
Abstract
Abstract
Objective
To estimate the prevalence and burden of medication overuse headache in a representative sample of the Greek population, aged 18–70 years old.
Methods
This is a cross-sectional descriptive observational study performed by quantitative computer-assisted telephone interviews, using a standardized 37-item questionnaire for headaches. The prevalence of medication overuse headache was estimated in the general population and compared within the groups formed by factors such as age, gender, diagnosis of headache type, prophylactic treatment used, geographical regions, social class, workdays lost and loss of productivity.
Results
1197 (12.0%) participants reported headaches affecting performance out of 10,008 interviewees. The estimated prevalence of medication overuse headache in the general population was 0.7% (95% CI: 0.5–0.9). The female to male ratio was 3.6:1. The proportion of medication overuse headache was largest in the 35–54 age group, followed by the over 55 group. The Aegean islands and Crete were the regions with the highest proportion of medication overuse headache. Among participants with headaches, the proportion of medication overuse headache was 5.8% (95% CI: 4.4%–7.1%); 6.3% (95% CI: 4.7%–7.9%) among females and 4.4% (95% CI: 2.2%–6.6%) among males. In the same headache group, the proportion of medication overuse headache by prophylactic treatment for headache was 19.0% (95% CI: 9.5%–29.1%) for recipients and 5.0% (95% CI: 3.8–6.3) for non-recipients. The mean absenteeism in people with medication overuse headache was 1.0 days/month (95% CI: 0.4–1.6) and the mean presenteeism 6.3 days/month (95% CI: 3.9–8.7). The social class stratification showed a significant effect between the medication overuse headache in the sample of the general population and the C2 class, corresponding to skilled manual labour (OR: 0.7, CI: 0.5–0.9). In people with chronic migraine, and chronic tension type headache, as differentiated by the 37-item questionnaire, the proportion of medication overuse headache in the headache group estimated to be 50.5% (95% CI: 40.8%–60.1%) and 45.9%, (95% CI: 29.9%–62.0%) respectively. The group of people with acute headache medication overuse fulfilling the rest of the diagnostic criteria for medication overuse headache, except from the number of headache days per month (≥15 days/month), had a prevalence of 2.0% (95% CI: 1.75–2.30) and a proportion of 17.0% (95% CI: 14.8%–19.1%) among people with headache. In the episodic types of headache, the proportion of acute headache medication overuse was higher in the subgroup of people with high frequency episodic migraine, 24.9% (95% CI: 18.8%–31.0%), while it was 10.8% (95% CI: 8.2%–13.5%), for the low frequency episodic migraine and 8.5% (95% CI: 5.5%–10.4%), for the episodic tension type headache.
Conclusion
The prevalence of medication overuse headache in the general population in Greece and its proportion among the people with headache belongs to the lower part of the range of the reported literature, while the 3.6:1 female to male ratio is in agreement with it. In the same line, the impact of absenteeism and presenteeism on the workplace renders the condition alarming socio-economic health problem demanding immediate health policy planning.
Keywords
Introduction
Medication overuse headache (MOH) is defined by the diagnostic criteria of ICHD-3 (1), as a chronic headache, designated by ≥15 headache days/month (d/m), in a patient with a pre-existing headache disorder, lasting for more than three months and accompanied by the use of pain relief medications for the acute headache pain, for 15 d/m or more (for common analgesics and non-steroidal anti-inflammatory drugs, NSAIDS) and 10 d/m or more for the other acute treatment medication classes (triptans, ergots, opioids etc). The exclusion of any other headache disorder is also a prerequisite. These diagnostic criteria do not include any specific clinical phenotype related to MOH nor its remittance after analgesic withdrawal. Thus, the current definition of MOH, facilitates its concurrent diagnosis, along with the pre-existing headache, if the above-mentioned cut-offs of headache days and pain relief medications are fulfilled, aiding the clinician to plan a management strategy (2–3). There is compelling evidence for the relationship of acute headache medication overuse (AHMO) and MOH, on a group level, by multiple prospective studies (4–7). The odds ratio for developing chronic headache are as high as 19.4 in a group of people with episodic headache and AHMO compared to a similar group without it (7).
MOH causes substantial disability. It has been ranked 20th among all medical conditions in terms of years lived with disability (YLDs) (8). Furthermore, the mean annual cost per person in Europe has been calculated as being three times more than migraine and ten times more than tension type headache (TTH) (9). The enormous health and financial consequences of MOH make its management a high priority (10–12).
In the present study we aimed to post-hoc calculate the prevalence of people with disabling headaches and MOH in Greece using the raw data of a national epidemiological survey conducted in 2017 (13).
Methods
The present study is part of a larger cross-sectional descriptive epidemiological survey, concerning the prevalence, burden, and treatment preferences of headaches in Greece in 2017. The STROND (Standards of Reporting of Neurological Disorders) checklist has been completed according to the guideline for the reporting of incidence and prevalence studies in neuroepidemiology. The methodology of the survey is outlined in detail elsewhere (13). In summary, we randomly selected a phone number out of a large database of 97,803 phone numbers, aiming to interview the 1.4‰ of the total population, corresponding to approximately 10,000 interviewees. This database was representative of the Greek population, in terms of gender, age and geographical region, based on the latest census. Subsequently, we used stratified random sampling, creating subgroups according to the gender, age and geographical region, directly proportional to the same subgroup of the general population. During the random sampling process, the respondents were asked to state their age, gender, and region. As long as the survey was proceeding, and quotas were successively completed, we kept looking for respondents with demographic characteristics matching only the still incomplete quotas. If, for instance, at some point of the ongoing survey, the target number was reached for females but not for males, fieldwork continued but if a woman answered, the interview stopped when she informed the interviewer about her gender. In such cases, the interviewer asked if anyone else was in the house, who could possibly take part in the survey (without specifying gender/age requirements) (13). Thus, randomization was achieved, as assessed by crosstabulation of gender by age groups (Table 1, Online Supplemental Material 1) and subsequent comparison to the similar table (Table 2, Online Supplemental Material 1), constructed by the Hellenic Statistical Authority (ELSTAT), during the last census in 2011 (14). Thus, there was no additional need for poststratification (Figure 1). Each subgroup was interviewed with the use of a previously standardized questionnaire. The screening question was: “Do you suffer from headaches that affect your performance and which occurred at least once in the year prior to this survey?”. The ICHD-3 beta diagnostic criteria were used, during the standardization procedure, for the comparison of the clinical diagnosis made by headache experts to the results of the completed questionnaire (13), as well as for the diagnosis of MOH. The sensitivity and specificity of the questionnaire for migraine/probable migraine were calculated to be 90.1% and 60.0%, for tension type headache (TTH)/probable TTH 94.3% and 42.9%, and for cluster headache/probable cluster headache 92.4 and 74.6% respectively; positive predictive values were 91.9%, 42.9% and 89.8%, respectively. Such values are not available for MOH and AHMO.
Proportion of MOH in the sample of the general population (N = 10,008), by gender, age and geographical region.
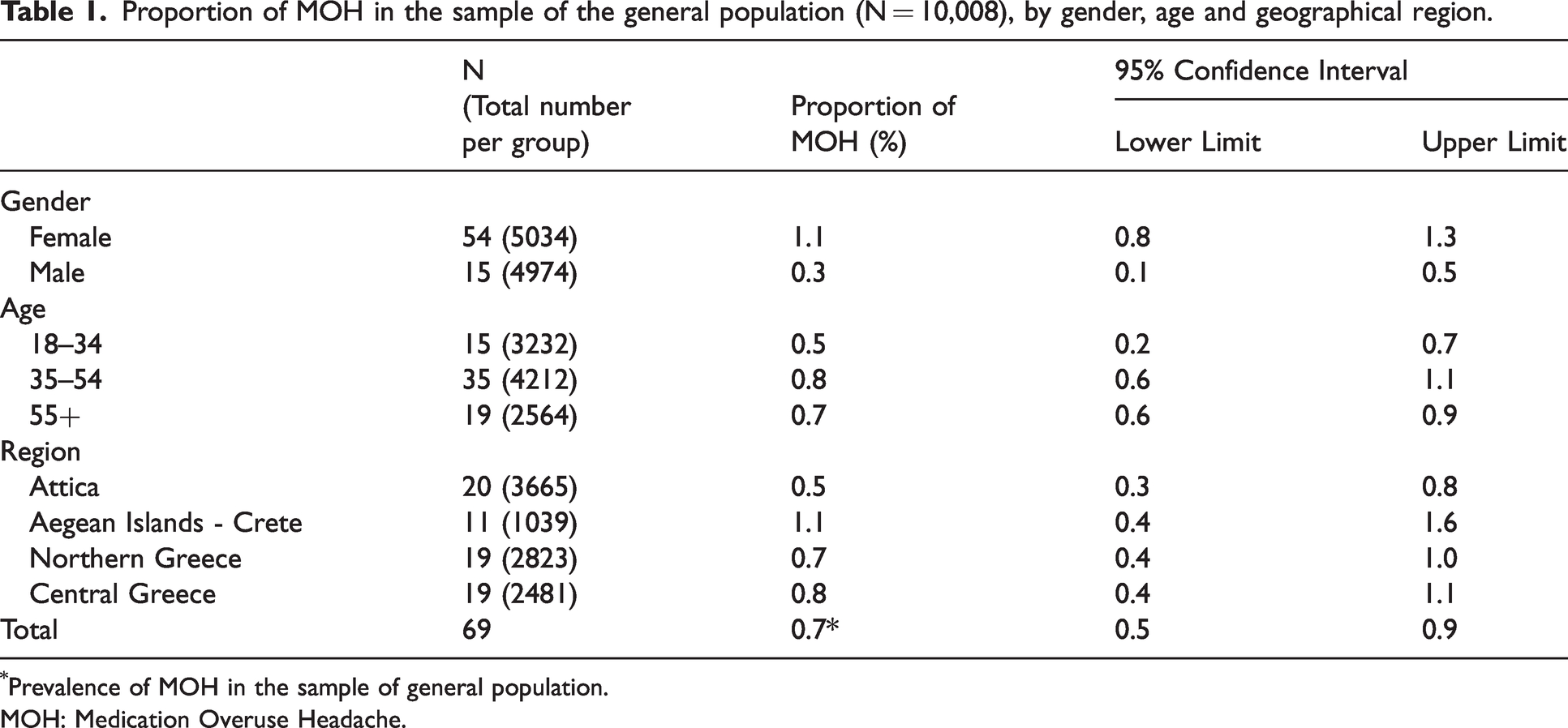
Prevalence of MOH in the sample of general population.
MOH: Medication Overuse Headache.
Logistic regression table. Dependent variable: MOH in the sample of the general population (N = 10,008).
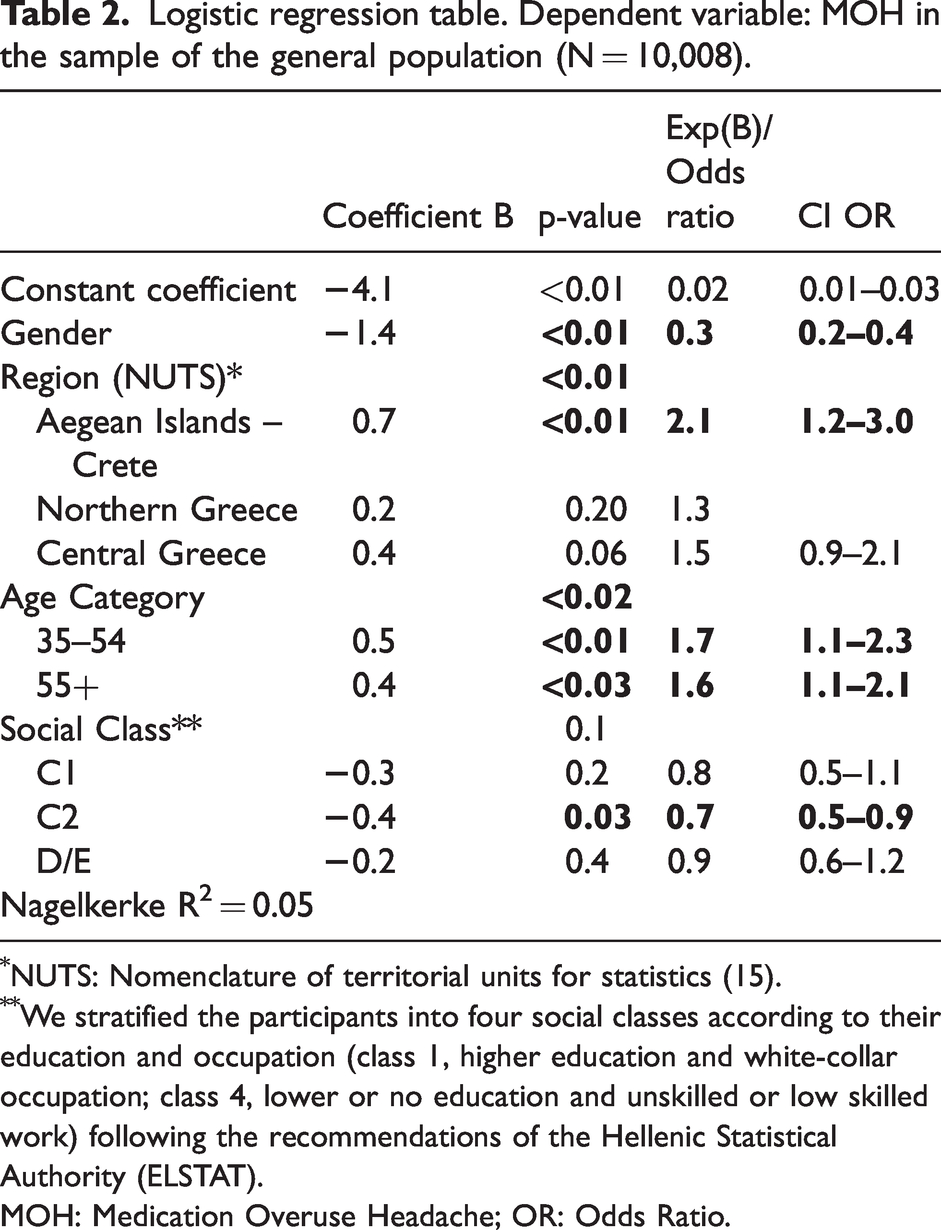
NUTS: Nomenclature of territorial units for statistics (15).
We stratified the participants into four social classes according to their education and occupation (class 1, higher education and white-collar occupation; class 4, lower or no education and unskilled or low skilled work) following the recommendations of the Hellenic Statistical Authority (ELSTAT).
MOH: Medication Overuse Headache; OR: Odds Ratio.

Study flowchart. We used stratified random sampling, creating subgroups according to the gender, age and geographical region, directly proportional to the same subgroup of the general population. During the random sampling process, the respondents were asked to state their age, gender, and region. As far as the survey was proceeding, and quotas were successively completed, we kept looking for respondents with demographic characteristics matching only the still incomplete quotas.
We stratified the participants into four social classes according to their education and occupation (class A/B, higher education and white-collar occupation; class D/E, lower or no education and unskilled or low skilled work) following the recommendations of the Hellenic Statistical Authority (ELSTAT) (14).
The geographic division of Greece in to four major regions followed the nomenclature rules of territorial units for statistics (15).
The people with headache fulfilling the diagnostic criteria of MOH, except for the one concerning the number of headache days per month, that is ≥15 headache d/m, were classified by us as the group of AHMO. The final sample of the general population that was interviewed consisted of 10,008 persons, aged 18–70, and 1197 of them suffered from headaches. The study was conducted by Ipsos Opinion S.A. on behalf of the Hellenic Headache Society, between 22 May 2017 and 27 June 2017.
Standard protocol approvals
The study protocol and the standardized questionnaire were approved by the Hellenic Data Protection Authority (No 1363/2017), in accordance with the General Data Protection Regulation (GDPR) (EU) 2016 (Online Supplemental Material 2) An additional approval from an ethics committee was not considered necessary. All interviewees gave a verbal informed consent.
Statistical analysis
The continuous study parameters (e.g., monthly workdays lost) were presented using mean ± standard deviation, while the nominal ones (e.g., prevalence) were presented using tables of frequencies. Normal approximation, 95%, two-sided confidence intervals (CIs) were used, while for all statistical tests the value for α was equal to 0.05. Binary logistic regression (BLR) with stepwise selection model was used to test the relationship of MOH among the primary headache types, and among the recipients and non-recipients of prophylactic treatment. Demographic data were also used as independent variables in the logistic regression model. Consequently, we tested the relationship of monthly workdays lost with the demographic data of people with headache and primary headache types using Multiple Linear Regression (MLR). The same model was used for the analysis of monthly days with reduced performance by diagnosis of headache type, gender, age, social class and geographical region, as well as for the comparison of monthly frequency of pain relief intake by geographical region and use of prophylactic treatment. For all regression models, the reference category of each independent variable was its 1st category. Missing data were infrequent and random and therefore we applied pairwise deletion for basic statistics and listwise deletion for BLR or MLR. Most of the comparisons applied resulted in p-values either greater than 0.5 or less than or equal to 0.02. Thus, we did not proceed further to make corrections for multiple comparisons. Finally, we tested for multicollinearity, whenever necessary, using the variance inflation factor (VIF) with values >5 as a cut-off point for variable removal from the model. For nominal variables we constructed dummy variables and applied again the VIF rule. IBM SPSS Statistics for Windows v24.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses.
Results
Estimation of MOH in the general population
The prevalence of MOH in the sample of the general population was 0.7% (69/10,008), with 95% confidence interval (CI): 0.5%–0.9%. The female to male ratio was 3.6 (1.1% for females and 0.3% for males, P < 0.01). The prevalence of MOH in the general population, and its proportion by gender, age and geographical region is presented in Table 1. Notably, the proportions of all three factors were found to be strongly statistically significant in the model of BLR used (Table 2). There was higher proportion of MOH in the 35–54 age group (p < 0.02) and in the region of Aegean Islands and Crete (p < 0.01) (Figure 2). The mean monthly workdays lost, due to headaches, in the sample of participants with MOH, was 1.0 d/m (95% CI: 0.4–1.6) and the mean monthly days with reduced performance was 6.3 d/m (95% CI: 3.9–8.7), corresponding to the rates of absenteeism and presenteeism. Table 3 presents these rates by gender, age, region and social class.

Proportion (%) of MOH by region (N = 1197).
Mean monthly workdays lost and mean monthly days with reduced performance, by gender, age, region and social class in the MOH group.

NUTS: Nomenclature of territorial units for statistics.
Class A/B: higher education and white-collar occupation. Class D/E: lower or no education and unskilled or low skilled work.
MOH: Medication Overuse Headache.
Estimation of the proportion of MOH in subgroups of people with headache
The proportion of MOH among the people with headaches was 5.8% (69/1.197, 95% CI: 4.4%–7.1%). The proportion of females with MOH within the same group was 6.3% (54/856, 95% CI: 4.7%–7.9%)
The distribution of MOH within the headache group, according to the diagnosis of headache type is shown in Tables 4 and 5. The percentage of MOH was 50.5% (95% CI: 40.8%–60.1%) and 45.9% (95% CI: 29.9%–62.0%) in participants with chronic migraine (CM) and chronic TTH (cTTH), respectively (Table 4). MOH was nearly 3.3 times more frequent in the group of people with headache taking prophylactic treatment than those in the non-prophylactic treatment group (19.0%, 95% CI: 9.5%–29.1% versus 5.8%, CI: 4.4%–7.1%, respectively, p < 0.05). In addition, the proportion of participants living in Aegean islands and Crete was also higher than those living in the mainland (8.4%, 95% CI: 4.9%–13.1%, versus 4.9%, 95% CI: 2.8%–7.0%, in Attica, 5.4%, 95% CI: 3.1%–7.8%, in Northern Greece and 6.1%, 95% CI: 3.5%–8.8%, in Central Greece, p < 0.01) (Table 5).
Proportion of MOH by headache type and prophylactic treatment among people with headache (N = 1197).

MOH: Medication Overuse Headache.
Proportion of MOH by gender and region among people with headache (N = 1197).

*NUTS: Nomenclature of territorial units for statistics.
MOH: Medication Overuse Headache.
The distribution of absenteeism and presenteeism in the MOH group, across the demographic factors, namely gender, age group, geographical region and social class did not reveal any significant effect.
Prophylactic treatment was found to have a statistically significant relationship with the percentage of MOH among participants with headaches (p < 0.05), (Table 6). The mean monthly frequency of acute medications intake was 15.6 d/m (± 8.7) for the participants taking prophylactic treatment versus 8.7 d/m (±7.2) for those not taking prophylactic treatment. Simple analgesics (aspirin and paracetamol) or NSAIDS alone or in combined products was the most common drug class (94.1%), followed by opioids (7.9%) and triptans (3.4%) (Table 7).
Logistic Regression table. Dependent variable: MOH in the headache group (N = 1197).
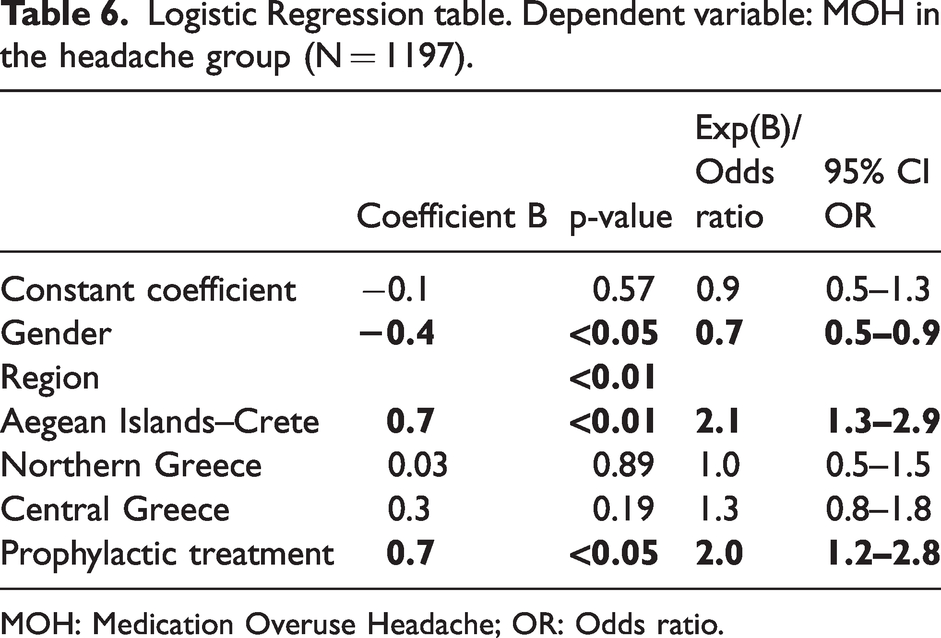
MOH: Medication Overuse Headache; OR: Odds ratio.
Drug classes in the MOH (N = 69) and AHMO groups (N = 203).
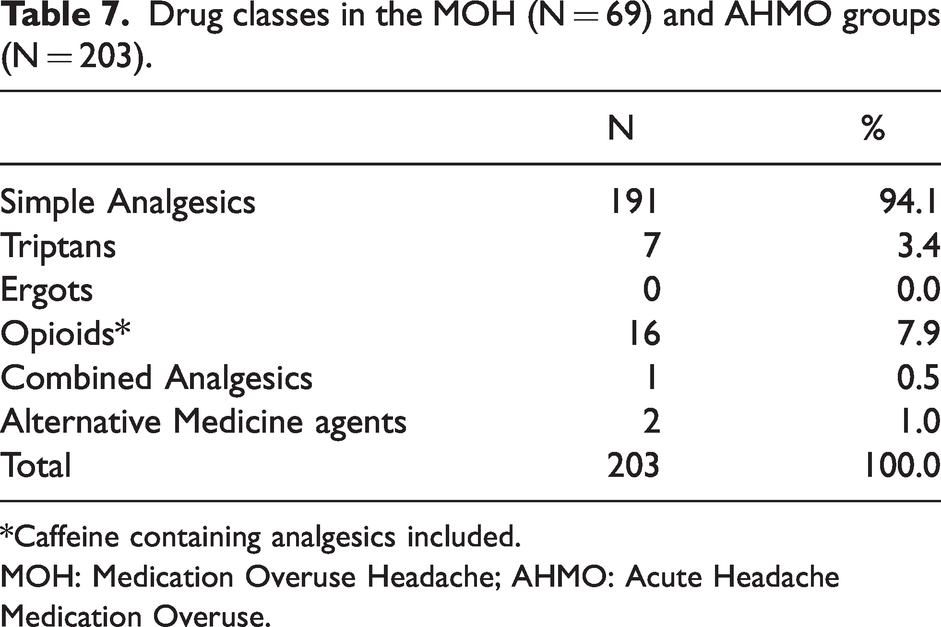
*Caffeine containing analgesics included.
MOH: Medication Overuse Headache; AHMO: Acute Headache Medication Overuse.
AHMO estimation in participants with headache
The number of people with AHMO was 203, corresponding to a prevalence of 2.0% (95% CI: 1.8%–2.3%) in our sample of the general population and a percentage of 17.0% (95% CI: 14.8%–19.1%) in the group of people with headache. The female to male ratio, in the AHMO group was 3.8:1 (161:42). The proportion of AHMO participants was higher in the age group 35–54 (36/69 persons, 52.2%), followed by the age group 55–70 (20/69, 29.0.0%), and the 18–34 group, (13/69, 18.8%). The region of Aegean Islands and Crete, similarly to MOH, showed the highest proportion of AHMO (3.1%, 95% CI: 2.0%–4.1%), in comparison to the rest of the regions. All three factors, namely gender, age group and region were found statistically significant in BLR model, but not the social classes (p < 0.01, p < 0.01 and p < 0.02 and p > 0.05, respectively). The distribution of proportions of AHMO among the episodic headache types showed a clear preponderance of high frequency episodic migraine (HFEM), 24.9% (95% CI: 18.8%–31.0%), followed by low frequency episodic migraine (LFEM), 10.8% (95% CI: 8.2%–13.5%) and episodic TTH (eTTH), 8.5% (95% CI: 5.5%–11.4%).
Discussion
Summarizing our data, the estimation of the prevalence of people with MOH was 0.7% (95% CI: 0.5%–0.9%) in Greece in 2017 and nearly four times more common in females (3.6:1). The proportion of MOH among the people with headache was estimated to be 5.8%. The maximum frequency was in the age group 35–54 followed by the ≥55 group. It was also more frequent in the geographical region of the Aegean islands and Crete versus the mainland. The group of people with AHMO is not a discrete diagnostic category or headache type within ICHD-3. Nevertheless, we separately calculated the same parameters as MOH, for this group since it consists one of the important risk factors for headache chronification (2,3,7,16). MOH was determined to be more frequent in CM (50.5%, 95% CI: 40.8%–60.1%) followed by cTTH 45.9% (95% CI: 29.9%–62.0%). The proportion of AHMO was estimated at 2.0% (95% CI: 1.8%–2.3%) in the general population, while its proportion in the group of people with headache was at 17.0% (95% CI: 14.8%–19.1%), following similar distribution among age groups, gender, and geographical regions, as MOH. AHMO was more frequent in HFEM (24.9%, 95% CI: 18.8%–31.0%), in comparison to other episodic headache types.
The global prevalence of MOH, under the current diagnostic criteria, varies broadly between 0.5% to 7.2%, with a median value of 1–2%, affecting nearly 60 million persons (2), and 11–70% in the group of people with chronic daily headache (3). Especially in Europe, the prevalence of MOH is estimated in the median range of 1–2% (16). Thus, the 0.7% prevalence of MOH in Greece is below the European mean of MOH and at the lower limit of the global median range. The female to male ratio has been reported between 3:1 (16) and 4:1 (2,17,18). Our finding of 3.6:1 female to male ratio of MOH and 3.8:1 of AHMO is also within the usually reported range. The age group with the highest proportion of MOH has been reported to be 50–60 years old (2,16), while the lowest one is in adolescents (19). Although the age group categorization is not always comparable among studies, our findings are in accordance with the previously reported data. Among the four main geographical regions of Greece, the Aegean islands and Crete had a proportion of MOH as high as 1.1%, more than double when compared to 0.5% in Attica (prefecture of Athens). This finding is not readily interpretable with the data collected in our survey. If for instance, there are differences among the geographical regions, concerning the risk factors for MOH, that potentially affects its proportion among them (2), such as psychiatric or gastrointestinal comorbidities, BMI, and habits like smoking, these data are not available from our survey in order to make any evidence-based assumption.
The analysis of the social classes showed a significant relationship only between the C2 class and MOH. The people in this class are mainly skilled manual workers, with a level of education more than elementary. It is widely accepted that a low socio-economic level is a risk factor contributing to MOH (20–22). Thus, our finding is rather close to this line of data. However, no significant effect of the social class factor was detected in the ΑΗMO group.
Within the group of 1197 people with headache, in our sample, the ICHD-3 criteria of MOH were fulfilled by 17.0% (95% CI: 14.8%–19.1%), except for the last criterion, that is headache for 15 d/m or more. This is the group we named as AHMO. A very similar number of AHMO, namely 17.7%, has been reported in the Chronic Migraine Epidemiology and Outcomes (CaMEO) Study (23) and 15.4% in the Migraine in America Symptoms and Treatment (MAST) study (24). Both of them calculated the migraineurs with AHMO, independently of their number of headache d/m (the last one criterion) and consequently did not fulfill one of the main diagnostic criteria of MOH, i.e. that the monthly headache days have to be ≥15 d/m. In addition, a whole 67.9% of the group included in the 17.7%, had <15 monthly headache days (23). Hence, those with MOH should be one third of 17.7%, corresponding to a percentage around 6% of the total number of migraineurs, without including any other headache types. Thus, these numbers, although apparently similar, are not directly comparable to ours, due to the absence of any other headache type in their study except for migraine. The distribution of MOH across its coexisting chronic headache types, shows a slight preponderance in CM (50.5%), followed by cTTH (45.9%) (Table 8, Figure 3) In a German study (25), following the ICHD-2 criteria, it was estimated that 66.7% of chronic migraineurs fulfilled the MOH criteria as well. In general, a high prevalence of MOH in chronic headache types is widely accepted (2,26,27). HFEM is the episodic headache type with the highest proportion of AHMO, followed by LFEM and eTTH with proportions of 24.9%, 10.8% and 8.5% respectively. Similarly, high proportions of AHMO have also been shown by CaMEO and MAST studies, in the group of migraineurs with <15 migraine d/m, as mentioned earlier. The presence of AHMO in episodic types of headaches is of notable clinical importance, since it is one of the significant risk factors for their chronification (4,7,28–31). There is also a notable 22.9% difference in the prevalence of AHMO between prophylactic treatment users and non-users (38.7% versus 15.8%). Similarly, those under prophylactic treatment, were using pain relief medications for 15.6 d/m versus 8.7 d/m to non-users. This finding may suggest a common patient perspective to receiving either acute headache medication or prophylactic treatment. Those with a positive point of view for pharmacological treatments accept both acute headache medication and prophylaxis more easily, while those with a negative point of view do not accept either of them. The administration of an additional nocebo questionnaire would be probably helpful for the clarification of this point. The common analgesics were by far the most dominant class of drugs, both in the MOH and AHMO groups, with an impressive percentage of 94.1%, followed by 7.9% for opioids and 3.4% for triptans. Ergots have not been available in the Greek pharmaceutical market during the last decade and for this reason they were not included. Medications including caffeine were available only in combination with opioids during and prior to our survey. The combined analgesics are not a common option in our sample, in contrast to other countries (24).
Percentage of AHMO by headache type and prophylactic treatment among people with headache (N = 1197).


Percentage (%) of AHMO by headache type, in the headache group (N = 1197).
In our previous epidemiological study (13), a significant percentage of 43.5% (95% CI: 40.6%–46.3%) of the people with headache experienced shame or other negative feelings in their work or home due to their headaches. Thus, nearly half of the people with headache in Greece, frequently, avoid stating that they are suffering from headache, experiencing it in private.
Strengths and limitations of the study
This is the first large population-based epidemiological survey investigating the prevalence of MOH both in the general population and across demographic parameters. Additionally, the burden of MOH in Greece, in terms of absenteeism and presenteeism was also investigated. The first limitation concerns the cross-sectional surveys in general. The collection of information demands that the participants recollect their symptoms and habits for a period of months and sometimes years. Thus, some degree of distortion of the recollected information is inevitable, decreasing the reliability of the data. The questionnaire was standardized by headache experts in their clinic or in their outpatient offices and not in the general population, where the survey was conducted. The diagnosis of MOH has not been included in the standardization procedure of the questionnaire and thus the data about sensitivity and specificity were not available. In addition, the burden of MOH, in terms of absenteeism and presenteeism, was assessed by self-reporting data, and not by any relevant questionnaire, such as MIDAS. From the initial number of 97,803 phone calls a percentage as high as 70.2% did not participate in the survey finally. This dropout may have affected the representativeness of the sample, despite the balance achieved by age, gender and geographical region. Furthermore, based on the automatic diagnostic algorithm only one diagnosis could be made. Thus, the cases with more than one coexistent headache disorder were categorized into the most predominant one.
Conclusions
Nearly one out of 140 Greek citizens (0.7%), aged 18–70 years old, fulfil the ICHD-3 criteria for MOH. This prevalence of MOH is lower than the median range of European prevalence, i.e., 1–2%. The presence of MOH is nearly four-fold in females in comparison to males and more frequent in the age groups 35–54 and ≥55 years old. The proportion of MOH among people with headaches is 5.8% (95% CI: 4.4%–7.1%). The burden of MOH, in terms of monthly workdays lost and monthly workdays with decreased productivity, is considerable, contributing to the huge total indirect and direct burden of MOH, raising it into a worldwide health problem which demands special attention from physicians and health authorities.
Public health relevance
The prevalence of MOH in the general population of Greece, aged 18–70, is 0.7% (95% CI: 0.5–0.9), affecting the females 3.6 times more frequently than males. The proportion of MOH, in the group of people with primary headaches affecting performance, is as high as 5.8% (95% CI: 95% CI: 4.4%–7.1%). The mean absenteeism in people with MOH was 1.0 d/m (95% CI: 0.4–1.6) and the mean presenteeism 6.3 d/m (95% CI: 3.9–8.7). The group of people with AHMO, i.e., the people with less than 15 or more headache d/m, but fulfilling the rest of diagnostic criteria for MOH, represent 2.0% (95% CI: 1.8%–2.3%) of the Greek general population and 17.0% (95% CI: 14.8%–19.1%) of those with headaches. The MOH criteria are fulfilled by 50.5% (95% CI: 40.8%–60.1%) of chronic migraineurs and 45.9% (95% CI: 29.9%–62.0%) of people with cTTH. Furthermore, the AHMO group, represented a percentage as high as 24.9% (95% CI: 18.8%–31.0%) of people with HFEM. The presence of AHMO as well as the rest of the episodic headache types, namely LFEM and eTTH, must be managed properly by the treating physicians, in order to decrease the risk of their future chronification.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024231184909 - Supplemental material for The prevalence and burden of medication overuse headache in Greece
Supplemental material, sj-pdf-1-cep-10.1177_03331024231184909 for The prevalence and burden of medication overuse headache in Greece by Theodoros S. Constantinidis, Chryssa Arvaniti, Nikolaos Fakas, Jobst Rudolf, Evangelos Kouremenos, Ermioni Giannouli, Dimos D. Mitsikostas and on behalf of the Hellenic Headache Society in Cephalalgia
Supplemental Material
sj-pdf-2-cep-10.1177_03331024231184909 - Supplemental material for The prevalence and burden of medication overuse headache in Greece
Supplemental material, sj-pdf-2-cep-10.1177_03331024231184909 for The prevalence and burden of medication overuse headache in Greece by Theodoros S. Constantinidis, Chryssa Arvaniti, Nikolaos Fakas, Jobst Rudolf, Evangelos Kouremenos, Ermioni Giannouli, Dimos D. Mitsikostas and on behalf of the Hellenic Headache Society in Cephalalgia
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TSC, CA, NF, JR, EK and EG report no disclosures. DDM received research support, speaking fees and travel grants from Allergan and Novartis, relevant to the present study.
Funding
The authors disclosed receipt of the following financial support or the research, authorship, and/or publication of this article: This study was designed by the Hellenic Headache Society and was conducted on its behalf by Ipsos Opinion S.A. Company. The study was supported by unrestricted research grants from Novartis Hellas and Allergan Hellas.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.