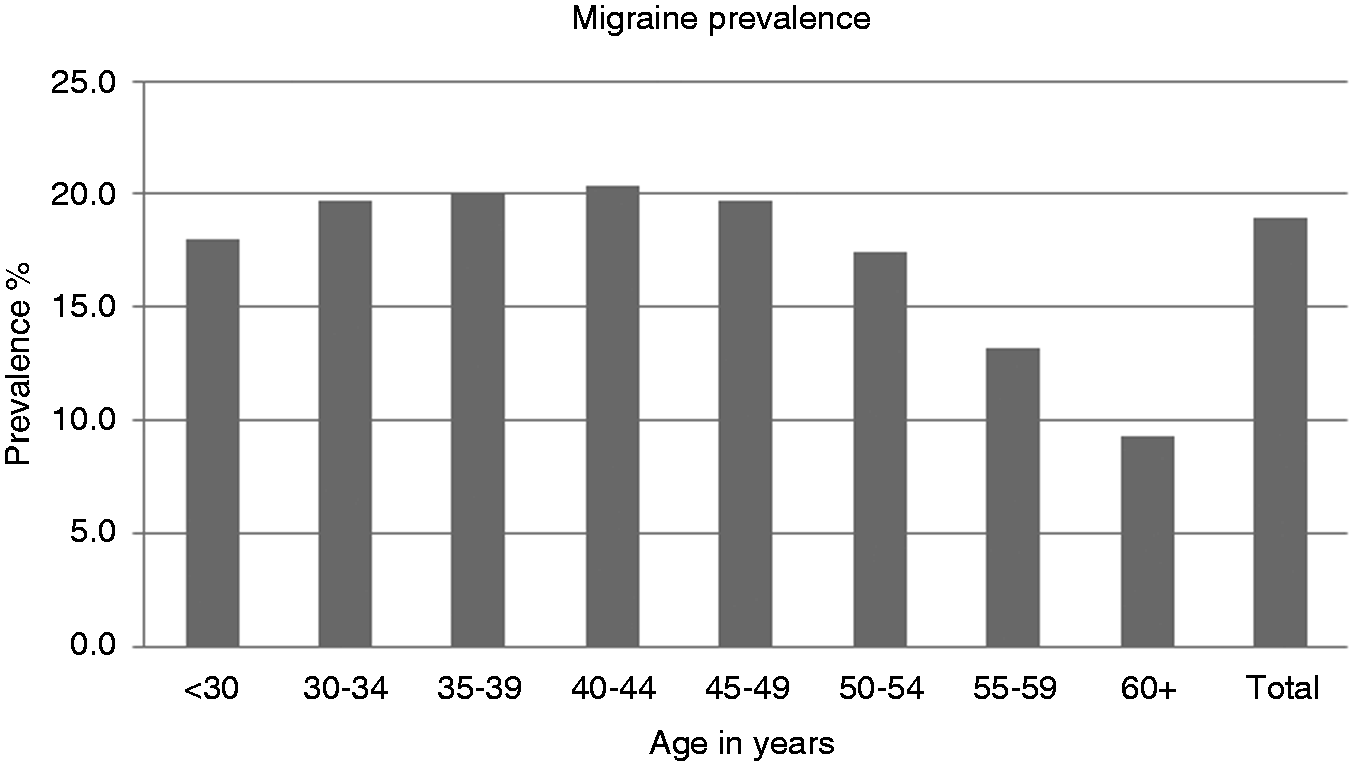

Migraine characteristics in 13,489 Mexican women from the Mexican Teachers’ Cohort.

P value: Comparison between with aura and without aura groups (chi squared test). **Aspirin, paracetamol or ibuprofen. ***Caffeine, ergotamine or sumatriptan containing medications.
Discussion
In this large population-based study of Mexican women, we observed an overall lifetime prevalence of migraine that is consistent with observations in Western populations; however, it is higher than those previously reported in Latin America. We observed a peak in migraine prevalence in women aged 40 to 44 and found that only half of women fulfilling ICHD-II criteria for migraine had a prior medical diagnosis. Women with aura appeared to be more symptomatic and received treatment more frequently than women who did not report aura.
The prevalence of migraine in our study is similar to that for European (5) and American women (8). However, this prevalence is higher than in one reported in Mexico (6). This discrepancy can be attributed in part to the differences in population characteristics, sample size, temporality and instrument used.
We observed a lifetime prevalence of migraine with aura that is higher than what has been previously reported in most (5,6,8) but not all studies. A population-based study in Iceland observed a prevalence of auras of 60% among women with migraine (9), similar to our findings. Reasons for this high frequency of migraine with aura results could be attributed to oversampling of women with migraine with aura or to difficulties in assessing aura using a self-reported questionnaire.
Lack of an appropriate diagnosis of migraine by a physician is a critical concern, and is high in the present study, in which 54.9% of women with migraines were undiagnosed. As reported in previous population-based studies (8–11), migraine is underdiagnosed and undertreated despite its considerable burden. These results provide evidence of the fact that many patients with headache characteristics consistent with migraine are not receiving an adequate treatment because diagnosis was never made.
This is one of the few studies for assessing migraine prevalence in Mexican women using ICDH-II criteria in a large population-based sample. Our study has limitations: We used a self-reported questionnaire to assess migraine that has not been validated in this population. However, good agreement of a similar self-administered questionnaire with ICHD-II criteria has been reported previously (12). Even though this is not a representative sample of the Mexican population, included women are very similar to the general female population.
Migraine is a highly prevalent and incapacitating disorder associated with several comorbidities. Understanding the burden of this disease in Mexico, addressing inadequate (under)treatment, and evaluating risk factors are essential in this understudied population for specific recommendations and prevention efforts.
Clinical implications
Estimated migraine lifetime prevalence in Mexican women is higher than those reported in previous studies in Latin America (19%). Migraine is still underdiagnosed and undertreated in Mexico despite its considerable burden; only 45.1% migraneuses had a previous diagnosis of the disease.
Footnotes
Funding
This work was supported by the Centro Nacional de Equidad y Género and Consejo Nacional de Ciencia y Tecnología (Project 161786). The funding sources had no involvement in the design, writing or the decision to submit the paper for publication.
Conflict of interest
None declared.