
Abstract
Background
Medication overuse headache (MOH) presents a considerable challenge in patient care, with physicians playing a critical role in its prevention and management. However, awareness, knowledge, and practices regarding MOH among physicians are often found to be inadequate.
Methods
A cross-sectional study was conducted at King Chulalongkorn Memorial Hospital to investigate the awareness, knowledge, and practices concerning MOH among residents from family medicine, internal medicine, and neurology specialties. Participants were surveyed using an internet-based questionnaire.
Results
Of the 130 residents, 70 participated in the study. Ten percent were unaware that analgesics could exacerbate headaches, a finding particularly notable among family medicine residents. Furthermore, 11.4% of participants were uncertain about the classification of MOH, while 31.4% and 44.3% were uncertain about the frequency with which the use of simple analgesics and migraine-specific drugs could lead to MOH, respectively. This uncertainty was prevalent among residents in internal medicine and family medicine. Additionally, 22.9% of participants, especially those in internal medicine, prescribed opioids for abortive treatment in migraine patients. Residents in neurology generally performed better across various aspects compared to those in other specialties.
Conclusion
The study highlights a significant gap in the awareness, knowledge, and practices regarding MOH, particularly in non-neurology residency programs. Addressing these issues may require continuous medical education utilizing a multifaceted approach, encompassing undergraduate courses, postgraduate training, and public outreach.
Introduction
Medication overuse headache (MOH) is a chronic headache disorder categorized within secondary headaches. Diagnosis depends on a history of headaches for 15 or more days monthly for three months, coupled with documented overuses of abortive medications. Specifically, paracetamol or NSAIDs are used on 15 or more days monthly, and ergot, triptans, opioids, or combined analgesics are used on 10 or more days monthly. 1 These overuses exacerbate headaches in individuals with underlying headache disorders, typically migraine and/or tension-type headaches. The global prevalence among adults’ ranges from 1–2%, varying by country and study methodology. 2 The 2013 Global Burden of Disease study estimated 63 million cases of MOH worldwide. 3 MOH significantly affects patients’ lives, contributing to disability. The Eurolight study estimated the annual cost of MOH in 2011 at €37 billion, with 92% attributed to lost productivity. 4 Consequently, MOH is a major concern in headache patient care, necessitating a pivotal role for physicians in prevention and management through patient education.
Physicians’ awareness and knowledge are critical for the prevention of MOH. However, headache education for physicians remains insufficient. 5 Resident training programs play a crucial role in enhancing the quality of headache care. The study investigates awareness, knowledge, and practices about MOH among resident doctors in our university hospital through an internet-based questionnaire. Additionally, our secondary goal is to evaluate factors that influence participants’ awareness, knowledge, and practices concerning MOH, including specialty training programs, gender, age, and the duration of practice post-M.D. graduation.
Methods
This cross-sectional study investigated awareness, knowledge, and practices regarding MOH among resident doctors at King Chulalongkorn Memorial Hospital (KCMH), The Thai Red Cross Society, Bangkok, Thailand. We surveyed 130 participants, including residents from the specialties of family medicine, internal medicine, and neurology. The internet-based survey was administered using a Google Forms questionnaire, which was distributed publicly through the department's announcement system, including department conferences, and via email to residents, allowing for voluntary and anonymous participation. Data were collected from the responses submitted via Google Forms during survey period. Informed consent was obtained from all willing participants. The study received approval from the Institutional Review Board Research Ethics Committee of the Faculty of Medicine, Chulalongkorn University, Bangkok, and KCMH in February 2023 (IRB number 009/2023). Data collection was conducted from February to April 2023, with each participant permitted only one response.
The questionnaire, developed in Thai, comprised 13 multiple-choice questions on MOH awareness, knowledge, and practices (Supplementary Material 1). Questions on awareness asked whether analgesic drugs could cause headaches. Knowledge-based questions covered types of headaches as defined by the ICHD-3, 6 frequency of analgesic use leading to MOH, indications for migraine prophylaxis, and MOH diagnosis and treatment strategies. Practice-related questions explored the types and numbers of prescribed analgesics, patterns of prescribing abortive medications, inquiries about headache frequency and analgesic usage, and advice on maintaining headache diaries. De-identified demographic data, including age, gender, residency program, and post-M.D. graduation practice duration were also collected.
Continuous data were presented as the median and inter-quartile range (IQR). Categorical data are shown as numbers and percentages. Pearson's chi-squared test (X2) analyzed associations in categorical data. Normality was tested using visualized histograms and the Shapiro-Wilk test. The statistical significance was set at 0.05 with the two-tailed hypothesis. All statistical analyses were performed using IBM SPSS statistics version 29.0.
Results
Out of 130 resident doctors, 70 participated in the study, resulting in a 53.8% response rate. Of these participants, 24 (34.3%) were from neurology, 24 (34.3%) from internal medicine, and 22 (31.4%) from family medicine. Among the respondents, 50% were male, with a median age (IQR) of 31 (29–31) years and a median number of years since graduation (IQR) of 6 (4.25–7.75). Demographic data were presented in Table 1.
Demographics of questionnaire responders.

Awareness
Regarding awareness of MOH, 10% of residents were unaware that analgesic drugs could worsen headaches. Family medicine residents demonstrated a significantly higher proportion of unawareness (31.8%) compared to other specialties (X2 = 16.97, p = 0.02) (Figure 1(a)).

Distribution of MOH awareness among different residency training programs (in percentages). (a) Illustrates the variability in awareness of MOH, (b) illustrates awareness/knowledge of the use of Acetaminophen or NSAIDs for ≥15 days per month potentially resulting in MOH, and (c) illustrates awareness/knowledge of the use of ergotamine, triptans, or opioids for ≥10 days per month potentially resulting in MOH.
Knowledge
Regarding MOH knowledge, 11.4% were uncertain about its classification according to the ICHD-3 and 14.3% incorrectly identified MOH as a primary headache. Furthermore, 22 residents (31.4%) demonstrated uncertainty or provided incorrect responses concerning the number of simple analgesic drugs (acetaminophen, NSAIDs) that could potentially cause MOH. Notably, residents from family medicine (10 residents, 45.5%) and internal medicine (9 residents, 37.5%) were significantly more uncertain about these numbers compared with their counterparts in neurology (3 residents, 12.5%) (Figure 1(b)). Similarly, 31 residents (44.3%) were either uncertain or provided incorrect answers regarding the frequency of ergots, triptans, or opioids use leading to MOH. Residents in family medicine (12 residents, 63.6%) and internal medicine (12 residents, 50.0%) exhibited significantly more uncertainty about these figures compared to their counterparts in neurology (5 residents, 20.8%) (X2 = 14.47, p = 0.025) (Figure 1(c)).
Respondents who disagreed with each indication for initiating migraine prophylactic agent include 10.0% for having at least 4 migraine days per month; 8.6% for headaches that cause significant disability; 28.6% for the patient who develops or is at risk of MOH; 28.6% for the patient with disabling migraine auras such as hemiplegic migraine or brainstem aura; and 44.3% for the patient contraindicated to or experiencing side effects arose from analgesic drugs.
In a case scenario representing chronic migraine with MOH, 51.4% of respondents incorrectly identified the condition as either chronic migraine or MOH. Concerning MOH treatment, 11.4% of residents suggested starting proper preventive medication, 2.9% proposed switching to another analgesic, and 85.7% recommended discontinuing the culprit analgesic and starting appropriate prophylactic medication.
Practice
Regarding practice among headache patients, 58.6% of respondents never recommended headache diaries for patient follow-up. Neurology residents (n = 18, 75%) were significantly more likely to endorse headache diaries compared to other specialists (X² = 18.04, p < 0.01) (Figure 2(a)). Additionally, 32.9% of respondents occasionally asked patients about headache frequency, 5.7% never inquired, while 61.4% consistently asked. Neurology residents (n = 22, 91.7%) significantly outperformed other specialists in regularly exploring headache frequency (χ² = 15.87, p = 0.003) (X² = 15.87, p = 0.003) (Figure 2(b)).
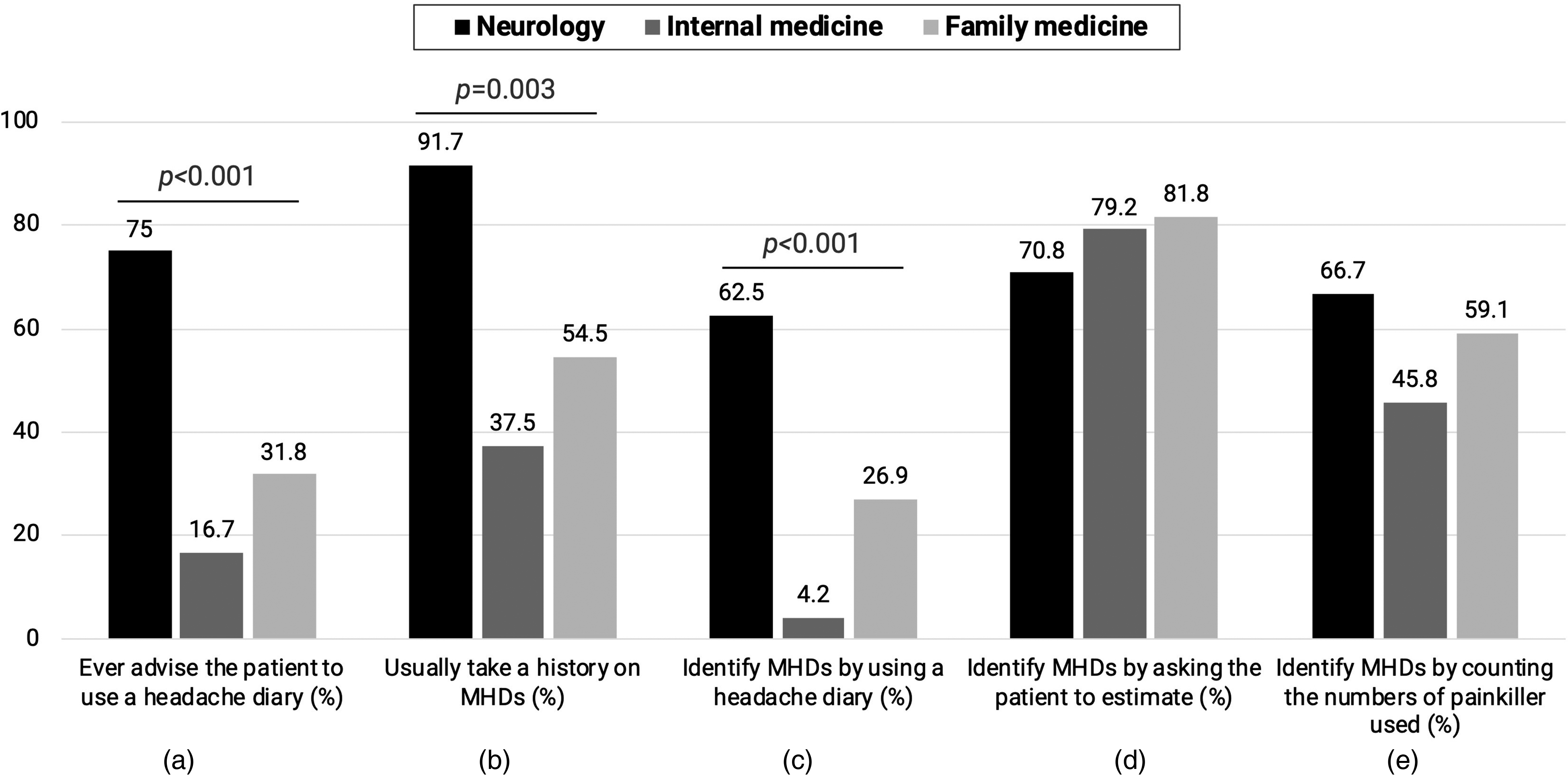
Residency training program perspectives on headache-related practices (in percentages). (a) Illustrates the prevalence of advising patients to use a headache diary, (b) illustrates the inquiry frequency about headache occurrence, and (c), (d), and (e) delineate different methods for assessing headache frequency. These methods include the use of headache diaries, asking patients to estimate their headache frequency, and utilizing abortive medication consumption as an indicator, respectively.
For assessing headache frequency, 30.0% of respondents utilized headache diaries (Figure 2(c)), 77.1% asked patients to estimate it (Figure 2(d)), and 57.1% used the consumption of abortive medication as an indirect measure (Figure 2(e)). Neurology residents (n = 15, 62.5%) significantly preferred the use of headache diaries over other specialties (X² = 20.25, p < 0.001) (Figure 2(c)).
Prescription habits for analgesic medications (Figure 3) revealed that 87.1% of respondents prescribed acetaminophen, 92.9% prescribed NSAIDs, 34.3% prescribed triptans, 10% prescribed ergots, and 22.9% prescribed opioids. Neurologists prescribed triptans significantly more often than other specialists (X² = 14.95, p < 0.001) (Figure 3(c)). NSAIDs were frequently prescribed by neurology (n = 24, 100%) and family medicine (n = 21, 95.5%) compared to internal medicine residents (n = 20, 83.3%) (Figure 3(b)), although the difference was not statistically significant (χ² = 5.352, p = 0.069). Conversely, internal medicine residents prescribed opioids more frequently than other specialists (X² = 7.959, p = 0.019) (Figure 3(e)).

Proportion of abortive medication prescriptions within each residency training program: (a) Acetaminophen, (b) NSAIDs, (c) triptans, (d) ergotamine, (e) opioids.
Regarding recommendations for abortive medication, 82.9% of respondents advised initiating treatment at headache onset, 7.1% recommended adherence to drug labels, and 10% suggested use before onset. Prescribing approaches varied: 68.6% prescribed a specific amount to prevent MOH, 14.3% based their prescriptions on the appointment day, 12.9% tailored them to patient requests, and 4.3% offered alternative strategies, such as limiting prescriptions to around 20 pills per month.
Additionally, we analyzed other factors influencing our secondary goal including age, sex, and duration of practice post-M.D. graduation and found that they were not associated with awareness, knowledge, and practice of MOH (data not shown).
Discussion
MOH presents a significant challenge among headache patients, where physicians play a crucial role in prevention and treatment. One important issue is the inadequate headache education among physicians. According to a survey by the American Headache Society (AHS), medical students receive on average only one hour of preclinical instruction and two hours of clinical instruction related to headache medicine. 7 As specialists in internal medicine, family medicine, and neurology are primarily responsible for treating headache patients, integrating headache knowledge and practices into such residency training programs is essential for addressing the MOH issue. However, our study has identified persistent gaps in awareness, knowledge, and practice among resident doctors in these specialties.
Awareness
Our population demonstrated MOH awareness in 90% of resident doctors, which appears to be higher than in other studies. A study conducted at Dokuz Eylul University's health campus in Turkey found that only 51% of doctors were aware of MOH, 8 while a study at the University of Birmingham reported a 38% awareness among healthcare-educated individuals. 9 A survey of French neurology residents revealed that 74.4% were aware of MOH in headache patients. 10 The heightened awareness in our study can be partly attributed to one-third of the participants being from neurology residency programs. Additionally, the issue of MOH is increasingly recognized as significant among healthcare personnel.
Knowledge
Approximately half of the non-neurology residents and about 15% of neurology residents demonstrated insufficient knowledge about MOH, particularly regarding the number of analgesic drugs posing risks for MOH. This discrepancy in knowledge may be linked to variations in headache education across different residency training programs. At our medical school, neurology residents possess more extensive knowledge about MOH due to a mandatory one-month clinical rotation at an outpatient headache service during their third or final year of training. Additionally, they receive around 10 h of mandatory lecture-based headache education annually and benefit from daily bedside teaching provided by five neurologists specializing in headaches at our university. This educational approach is consistent with the results of a 2015 U.S. survey, which found that 97% of program directors believe that at least two weeks of clinical exposure to headache is adequate for a neurology residency training program, and 72% agreed that more than five hours of lectures are sufficient for training. 11 In contrast, internal medicine and family medicine residents at our medical school attend only one session of clinical observation at the outpatient headache service and receive just one hour of lecture-based education throughout their three-year training period. The estimated formal education on headache is only about 1–2 h throughout the training. A 2005 survey at U.S. medical schools indicated differences in headache education across residency training programs: two-thirds of neurology programs provide more than five hours of lecture-based headache education, compared with only one-third of family medicine programs. Despite this, over 85% of program directors from both specialties consider these educational plans sufficient for the care of headache patients, though this adequacy is questionable. 12
Practice
Our survey highlighted some potential practice trends contributing to MOH, including opioid prescriptions, particularly by internal medicine residents. This trend may be attributed to concerns about potential NSAID side effects, such as renal toxicity, gastrointestinal issues, and cardiovascular events, combined with a lack of awareness among internal medicine residents regarding the link between opioid use and headache chronification. 13 Meanwhile, a high proportion of triptan prescriptions was observed among neurology residents. In our country, triptans can only be prescribed with approval from board-certified neurologists, due to cost-effectiveness considerations. This restriction might reflect the underutilization of effective migraine-specific treatments among non-neurologists.14,15
Our study revealed that only a low proportion of residents based the number of prescribed analgesics on the appointment day or tailored it to patient requests. Nevertheless, this practice of overprescribing analgesic medication should still be addressed, as it significantly contributes to the risk of developing MOH. A study in Japan found that 9.2% of patients were overprescribed acute medications, with a trend of increasing overprescription rates among patients who had a persisting headache diagnosis two years after their initial diagnosis. 16 This issue could potentially be mitigated by enhancing awareness and knowledge of MOH and by utilizing healthcare resources more effectively. Such resources could include electronic prescription programs and comprehensive multidisciplinary care involving trained pharmacists or nurses at headache clinics.
Despite important findings, our study faced limitations. First, this study involves a small population limited to neurology, internal medicine, and family medicine residents at King Chulalongkorn Memorial Hospital, who only interacted with headache patients in the outpatient department. The results might differ in other populations and at other universities. We plan to extend the survey to other universities and include other subspecialties such as emergency medicine, which frequently encounters with MOH patients in emergency rooms. Secondly, we observed a low response rate of 30.4% (24/79) from internal medicine, while neurology had a 100% response rate (24/24), and family medicine had 81.5% (22/27). Given the relatively larger number of internal medicine residents, the department's announcement system may not be thorough enough to reach all potential respondents. Additionally, due to their high workload, there may be limited cooperation from internal medicine residents.
To address the issues of MOH among resident doctors, we propose three strategic focuses: amplifying awareness, enhancing educational content, and preventing malpractise related to MOH. First, we plan to launch a comprehensive awareness campaign targeted at both healthcare professionals and patients to improve understanding and management of MOH including society education via social media. 17 Second, we advocate for a significant revision of the medical curriculum related to headache disorders, from medical school through to residency training. This revision includes an increase in dedicated instructional hours on headache management, integration of practical case studies, and the provision of hands-on training opportunities. We recommend incorporating active learning sessions such as Team-Based Learning (TBL) and case discussions for medical students. Postgraduate programs should dedicate lectures to MOH topics and facilitate real patient encounters at headache clinics. Finally, we suggest improvements in the healthcare system to help prevent MOH, for example, by restricting the number of abortive medications prescribed to patients, particularly opioids, through electronic medical records, laws, regulations, guidelines, and policies.18,19 By implementing these measures, we aim to cultivate a healthcare workforce that is not only more knowledgeable and skilled in addressing MOH but also capable of significantly reducing malpractise instances, thereby enhancing patient care and outcomes in headache disorders.
Conclusion
This study revealed that while resident physicians demonstrate a heightened awareness of MOH, their knowledge remains limited and certain practices may jeopardize MOH patients. Subspecialty training programs are crucial in influencing awareness, knowledge, and practices related to MOH. Neurology resident training programs demonstrate greater awareness, knowledge, and practice regarding MOH compared to other specialties. In contrast, family medicine residents show lesser awareness and knowledge, and internal medicine residents may engage in practices that pose risks to MOH patients. To correct these misconceptions, continuous medical education extending beyond neurology is essential. Such education should encompass undergraduate courses that feature active learning sessions, postgraduate experiences with direct patient encounters in headache clinics, and public outreach initiatives, including awareness campaigns, societal education via social media, and professional community engagements. These efforts are vital for improving patient health outcomes and alleviating the burden on the healthcare system.
Public health relevance
Awareness, knowledge, and practices concerning MOH remain problematic among resident training programs, especially in non-neurology programs.
The number of lecture hours and practical sessions dedicated to headaches may significantly influence the successful understanding of MOH.
The study highlights the necessity for enhanced headache education across all medical specialties to improve MOH management and patient outcomes, advocating for a comprehensive approach to training, the importance of continuous medical education, and public awareness campaigns.
Supplemental Material
sj-docx-1-rep-10.1177_25158163241266948 - Supplemental material for Awareness, knowledge, and practice towards medication overuse headache in Thailand: A university hospital-based survey in residency training programs
Supplemental material, sj-docx-1-rep-10.1177_25158163241266948 for Awareness, knowledge, and practice towards medication overuse headache in Thailand: A university hospital-based survey in residency training programs by Prakit Anukoolwittaya, Thanakit Pongpitakmetha, Akarin Hiransuthikul, Sekh Thanprasertsuk and Wanakorn Rattanawong in Cephalalgia Reports
Footnotes
Abbreviations
Acknowledgments
We extend our gratitude to the residents in the family medicine, internal medicine, and neurology training programs for their valuable responses to our surveys. We also acknowledge ChatGPT-4, OpenAI in San Francisco, CA, USA, for its assistance in constructing and language editing the manuscript submitted for publication. Authors read and had final approval for the intellectual content after language editing by ChatGPT-4.
Author contribution
PA and TP acquired the data, created the figure, and drafted the manuscript for intellectual content. AH analyzed and interpreted of data. ST created the figure and revised the manuscript for intellectual content. WR acquired the data and revised the manuscript for intellectual content. All authors designed and conceptualized the study.
Data availability
The original data was kept with the corresponding author and data could be shared upon request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Approval was obtained from the ethics committee of Chulalongkorn University (IRB no. 009/2023). The procedures used in this study adhere to the tenets of the Declaration of Helsinki. Informed consent was obtained at time of answering the questionnaire.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.