
Abstract
Aim
J.A.P. and M.A.L. contributed equally to this manuscript.
Methods
A retrospective, controlled follow-up study was performed with 416 MOH patients. All patients were treated with outpatient withdrawal therapy, with two treatment arms: with or without the support of a specialised headache nurse. The outcome measures were: i) successful withdrawal, defined as discontinuation of all headache medication according to the study protocol; and ii) the responder rate, defined as the percentage of patients with ≥50% reduction in headache days after successful withdrawal and iii) relative reduction in headache days after successful withdrawal.
Results
Successful withdrawal percentages were significantly higher in the group supported by the headache nurse than in the group without support (73.1% vs. 60.7%; p = 0.008), which was confirmed in multivariate analysis (OR 1.73, 95% CI 1.11–2.71, p = 0.016). Support by a headache nurse was not associated with response. The underlying primary headache diagnosis, determined after withdrawal, was significantly correlated with response.
Conclusion
The support by a headache nurse results in an increased adherence to detoxification.
Introduction
Medication-overuse headache (MOH) is a highly disabling headache disorder, with a population-based prevalence of 0.7%–1.7% and a preponderance in women (1–3). The prevalence in headache clinics ranges from 30% in Europe to more than 50% in the United States (1,2). MOH is defined in the International Classification of Headache Disorders, third edition beta (ICHD-III beta) criteria as headache occurring on half or more days per month as a consequence of regular overuse of acute headache medication (on ≥10 or ≥15 days per month, depending on the type of medication) for more than three months (4). Although consensus about the optimal treatment for MOH has not yet been reached, withdrawal of the overused medication is strongly suggested as an essential component in the management of MOH, to reduce headache frequency and improve responsiveness to both acute and prophylactic therapy (1,2,5,6). Several studies have compared different treatment strategies (2,7) and some suggested that simple withdrawal advice is effective (8,9). In compliance with those studies, acute withdrawal without any concomitant therapy is advised in the national headache guidelines of the Netherlands, and common practice. However, a well-defined selection of patients prone to benefit from simple withdrawal advice has not been established. Withdrawal programmes are increasingly multidisciplinary coordinated, with implementation of patient education and motivational or cognitive behavioural therapy, often realised by a headache nurse (10–14). Despite this, the effectiveness of a headache nurse in withdrawal therapy has never been studied in a controlled follow-up study. Therefore, the objectives of this study are (i) to determine whether support by a headache nurse in the treatment of MOH increases successful withdrawal, and (ii) to investigate intrinsic patient factors associated with response to withdrawal therapy.
Methods
Study design and population
The current study used a retrospective, controlled follow-up approach. Participants were recruited during a period of four years (1 April 2006–31 March 2010) among all new patients at the specialised outpatient headache clinic of the Leiden University Medical Centre (LUMC), functioning both as a primary and secondary referral centre with referrals from general practitioners and from colleague neurologists. Inclusion criteria for participants were: (i) age ≥18 years; (ii) diagnosis of MOH, defined by the ICHD-II criteria (15), which are similar to the ICHD-III beta criteria on MOH (4) (supervised by an experienced headache neurologist (MDF, GMT)); and (iii) receiving advice to withdraw all acute headache medication (triptans, analgesics, combination of both, other medication comprising opioids, ergots or combinations of those medications with analgesics or triptans), prophylactic medication and caffeine-containing liquids during two or three months. Follow-up occurred after withdrawal, to determine the final underlying primary headache diagnosis and start further treatment. At the first visit patients were instructed that because of lack of therapeutic options whilst overusing medication, no follow-up visit was offered if they did not succeed to withdraw. Therefore, patients who were lost to follow-up were considered as ‘not successfully withdrawn’. Patients were excluded when the final diagnosis was not migraine, tension-type headache or a combination of both. The treatment protocol for patients included between 1 April 2006 and 31 March 2008 (group A) comprised withdrawal advice by a resident in neurology/neurologist. All physicians involved during the total inclusion period gave the same instructions and maintained the same conditions of withdrawal, according to the standardised protocol at the LUMC. This encompassed an outpatient detoxification with the advice to instantly stop acute headache medication. The duration of the withdrawal period was two months in case of triptan overuse, three months for other types of medication or combinations of medication, and/or caffeine use of ≥5 units/day. If patients were on preventive treatment this was tapered off, since the present medication was not effective, and preventive medication regains effectiveness after withdrawal (6). New preventive treatment was postponed until successful withdrawal was accomplished. Use of escape medication or caffeine-containing liquids was not permitted. During the withdrawal period no facility was provided for additional contacts or support. Due to the employment of a specialised headache nurse ever since 1 April 2008, patients included between 1 April 2008 and 31 March 2010 (group B) were advised exactly the same withdrawal protocol, but additionally received support during the withdrawal period by the specialised headache nurse. The headache nurse was trained and experienced in headache care, and received additional training on cognitive behavioural therapy. The support by the headache nurse started immediately during the first visit with a 15- to 30-minute consultation consisting of a reprise of the withdrawal advice and elaboration on questions from the patient. The consequences for daily professional and social life were discussed and a plan of approach was assembled. Furthermore, strategies for pain management (other than medication treatment) were discussed. Subsequently, the headache nurse contacted all patients two weeks after initiation of the withdrawal period. Depending on the patients’ need for support, the headache nurse had additional interaction during the withdrawal period, varying from one to six contacts (median three contacts) by telephone.
Measurement
Two trained examiners obtained medical information from the outpatient clinic administration, patient letters and medical files, using the same methods and criteria to select patients and classify data. The outcome measures were: i) successful withdrawal, defined as a completed medication- and caffeine-free period; ii) response, defined as ≥50% reduction in headache days after successful withdrawal; and iii) relative reduction in headache days after successful withdrawal, since a reduction <50% may be considered clinically relevant as well (16). The number of headache days at baseline and at follow-up were collected to calculate outcome measures. In case of missing data on response (n = 25 patients), patients reporting ‘strong improvement’, ‘nearly no headache’ or ‘no headache’ at follow-up were considered as a ≥50% reduction in headache days (responder), and patients reporting ‘aggravation’, ‘no improvement’ or ‘some to moderate improvement’ at follow-up were considered as a <50% reduction in headache days (non-responder). This subjective classification and the classification based on absolute change in headache days were highly correlated (n = 75, r = 0.80, p < 0.001). To be able to find associations between potential intrinsic determinants and our outcome measures, we collected data on gender, age, pre-existing headache type, final primary headache after successful withdrawal, number of headache days at baseline, number of medication days at baseline, type of overused medication, and caffeine units per day. Pre-existing headache and final primary headache at follow-up were classified according to ICHD-II/ICHD-III beta criteria (4,15) as: i) migraine; ii) tension-type headache; and iii) combination of both migraine and tension-type headache. Because of the typical blurred presentation of primary headache at baseline, which is often the case during a period of medication overuse, the pre-existing headache was in some cases impossible to determine (n = 85). Therefore, final primary headache diagnosis was used in the analysis. In any case, pre-existing and final headache diagnoses were fairly correlated (n = 182, r = 0.62, p < 0.001). Type of acute medication was classified as: i) triptans, ii) analgesics (paracetamol/acetaminophen and/or nonsteroidal anti-inflammatory drugs (NSAIDs)), iii) combination of triptans and analgesics, and iv) other medication, comprising opioids, ergots or combinations of those medications with analgesics or triptans. No approval of the local ethics committee was necessary as the study was a retrospective follow-up study and all data were analysed anonymously.
Data analysis and statistics
Baseline characteristics were reported as mean ± SD or absolute numbers with percentages. The number of headache days and medication days at baseline were grouped into daily (30.4 days/month) and non-daily ( < 30.4 days/month), because of the non-parametric distribution of the data. Differences in means between groups were tested with independent sample t-tests and one-way analyses of variance (ANOVAs). Differences in proportions were tested using χ2 tests. Patients were stratified into ‘successfully withdrawn’ and ‘not successfully withdrawn’, the latter including patients who were lost to follow-up. All patients were included in the analysis of the first outcome (successful withdrawal). Successfully withdrawn patients were included in the analysis of the second and third outcomes (response and relative reduction). Univariate logistic regression models were used to test crude associations. Analyses were rerun as a multivariate model, adjusting for the potential confounding effects of all variables that were tested in the univariate model. For all analyses, two-tailed p values < 0.05 were considered as statistically significant. All statistical analyses were performed using SPSS 17.0 (SPSS Inc, IBM, USA).
Results
Participants and descriptives
The total study flow is shown in Figure 1. Of 2086 new outpatients, 416 patients were diagnosed with MOH and advised to withdraw medication, 163 without (group A) and 253 with support of a headache nurse (group B). Both groups differed significantly in gender, age, type of medication and daily use of medication (Table 1). Although the absolute number of new headache patients visiting the outpatient headache clinic increased in the last two years of the inclusion period, the proportion of patients who met inclusion criteria remained the same (19.0% in group A and 20.6% in group B). To detect shifts in population composition due to exclusion of patients, loss to follow-up or missing data, differences between the total included population (n = 416) and the population that had successfully withdrawn (n = 267) were explored. No major differences in composition occurred.
Study population flowchart. Baseline characteristics of patients with medication-overuse headache, included for primary analysis, without (group A) and with (group B) support by a headache nurse (n = 416). Values are the absolute numbers with corresponding % or means ± SD. Significant p values are depicted in bold. aχ2 test. bTwo-tailed independent samples t-test. cIndependent samples Mann-Whitney U test.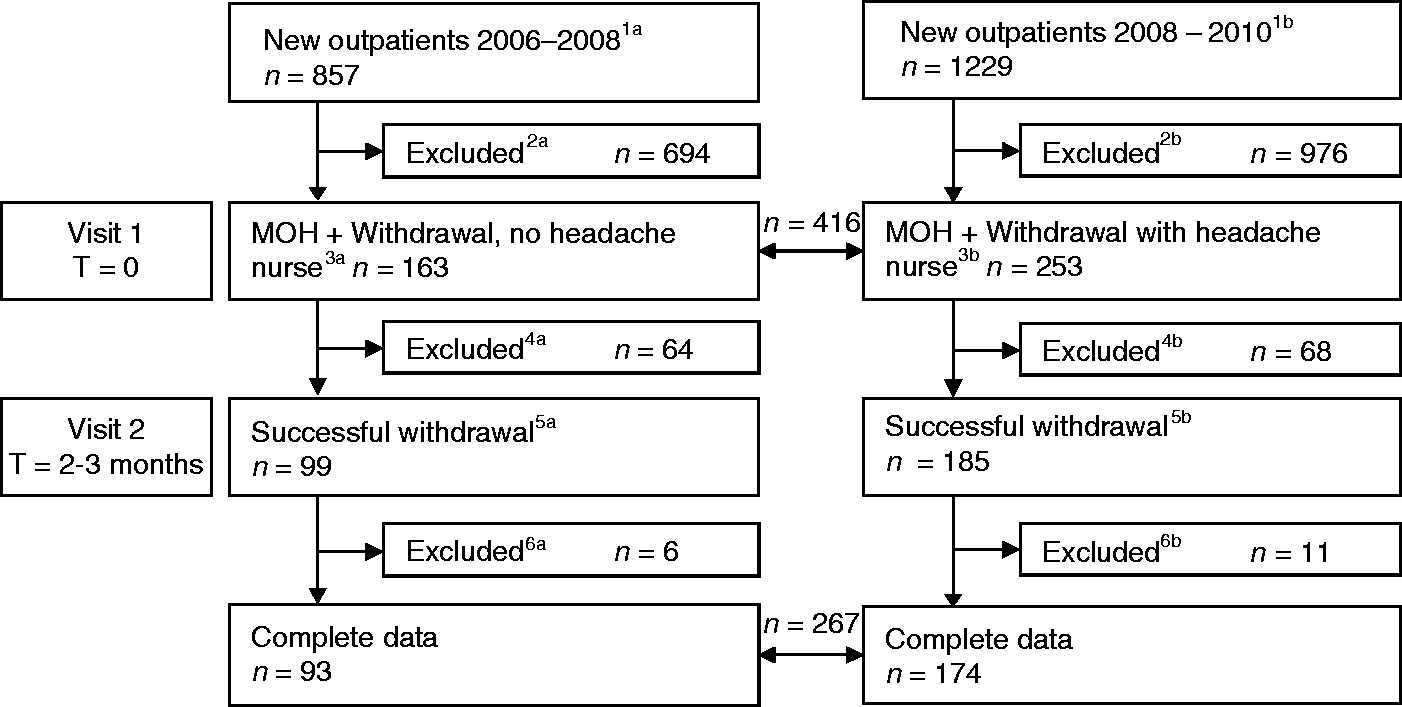

Effectiveness of support by a headache nurse in successful withdrawal in MOH
Successful medication withdrawal, defined as a two- to three-month medication- and caffeine-free period, in patients with medication-overuse headache following withdrawal therapy without (group A) and with (group B) support by a headache nurse (n = 416).

Values are the absolute numbers with corresponding %.
Including patients who are lost to follow-up and therefore considered not successfully withdrawn 44 (27.0%) and 31 (12.3%), respectively. bχ2 test.
Odds ratios (1. univariate; 2. multivariate, adjusted for all mentioned covariates) for successful withdrawal, defined as a two- to three-month medication- and caffeine-free period (n = 416).
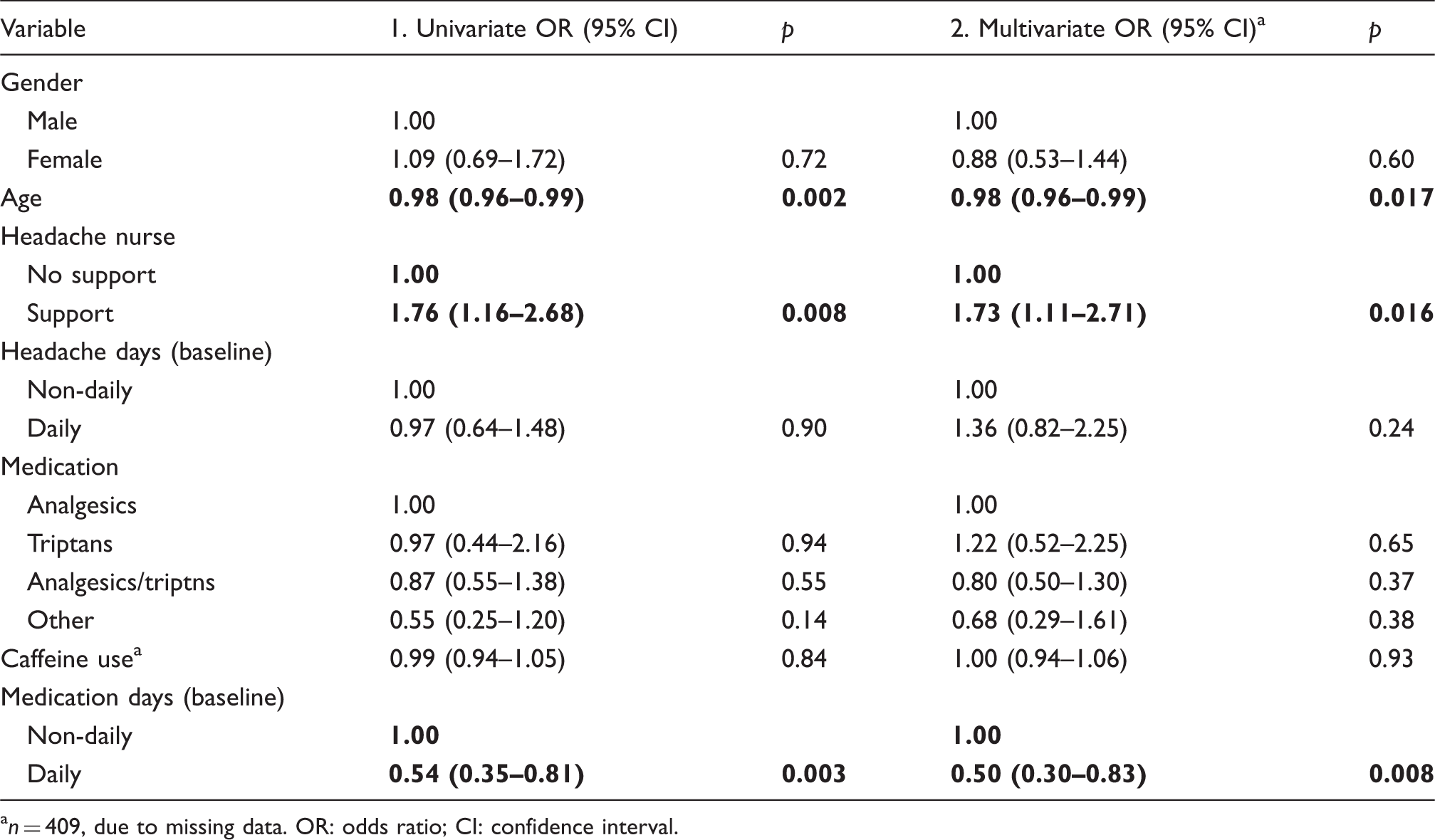
n = 409, due to missing data. OR: odds ratio; CI: confidence interval.
Variables associated with response and relative reduction to withdrawal therapy
The support by a headache nurse was not associated with response (OR: 1.42; 95% CI 0.78–2.60; p = 0.25) (Table 4). The responder rate, defined as the percentage of patients with ≥50% reduction in headache days, was not significantly different in both groups (no support 35.5%, with support 46.0%, p = 0.098, Figure 2). The relative reduction in headache frequency, also showed no significant association with support by the headache nurse (B: 1.92; 95% CI –7.75 to 11.60; p = 0.70). This indicates that there is no effect of the support by the headache nurse on reduction of headache days when successfully withdrawn. The underlying primary headache disorder, which remained after the withdrawal, was significantly associated with relative reduction and response, with three times increased odds for response in case of migraine when compared to tension-type headache (OR 0.31, 95% CI 0.16–0.63; p < 0.001), and nine times increased odds in case of migraine when compared to migraine with tension-type headache (OR 0.11; 95% CI 0.05–0.24; p < 0.001) (Table 4). This gives a clear indication that the reduction in headache frequency was highest in the migraine group and lowest in the migraine with tension-type headache group (Table 4, also depicted in Figure 2). The relative reduction in headache days was 34.2% ± 38.9 for the total group and was significantly different between individuals with migraine, tension-type headache, and combined migraine and tension-type headache (56.1% ± 32.1, 26.0% ± 39.6 and 16.0% ± 31.9, respectively) (Figure 3). As shown in Table 4, gender and age were not associated with response, nor was the number of headache days or number of medication days at baseline. Furthermore, neither the type of medication that was overused (simple analgesics, triptans, combination of both, or other medication) nor caffeine use was associated with response. These covariates were not associated with relative reduction either.
The responder rate, defined as the percentage of patients with a ≥50% reduction in headache days, following medication withdrawal with and without support by a headache nurse, subdivided by diagnosis (N = 267). The mean relative reduction in headache days of successfully withdrawn patients and subdivided by diagnosis (n = 242, due to missing data in 25 patients, one-way ANOVA: p < 0.001). Error bars display standard deviations. TTH: tension-type headache; ANOVA: analysis of variance. Odds ratios (1. univariate; 2. multivariate, adjusted for all mentioned covariates) for response, defined as a ≥50% reduction in headache days, following medication withdrawal (n = 267). TTH: tension-type headache; OR: odds ratio; CI: confidence interval.


Discussion
Being the first controlled follow-up study, this study shows that support by a headache nurse during simple withdrawal therapy increases the chance that a patient with MOH successfully withdraws from overused medication. In this manner, the high drop-out percentage seen in outpatient withdrawal therapy can be reduced (7). As expected, the reduction in headache days during withdrawal therapy is independent of the support by a headache nurse, as this is more likely to be influenced by intrinsic, patient-related factors. The current study shows that patients with migraine as the solely underlying headache disorder have a higher chance at response to withdrawal therapy.
The strengths of this study include the controlled design in a large, representative study population of MOH patients. Although randomisation was not achievable, the retrospective design is particularly suited to determine the effect of the headache nurse, since we studied the insulated effect of the nurse and there were no ethical issues or risk of blinding failure. We changed our treatment protocol of patients with MOH during our inclusion period by the employment of a headache nurse in April 2008, but no other changes regarding to treatment protocol or referral strategies were introduced. In a prospective, controlled study, the recruitment procedure would lead to a highly motivated population, and it would be extremely difficult to blind patients for receiving or not receiving support by a nurse, since patients must be informed about the nature of a study. One group of patients would thus be instructed not to contact the outpatient clinic at any moment, whilst they know about the availability of support to the other group. This would definitely introduce disappointment and other expectations and would bias the results in favour of the intervention. The results of our retrospective study are not influenced by this kind of bias.
There are also some limitations of our study design. First and most important, there was no ability to collect data from patients who did not return for a second visit and were, therefore, stated as lost to follow-up. Since patients were explicitly instructed that they were not allowed to revisit in case of unsuccessful withdrawal, and they were informed that no additional treatment would be supplied, we consider the majority of the lost-to-follow-up patients as unsuccessfully withdrawn. We believe the possibility that loss to follow-up is caused by economic reasons negligible due to the health care system in our country, and the visit could be changed to a 15-to 30-minute telephone appointment in case patients definitely could not miss work. Analysis considering lost to follow-up as unsuccessfully withdrawn shows similar result as analysis with lost-to-follow-up patients as a separate group. Secondly, because of uncertainty about diagnoses before withdrawal, we diagnosed the primary headache disorder after successful withdrawal, and used this diagnosis. Still, the pre-existing primary headache diagnosis was fairly correlated with the final diagnosis. Third, long-term effects of withdrawal were not investigated in this study. Considering the high recidivism rate, it would be interesting in future research to study the long-term effect of support by a headache nurse in patients with MOH after withdrawal. However, the long-term effect of a headache nurse on medication overuse was beyond the scope of this study as we specifically wanted to investigate the response to the initial withdrawal period. In many countries patients with MOH are usually unwilling to endure acute withdrawal therapy. Patients in these countries refuse to discontinue their medication on the grounds that the withdrawal symptoms will be too serious or they are afraid to lose their jobs if they will be ill for a longer period because of the withdrawal symptoms. There is usually a drug treatment started with prophylactics although it is recognised that it often fails if the patient continues to overuse acute headache medication. Therefore, it was our main interest to show the high success rate of acute withdrawal with the support of a headache nurse.
In the literature, several withdrawal therapies, sometimes with support by a headache nurse, for MOH patients have been described, but no other study investigated the insulated effect of a headache nurse and uniform endpoints are lacking, hampering direct comparison between studies (11–14,16).
Possible explanations and implications
The headache nurse has an unmistakable effect on successful withdrawal therapy. Previous studies suggest that patients with (chronic) headache or high headache-related disability are more prone to use unsuitable coping mechanisms (17), score low on pain acceptance (18) and high on catastrophising scales, and experience low internal pain control (19). In patients with migraine, pain control and self-management can be improved by behavioural therapy (20). We hypothesise that contact with a headache nurse influences the above-mentioned factors and thus will help patients to endure the withdrawal period. Patients with tension-type headache and the combination of migraine and tension-type headache seem to benefit less from withdrawal therapy than patients with migraine alone, which may suggest that the pathophysiological mechanism of medication overuse differs between different underlying primary headache syndromes.
Nowadays the view on treatment of MOH shifts from the traditional ‘withdrawal therapy first’ towards an approach in which prophylactic therapies are started before patients are withdrawn from the overused medication. Randomised trials in chronic migraineurs with topiramate and onabotulinum toxin A (21–23) contributed significantly to the debate whether, and when, detoxification is necessary in the treatment of MOH (24). From these trials the question remains, however, whether the effect is clinically relevant. Moreover, the studies lack adequate reporting of plausible blinding failure, and most important, in these trials withdrawal was not advocated. To illustrate, the responder rate of migraineurs in our study is comparable to the responder rate in the pooled results of the onabotulinum toxin A trials. We realise that in our population not many patients overuse barbiturates or opiates, which enables acute medication withdrawal, in accordance with our national guidelines. Nevertheless, our study shows that with the support of a headache nurse, comprising only one face-to-face contact and a median of three contacts by telephone, 75% of MOH patients succeed to undergo a highly cost-effective outpatient withdrawal therapy, which is easily implemented in general neurology practice.
Withdrawal therapy is an effective treatment for MOH, especially for patients with migraine. Support by a headache nurse provides a substantial increase in treatment adherence and can be applied in an outpatient setting.
Clinical implications
With support by a headache nurse, almost 75% of medication-overuse headache (MOH) patients succeed to withdraw from overused medication. Withdrawal therapy with support by a headache nurse is applicable in an outpatient setting in general neurology practice. MOH patients with migraine as the solely underlying primary headache disorder benefit the most by simple withdrawal therapy.
Footnotes
Acknowledgements
The authors thank Mrs. J. Trouerbach, headache nurse, for supporting MOH patients during withdrawal therapy.
Funding
This work was supported by grants from the Netherlands Organization for Scientific Research (NWO) (VIDI 917.11.319 to G.M.T.) and the European Community (EC) (FP7-EUROHEADPAIN-no.602633). They had no role in the design or conduct of the study.
Conflicts of interest
M.A. Louter reports financial support for conference visits from Allergan and Menarini.
M.D. Ferrari reports grants and consultancy or industry support from Medtronic, Menarini, and Merck and independent support from NWO, the National Institutes of Health (NIH), the European Community, and the Dutch Heart Foundation.
G.M. Terwindt reports support for conference visits from Menarini, and independent support from NWO, the European Community, and the Dutch Heart Foundation.
The other authors have nothing to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.