
Abstract
Introduction:
Headache epidemiological studies in Latin America are scarce, and available data suggest that medication overuse headache is an existing health concern in the region.
Materials and Methods:
A survey empirically constructed to assess the management of medication overuse headache was sent to all the International Headache Society (IHS) members from Latin American countries.
Results:
We found no IHS members in 13 countries of Latin America. In countries with active members, the median number of IHS members per million inhabitants was significantly less when compared to Western Europe. Although the International Classification of Headache Disorders-3-beta (ICHD-3-beta) criterion was the most frequently used tool for medication overuse headache diagnosis, 41% of responders considered the diagnostic criterion ‘ambiguous’ and only 67% found them ‘very useful’. With respect to preferred treatment patterns, an important lack of uniformity, and a very limited usage of therapeutic approaches widely employed in other regions, characterized the responses.
Conclusion:
There is an urgent need to reach a consensus and establish region-specific strategies for the management of medication overuse headache as well as other headache disorders in this region. Development of headache specialized educational programmes, and participation of Latin American health providers in the IHS, should be incentivized.
Keywords
Introduction
Medication overuse headache occurs as a consequence of inappropriate management of primary headache disorders in susceptible individuals. 1 It is a highly burdensome condition at both personal and societal levels. 2 Its treatment is often challenging, requiring strong patients’ commitment in hands of well-trained, dedicated, health providers. Even in the best-case scenario, relapses are common and difficult to prevent. 2
Latin America extends from the northern Mexican border to the southernmost point of Chile. Its estimated population in 2015 increased to 626,741,000 people, representing approximately 8% of the total global population. 3 Epidemiological studies in this region are scarce, and available data suggest that headache disorders represent a common public health problem, with a mean migraine prevalence estimated around 9.6%. 4
The prevalence of medication overuse headache in this region is completely unknown. A nationwide population-based study in Brazil performed almost a decade ago revealed an alarming prevalence of chronic daily headache that reached approximately 7%. 5 More recent studies in Argentina and Chile have recognized medication overuse headache as an existing health concern but provided no specific numbers of the amount of individuals affected by this condition within the general population. 6
As an initial step towards unveiling the problem of headache disorders in the region, this study presents the results of a medication overuse headache survey among members of the International Headache Society (IHS) from Latin America and discusses the findings.
Materials and methods
Using the Qualtrics® survey platform, a survey was sent to all IHS members from Latin American countries. Members’ email addresses were available by logging into the IHS website 7 as a member. Five emails were immediately returned because of an incorrect email address; however, these individuals were finally reached after finding their updated contact details. A second email was sent to non-responders after 2 to 3 weeks. Accompanying the link to the survey, an explanatory letter about the objectives and importance of this research was sent to all Latin American members in an attempt to increase willingness to participate. The questionnaire was empirically constructed to assess the management of medication overuse headache by practitioners from this region. It consisted of nine items addressing medication overuse headache diagnosis (1–3), and specifically the usefulness of the International Classification of Headache Disorders 3rd edition beta version (ICHD-3-beta) criterion (4); medication overuse headache treatment patterns (5); personal information questions evaluating the clinical practice setting (6); years of experience treating headache patients (7); area of expertise (8); and participation in medical/scientific societies (9). The questions included multiple choice questions, rating scales and free text input. Questions were initially written in Portuguese (Brazilian version) and then translated into Spanish to cover all Latin American countries. An English version of the survey is available in the annexes. Responses were anonymous. Statistical analyses and figures were performed using Prism version 6.00 for Windows (GraphPad Software, La Jolla, California, USA) and SPSS (Version 20.0, IBM Corp, Armonk, New York, USA). Given that data were non-normally distributed, the median and interquartile range were employed for descriptive analyses and non-parametric tests were performed for hypothesis testing.
Results
There were 12 countries with and 13 countries without (Belize, Costa Rica, Ecuador, El Salvador, Guyana, Haiti, Honduras, Jamaica, Panama, Paraguay, Puerto Rico, Suriname, or Venezuela) registered IHS members. Although Belize, Guyana and Suriname do not speak a Latin language, we still included them in the study for geographical reasons.
The median number of IHS members per million inhabitants in Latin America (n = 12, median = 0.295; IQR = 0.1274–0.512 IHS members/million) was significantly inferior compared to a group of Western European countries (Belgium, Denmark, France, Germany, Ireland, Italy, Luxembourg, Netherlands, Portugal, Spain, Switzerland, United Kingdom) (n = 12, median = 0.887; IQR = 0.444–2.592 IHS members/million; Mann–Whitney test, p < 0.01; Figure 1).

International headache society members per million habitants in Latin America (colour coded). The highest density was found in Dominican Republic. There are no registered IHS members in 13 countries in the region. IHS: International Headache Society.
From the 164 surveys delivered, only 50 responses were received, resulting in country-wise response rates mostly below 50% (median response rate of 27.7%; IQR = 4.175–50.00%; Figure 2). Nearly all responders (96.2%) were clinicians working on private (79.3%) or public (39.6%) settings, with a median of 17 years (range 2–42 years) of experience of seeing headache patients. Besides being enrolled in the IHS, 38% of responders referred being members of the Latin American Headache Association (ASOLAC), 34% of responders referred being members of the European Headache Federation and another 21% participate in the American Headache Society.

Survey response rates per country.
The ICHD-3-beta criterion for medication overuse headache, headache diaries and treatment response were the most frequently used tools for diagnosis of patients frequently taking acute medication. Responses concerning the conciseness and ease of use of the ICHD-3-beta diagnostic criterion for medication overuse headache, as well as diagnostic implications, are summarized in Figures 3 and 4. Responses concerning treatment patterns and withdrawal preferences are summarized in Figure 5.

Clearness (left) and usefulness (right) of the ICHD-3 beta criteria for the diagnosis of medication overuse headache according to survey responses. ICHD: International Classification of Headache Disorders.
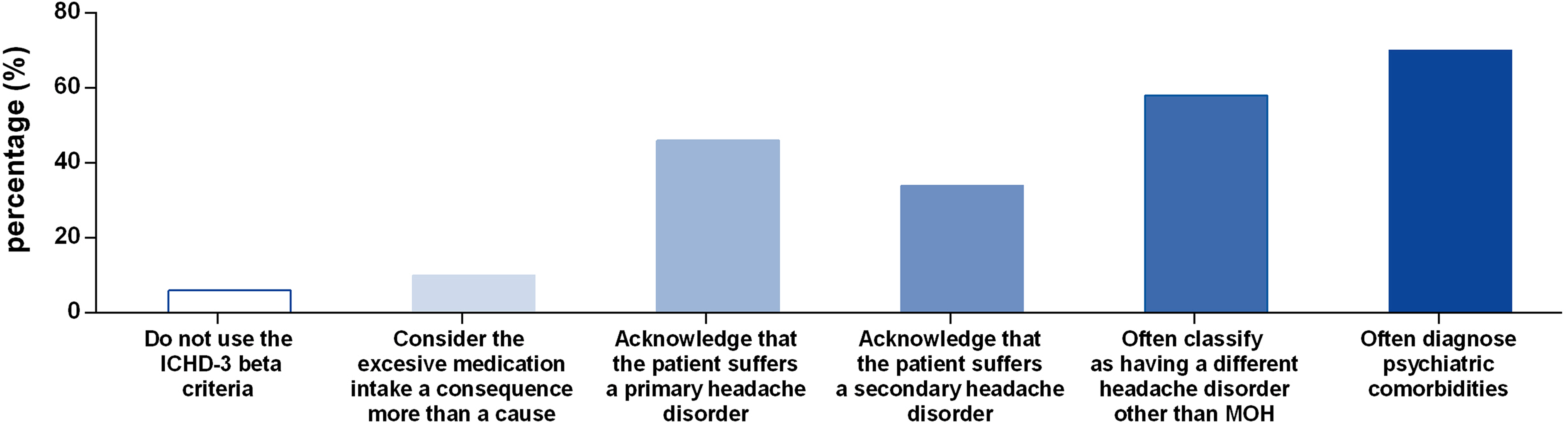
Related concepts when diagnosing medication overuse headache.

Top – usage of different therapeutic approaches. Bottom – withdrawal pattern preferences.
Discussion
Results from this study expose several potential weaknesses in medication overuse headache management in Latin America. First of all, although being a member of the IHS Society is not equivalent to providing the best standard of care for headache patients, this organization constitutes the most important scientific society dedicated to headache medicine worldwide. Therefore, the geographical distribution of its members could serve as an indirect indicator of the number of headache-dedicated scientists and evidence-based headache medicine practitioners in the region. We found no registered IHS members in 13 Latin American countries (52% of countries), with a cumulative population of around 97 million inhabitants. Moreover, when considering countries with active IHS members, the median number of IHS members per million inhabitants in Latin America represented only one-third of those observed in a group of Western European countries included for comparison.
Therefore, even if, to the best of our knowledge, the ‘optimal’ number of IHS representatives per country has not been established, our results recognize marked disparities between these two regions. Furthermore, by far, the majority of responders of our survey were clinicians, implying a scarce involvement in headache medicine of other kinds of health providers from this region. The reasons behind the lower number of IHS members in Latin America or their distribution cannot be determined on the basis of our survey. However, we hypothesize that economic as well as cultural factors might be responsible. Analysing what the ideal number of IHS members per country should be, as well as their distribution between different healthcare professionals (i.e. general practitioners, family medicine physicians, primary care physicians, general neurologists, headache specialists, headache specialized nurses, headache specialized kinesiotherapists, basic researchers), merits further research.
Although the ICHD-3-beta criterion for medication overuse headache was the most frequently used tool for diagnosis, several responders referred frequently using a positive response to withdrawal (which is no longer included in the criterion) for the diagnosis of this condition. Indeed, 41% of responders considered the ICHD-3-beta diagnostic criteria ‘ambiguous’, and 33% found them of merely ‘some’ or even a ‘low’ usefulness. Furthermore, on the basis of our analysis, several other concepts seem to be unclear for participants when diagnosing medication overuse headache (Figure 4).
With respect to treatment patterns, our findings show an important lack of uniformity between responders and suggest a very limited usage of therapeutic approaches widely employed in other regions, such as inpatient treatment. This could reflect not only a lack of consensus but also a lack of resources and information.
The outcomes of a European–Latin American joint project, the Continuous Monitoring of Medication Overuse Headache in Europe and Latin America: development and STAndardization of an Alert and decision support System (COMOESTAS) project, have been published. 6,8 –10 The results of such a tremendous effort have provided an invaluable insight into the medication overuse headache problems in Latin America. Remarkably, it revealed that the medications overused in Latin America differ from those in Europe, with a much higher prevalence of ergotamine overconsumption in the former 6 and underlined the reduction in medical expenses resulting from an adequate management of this condition, which is fundamental to increase political awareness. 9 Of note, data from Latin America were obtained from two centres in Argentina and Chile serving mostly middle–high income patients; the situation of the less privileged might be significantly worse.
In medicine, before establishing a therapeutic plan, a proper diagnosis must be obtained. This statement remains valid for healthcare at the population level. If we wish to improve headache care in Latin America, we must start by performing the necessary epidemiological (diagnostic) studies. A culturally, environmentally, and genetically, unique population such as Latin American cannot work on the sole basis of ‘borrowed’ evidence. There is an urgent need to reach consensus and establish region-specific strategies for the management of medication overuse headache as well as other headache disorders in this region. In addition, development of headache specialized educational programmes, fellowships and courses as well as participation of Latin American healthcare providers in the IHS should be incentivized. Countries where there are currently only few or no headache specialists should strive to achieve at least a minimal but thorough coverage in the region. Potential obstacles or challenges include the limited resources, lack of public awareness, and insufficient communication/interaction between healthcare professionals from different countries.
In the future, all the cultural and economic barriers that are currently blocking patients’ access to specialized headache care in Latin America need to be tackled. This is the main goal of the ‘Bridging the Gaps’ initiative, an initiative inspired by the Lifting the Burden campaign and the International Headache Society Global Patient Advocacy Coalition, aiming to improve headache care in Latin America.
Public health relevance
– There are no IHS members in 52% of Latin American countries and, in countries with active members, the median number of IHS members per million inhabitants is significantly less compared to Western Europe. – An important lack of uniformity and a very limited usage of therapeutic approaches widely employed in other regions characterizes medication overuse headache treatment patterns employed by IHS members from Latin America. – The development of headache specialized educational programmes, fellowships and courses as well as participation of Latin American healthcare providers in the IHS should be incentivized.
Footnotes
Acknowledgements
The authors wish to wholeheartedly acknowledge the valuable contribution of Carol Taylor from the International Headache Society in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.