
Abstract
Introduction
To investigate the association of genetically predicted migraine with the risk of primary open-angle glaucoma (POAG).
Methods
To estimate the shared genetic basis of migraine and POAG, we conducted genome-wide genetic correlation analyses using cross-trait linkage disequilibrium score regression. To assess potential causal effects of migraine on POAG risk, we conducted two-sample Mendelian randomization (MR) analyses using data from European ancestry individuals. Genetic instruments (N = 54 genetic variants with minor allele frequency (MAF) ≥ 0.01) were derived from our previous genome-wide association study (GWAS) of migraine conducted in the UK Biobank (16,709 migraine cases and 438,178 controls). For POAG, we used GWAS summary statistics from our previous GWAS conducted in the GERA cohort (3836 POAG cases and 48,065 controls) or using data from the International Glaucoma Genetics Consortium (15,229 POAG cases and 177,473 controls). The inverse-variance weighted (IVW) method was our primary source of MR estimates and common sensitivity analyses were conducted.
Results
We found that migraine was not genetically associated with POAG (rg = 0.05; SE = 0.11; P = 0.69). Further, we did not detect any evidence of association between genetically predicted migraine with POAG.
Conclusion
Our results provide evidence that genetic risk for migraine may not be a strong causal risk factor for POAG.
This is a visual representation of the abstract.
Introduction
Migraine is a prevalent and disabling neurological disorder, affecting 15% of the population worldwide, 1 and imposing a substantial burden on individuals and the healthcare system. 2 Characterized by recurrent and often debilitating headaches, accompanied by symptoms such as nausea, photophobia, and phonophobia, migraine significantly impacts the quality of life of those affected. 3 The pathophysiology of migraine is complex, involving vascular and neuronal components, with both genetic4,5 and environmental factors6–8 playing a role in its etiology.
Primary open-angle glaucoma (POAG) is the most common form of glaucoma and is characterized by damage to the optic nerve and is a leading cause of irreversible vision loss worldwide.9,10 The optic nerve is responsible for transmitting visual information from the eye to the brain, and damage to this nerve can result in visual field loss and eventual blindness if left untreated. 11 Although elevated intraocular pressure (IOP) is a well-established risk factor, the pathogenesis of POAG involves additional mechanisms, including vascular dysregulation, genetic predisposition, and neurodegenerative processes.12,13 Recent studies have proposed a potential link between POAG and migraine.14–17 This link is underpinned by shared biological mechanisms, including vascular dysfunction, neuroinflammation, and genetic overlap. Specifically, individuals with migraine may experience systemic or localized vascular dysregulation, including in the ocular vasculature, increasing the risk of optic nerve damage seen in POAG.14–17
Vascular dysregulation is a critical aspect of both conditions. Migraine is associated with endothelial dysfunction, impaired blood flow, and increased vascular resistance, which are also prominent features in glaucoma. The trigeminovascular system, central to migraine pathology, influences vascular tone and blood flow, consistent with mechanisms implicated in optic nerve head ischemia in glaucoma.16,18 Furthermore, nitric oxide, a key regulator of vascular tone, has emerged as a potential molecular link. Genetic studies revealed variations in genes associated with nitric oxide-related pathways in individuals with both migraine and glaucoma, highlighting the role of altered nitric oxide metabolism and suggesting a common, potentially polygenic vascular origin for these disorders.19,20 Another potential underlying link is neuroinflammation as genome-wide association studies (GWAS) have identified inflammation-related genes associated with migraine. 5 Similarly, studies on glaucoma models and patient tissues highlight pro-inflammatory activation of retinal glia and monocyte infiltration, implicating neuroinflammation in migraine and POAG disease progression 21 22
Despite these potential pathophysiological mechanisms, epidemiological evidence regarding the migraine–POAG relationship provides mixed results. While some studies, such as the Blue Mountains Eye Study, 23 Ohn et al. 14 and Kim et al. 15 support a positive association, others, including the Beaver Dam Eye Study, 24 Panicker et al. 25 and Giloyan et al. 26 report no significant correlation. These discrepancies extend within populations, as illustrated by conflicting findings from Taiwanese cohorts.16,27 A systematic review of 11 studies revealed a statistically significant relationship between migraine and POAG, with patients suffering from migraine having a 24% higher risk of developing POAG compared to those who had never suffered from a migraine. 28 However, the true associations and underlying mechanisms remain unknown.
One of the alternatives to observational epidemiological studies is Mendelian randomization (MR) studies, where the genetic variants, robustly associated with the exposure are used as instrumental variables to estimate the causal effect of the exposure on the outcome of interest.29,30 MR studies rely on the assumption that humans are randomly assigned genetic variants from their parents during the segregation of alleles, which are not affected by environmental conditions.31–33 MR results are consistent with those of randomized controlled trials (RCTs), reduce the effect of confounding, reverse causation and various biases seen in observation studies, and can be used in cases where RCTs are not feasible or ethical.31–33
The current study aims to assess the causality in the relationship between migraine and POAG using a two-sample MR approach and GWAS summary statistics. We used results from (1) our previous GWAS of migraine conducted in the UK Biobank (UKB) cohort 34 and (2) our previous GWAS of POAG conducted in the Genetic Epidemiology Research on Adult Health and Aging (GERA) cohort. 35 To validate the initial two-sample MR findings, we performed a replication analysis using data from the International Glaucoma Genetics Consortium (IGGC) large GWAS meta-analysis of POAG 36 as the outcome.
Methods
For the GERA cohort, the Institutional Review Board of the Kaiser Foundation Research Institute approved all study procedures, and written informed consent was obtained from all participants. For the UK Biobank, this research has been conducted using the UK Biobank Resource project #14105.
Genetic correlation analyses
We assessed genetic correlations (rg), which represent a measure of single-nucleotide variation (SNV) effects genome-wide, between POAG and migraine using cross-trait linkage disequilibrium score regression. 37 For these genetic correlation analyses, we used GWAS summary statistics from: (1) our previous GWAS of migraine conducted in GERA European ancestry individuals (including 9343 migraine cases and 49,036 controls) 34 ; and (2) our previous GWAS of POAG also conducted in GERA European ancestry individuals (including 3836 POAG cases and 48,065 controls). 35
Two-sample MR analyses
Two-sample MR analyses were conducted to investigate the association of genetically predicted migraine with the risk of POAG. All analyses were performed in the R software V.4.1.2. using the TwoSampleMR package V.0.6.6. 38 This package conducts causal inference about an exposure on an outcome using GWAS summary statistics, generates LD pruning of the exposure SNVs and then harmonizes exposure and outcome datasets. We used inverse-variance weighted (IVW) method as our primary source of MR estimates. Briefly, the IVW method conducts a weighted regression of SNV-outcome effects on SNV-exposure effects where the intercept is constrained to zero. We also explored this association using a set of sensitivity MR analyses, including weighted median MR, 39 mode-based, 40 MR-Egger, 41 and MR-PRESSO. 42 We ensured that study samples for the exposure (migraine) did not overlap with those for the outcome (POAG). The conceptual framework of the current MR study is reported in Figure 1 and the different data sets used in this MR study are summarized in Supplemental Table S1.

Conceptual framework of the Mendelian randomization study.
Sensitivity analyses
We used the regression intercept from the MR-Egger method 41 to evaluate the potential effect of pleiotropy, and used the Cochran Q tests 43 to evaluate the presence of global heterogeneity amongst the effects of the genetic instruments (Supplemental Table S6). We also conducted leave-one-SNV-out analyses using the MR-Steiger method 44 to remove variants from the analysis if their association with the outcome is stronger than that with the exposure (Supplemental Table S4). 43
Genetic instruments for migraine (exposure)
Genetic association data for migraine risk (exposure) were obtained from our recent GWAS of migraine conducted in the UKB cohort. 34 The UKB is a large prospective study following the health of over 500,000 participants resident in the UK aged between 40 and 69 years at the baseline recruitment visit. Demographic information, medical history and physical and cognitive assessments were collected from each participant. Migraine cases were defined as participants with a self-reported migraine (data field 20002 code 1265) and/or a diagnosis code for migraine (International Classification of Disease, Tenth Revision [ICD-10]: G43). The control group included participants who were not cases, after excluding participants who self-reported headaches (data field 20002, code 1436) and/or who had a diagnosis code for headaches (ICD-10: G44). In total, 16,709 migraine cases and 438,178 controls from UKB participants of European ancestry were included 34 (Supplemental Table S2). For the migraine risk exposure, we identified a set of genetic instruments from lead SNVs that were previously identified as genome-wide significant (P < 5.0 × 10−8). To ensure genetic variants were independent, genetic instruments were then clumped using a 10 Mb window and maximal linkage disequilibrium of r2 = 0.001 between instruments. After clumping, a total of 54 genetic instruments for migraine risk were used for the MR analyses (Supplemental Table S3). To evaluate the strength of the genetic instruments, the proportion of variance in migraine explained by those 54 variants were calculated in the UKB European sample, using rcompanion (v2.4.36) 45 package in R v4.4.2. We found that the proportion of variance in migraine risk explained by the 54 genetic instruments in the UKB sample was 0.49%.
GWAS summary statistics for POAG (outcome)
Genetic association data for POAG risk (outcome) were obtained from our previous GWAS study conducted in the GERA cohort, which includes 110,266 adult members of the Kaiser Permanente Medical Care Plan, Northern California Region (KPNC). 35 The KPNC is an integrated healthcare delivery system that consists of ongoing longitudinal electronic health record (EHR) data.35,46,47 We retrieved genetic association data from the GWAS of POAG conducted in 3836 cases and 48,065 controls of European ancestry in GERA. 35 Briefly, patients were identified for inclusion using the KPNC EHR system of International Classification of Disease, Ninth (ICD-9) and Tenth Revision (ICD-10) diagnosis codes. Specifically, POAG cases were defined as having at least: (1) two diagnoses of POAG (ICD-9: 365.01, 365.1, 365.10, 365.11 and 365.15); or (2) two diagnoses of normal tension glaucoma (NTG; ICD-9: 365.12); or (3) one diagnosis of POAG and one diagnosis of NTG. In all POAG cases, at least one diagnosis was made by a KP ophthalmologist. Notably, POAG cases did not have any diagnosis of other glaucoma subtypes (e.g. pseudoexfoliation, pigmentary, or primary angle closure glaucoma (PACG); ICD-9: 365.52, 365.13 and 365.2, respectively). After excluding subjects who have one or more diagnoses of any type of glaucoma (ICD-9: 365.xx), our control group included all the non-cases. Subjects who had no diagnosis of any type of glaucoma (any ICD-9: 365.xx other than 365.04) but did have a diagnosis of ocular hypertension (OHTN; ICD-9: 365.04), were included as controls. In total, 3836 POAG cases and 48,065 controls from GERA participants of European ancestry were included 35 (Supplemental Table S2).
Power calculations
Statistical power calculations were conducted for the MR analyses using an online calculator 48 based on the Burgess approach, 49 at α-level of 0.05. Given a specific (outcome) sample size, the power calculation relies on the following parameters: ratio of cases to controls, the proportion of variance (R2) explained for the association between the genetic instruments and the exposure, and the “true” causal effect of the exposure on the outcome.
Replication MR analyses
As a replication of the initial two-sample MR findings, genetic association data for POAG risk (outcome) were also retrieved from the recent large GWAS meta-analysis of POAG conducted by the International Glaucoma Genetics Consortium. 36 GWAS summary statistics for this study have been publicly accessible via GWAS Catalog under study accession identifier GCST90011767 (corresponding to all European ancestry cohorts except UKB; N = 15,229 POAG cases and 177,473 controls). The same set of 54 genetic instruments for migraine was used as mentioned above.
Results
Lack of genetic determinants between migraine and POAG
To estimate the shared genetic basis of migraine and POAG, we performed genome-wide genetic correlation analyses using cross-trait linkage disequilibrium score regressions 37 in GERA European ancestry individuals. Migraine was not genetically associated with POAG (rg, 0.05; SE, 0.11; P = 0.69).
Mendelian randomization analyses do not provide evidence of causal effects of migraine on POAG
To investigate whether genetically predicted migraine was causally associated with the risk of POAG, we conducted two-sample MR analyses using, as instrumental variables for the migraine exposure, 54 established and independent SNVs from a previous GWAS conducted in the UKB European sample. 34 No significant association was found between genetically predicted migraine and POAG risk (Table 1, Figure 2 and Supplemental Figure S1 and Supplemental Tables S3 to S5).

Association of migraine-associated variants (UKB) with the risk of POAG (GERA).
MR results of the associations of genetically predicted migraine with POAG.
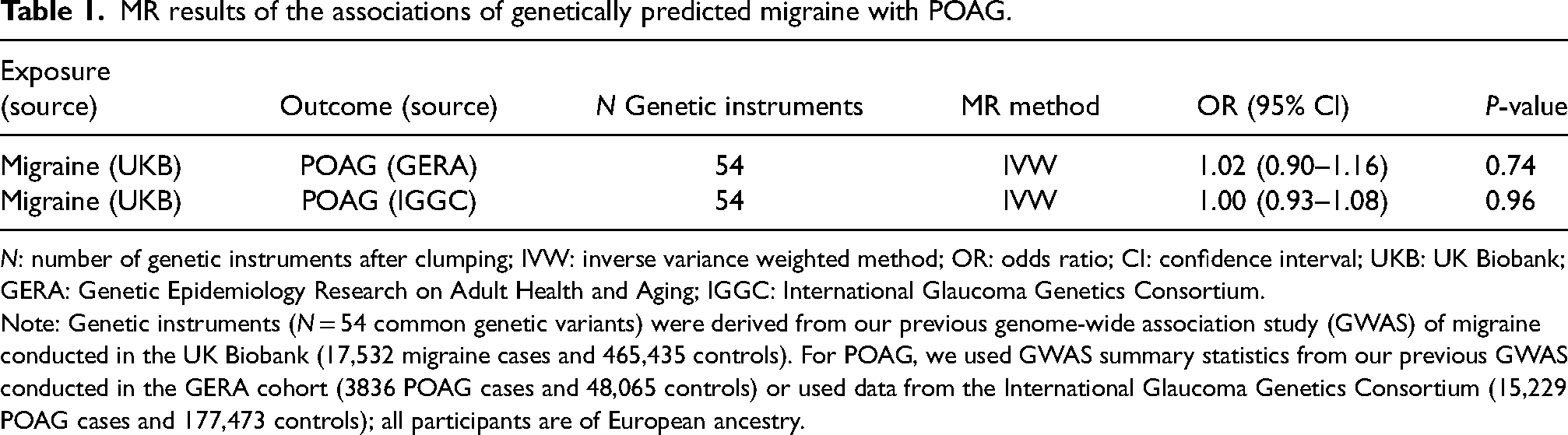
N: number of genetic instruments after clumping; IVW: inverse variance weighted method; OR: odds ratio; CI: confidence interval; UKB: UK Biobank; GERA: Genetic Epidemiology Research on Adult Health and Aging; IGGC: International Glaucoma Genetics Consortium.
Note: Genetic instruments (N = 54 common genetic variants) were derived from our previous genome-wide association study (GWAS) of migraine conducted in the UK Biobank (17,532 migraine cases and 465,435 controls). For POAG, we used GWAS summary statistics from our previous GWAS conducted in the GERA cohort (3836 POAG cases and 48,065 controls) or used data from the International Glaucoma Genetics Consortium (15,229 POAG cases and 177,473 controls); all participants are of European ancestry.
Sensitivity analyses
No evidence of directional or horizontal pleiotropy was observed for all the analyses, as indicated by MR-Egger intercept P-values greater than 0.05 (Supplemental Table S6). Further, using the Cochran's Q statistic, significant heterogeneity was observed among the effects of the genetic instruments for migraine in UKB (Q = 80.69, P = 8.44 × 10−3; Q = 104.16, P = 3.46 × 10−5; Supplemental Table S6). Since heterogeneity was detected, we conducted a MR-PRESSO model to identify potential outliers for migraine. However, we did not detect any potential outliers for migraine and POAG.
Power calculations
To calculate the statistical power for our MR analyses, we specified the IGGC sample size for POAG outcome (N = 192,702 total, including 15,229 POAG cases and 177,473 controls), and ratio of cases to controls (1:11.65), and an estimated R2 of 0.49% (UKB) for the genetic instruments based on 54 SNVs associated with migraine. We also included the true odds ratio of 1.24 for the risk of migraine in POAG patients based on a previous systematic review and meta-analysis. 28 We calculated a statistical power of 53.0% to detect the median of the range of effects.
Discussion
Despite the extensive research on migraine and POAG conducted worldwide, including genetic studies on separate cohorts or bioinformatic analyses of genetic databases, many aspects of the pathogenesis of these diseases remain unclear. To the best of our knowledge, the current study is the first investigation using genetic effect estimates to elucidate the causal association of genetically determined migraine with POAG risk. In this two-sample MR study, we did not find evidence of a causal association between migraine and POAG in European ancestry individuals.
Previous epidemiologic studies investigating the association between migraine and POAG have yielded mixed results, with some studies suggesting a connection and others finding no significant relationship. It was previously shown that patients with POAG frequently have anamnesis of conditions related to altered vascular regulation, such as migraine and cold extremities. 50 In the Blue Mountains Eye Study 23 and the Ocular Hypertension Treatment Study, 51 migraine headache was identified as a risk factor for progressive glaucomatous optic nerve damage, as well as a factor associated with fast visual field progression in patients with ocular hypertension. 52 Although results of some studies14,15,53 have suggested a positive association between migraine and POAG, others24,25,54 have not linked those two conditions. Moreover, a comprehensive meta-analysis, including 11 studies, identified a significant association between migraine and the risk of POAG and revealed a 24% higher risk of developing POAG among individuals with a history of migraine compared to those without. 28 Thus, our current MR study builds on these previous findings by using a more robust methodology to explore the potential causal relationship between migraine and POAG.
Previous research often relied on observational designs, such as cohort and case–control studies, which examined patient histories and clinical exams to find correlations and risk factors for both conditions. The major drawback of these observational studies is that they typically show associations, not direct causal links. They are also prone to various unmeasured confounders like lifestyle factors, other health conditions, and genetic predispositions, which can cloud the true nature of the relationship between migraine and POAG. To address these limitations, our study used an MR approach, leveraging genetic variants as instruments to infer causality between risk factors and outcomes, providing a clearer picture of the potential causal links. By analyzing summary statistics from large-scale GWAS for both migraine and POAG, we were able to investigate the genetic overlap and possible causal pathways between these conditions with greater accuracy and reliability.
It is possible that the lack of a clear link in the current study may be attributed to certain limitations. First, the definition used to identify migraine cases and controls in UK Biobank could represent a limitation –as mainly based on self-reported data and participants with headaches diagnosis were excluded from the control group—and its reliability could be considered modest. However, our previous GWAS meta-analysis 34 combining GERA and UKB results demonstrated consistency of the SNVs effect estimates between cohorts. Similarly, associations previously reported by the International Headache Genetics Consortium 55 were well validated in our previous GWAS meta-analysis. Second, in this study, the statistical power to detect an association between migraine and POAG could have been limited due to the limited proportion of variance explained by the 54 genetic instruments associated with migraine, the small number of genetic variants with a MAF threshold of >0.01, or residual confounding due to unmeasured factors due to the nature of using summarized data. Future studies would benefit from the use of individualized data in large sample sizes to conduct analyses in subgroups or strata of populations, or to adjust for relevant confounders. 43 Third, our analyses were restricted to individuals of European ancestry, and therefore, the results may not be applicable to other populations. Future investigations may examine the causal association between migraine and POAG in non-European ancestries as those genetic data become available. We acknowledge that the results of our MR study are potentially biased by pleiotropy, especially as recent studies56,57 have shown existing MR study methods are ineffective for detecting and accounting for horizontal pleiotropy under some conditions. Future studies that may detect a significant association between migraine and POAG could assess underlying biological mechanisms by conducting probabilistic MR methods (i.e. PMR-Egger, MRAID, or MR-MtRobin) that leverage horizontal pleiotropy to identify putatively causal genes, proteins and pathways.58–61
In addition, we were unable to examine specific subtypes of POAG, such as normal-tension glaucoma, due to a lack of adequately powered GWAS for these subtypes. The same limitation applies to subtypes of migraine, especially since migraine is a rather heterogeneous nosology. Given that more pronounced neuroinflammatory reactions occur in the chronic form of the disease, and that chronic and severe migraine is associated with a greater risk of developing POAG 14 ; investigating the effect of chronic migraine on glaucoma may warrant further investigation.
This study has notable strengths, including the use of instrumental variable methods such as MR, which emulates RCTs as both utilize the power of randomization to provide unconfounded causal effect estimates that are not subject to reverse causation and other various biases. 33 However, the validity of MR relies on a series of assumptions that are challenging, if not impossible, to test. Furthermore, the use of independent GWAS summary statistics from large study samples for both the exposure and the outcome provided strong genetic instruments and statistical power to detect modest causal effects.
Conclusion
In conclusion, using genetic correlation analyses, our study did not detect evidence of genetic correlation between migraine and POAG. Further, using a two-sample MR analysis, our study did not detect any evidence of causal association between genetically predicted migraine and the risk of POAG in European ancestry individuals. As such, considering that research between migraine and POAG has yielded mixed results so far, our findings do not support that genetic risk for migraine is a causal risk factor for POAG.
Key findings
Our study did not detect evidence of a genetic correlation between migraine and POAG in European ancestry individuals.
Our findings does not support that genetic risk for migraine is a causal risk factor for POAG.
Supplemental Material
sj-docx-1-rep-10.1177_25158163251323245 - Supplemental material for Association between migraine and primary open-angle glaucoma: A two-sample Mendelian randomization study
Supplemental material, sj-docx-1-rep-10.1177_25158163251323245 for Association between migraine and primary open-angle glaucoma: A two-sample Mendelian randomization study by Dima L Chaar, Aliya Yakubova, Chen Jiang, Thomas J Hoffmann, Alice Pressman, Denis Plotnikov and Hélène Choquet in Cephalalgia Reports
Footnotes
Acknowledgements
We are grateful to the Kaiser Permanente Northern California members who have generously agreed to participate in the Kaiser Permanente Research Program on Genes, Environment, and Health. Support for participant enrollment, survey completion, and biospecimen collection for the RPGEH was provided by the Robert Wood Johnson Foundation, the Wayne and Gladys Valley Foundation, the Ellison Medical Foundation, and Kaiser Permanente Community Benefit Programs. Genotyping of the GERA cohort was funded by a grant from the National Institute on Aging, National Institute of Mental Health, and National Institute of Health Common Fund (RC2 AG036607).
Author contributions
Concept and design: H.C., D.P.; Acquisition, analysis or interpretation of data: H.C., D.C., C.J., T.J.H., Drafting of the manuscript: D.C., A.Y., D.P., H.C.; Statistical analysis: C.J.; Obtained funding: H.C.; Administrative, technical or material support: H.C., D.P., A.P.; Supervision: H.C.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
For the GERA cohort, the Institutional Review Board of the Kaiser Foundation Research Institute approved all study procedures, and written informed consent was obtained from all participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: H.C. was supported by the National Eye Institute (NEI) grants R01 EY027004 and R01 EY033010. A.R.P. was supported by the National Institute of Neurological Disorders and Stroke (NINDS) grant R01 NS080863. A.Y. was supported by the Kazan Federal University Strategic Academic Leadership Program (PRIORITY-2030). D.P. was supported by a grant from the Academy of Sciences of the Republic of Tatarstan for postdoctoral fellows (№ 135/2024).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.