
Abstract
Background:
Temporomandibular disorders (TMD) and headaches are prevalent among the global population. Patients often suffer from both conditions, and they are likely to be associated in a bidirectional way. However, the nature of the association remains unclear. Understanding the epidemiological aspects of the relationship between these conditions could have important clinical implications.
Objective:
To evaluate the prevalence of headaches in TMD patients as well as the prevalence of TMD in patients who suffer from headaches.
Method:
A systematic literature search was conducted using electronic databases. Studies published in English and those that used an acknowledged diagnostic criteria for TMD and headaches were included. Study quality was assessed using the Newcastle-Ottawa scale and meta-analyses were performed to generate pooled prevalence estimates.
Result:
Thirty-one studies met the selection criteria for the review; 16 studies evaluated the prevalence of headache in TMD patients and 15 studies evaluated the prevalence of TMD in headache patients. The included studies were of moderate-to-high quality. Meta-analyses revealed moderate-to-large heterogeneities across included studies. Pooled prevalence estimates from meta-analyses indicated similar rates of headaches in TMD patients and of TMD in headache patients (61.58%, 95% CI 45.26–76.66 and 59.42%, 95% CI 51.93–66.60, respectively). Migraines were more commonly observed in TMD patients (40.25%, 95% CI 35.37–45.23) compared to tension-type headaches (18.89%, 95% CI 12.36–26.44). The prevalence of headaches was particularly high in painful-TMD (82.80%, 95% CI 75.41–89.10).
Conclusion:
Despite large variance in prevalence rates across included studies, this review suggests headache and TMD frequently co-occur, particularly in the case of migraines and muscle related TMD. This association has important clinical, pathophysiological and therapeutic implications.
Keywords
Introduction
Temporomandibular disorder (TMD) is defined as a musculoskeletal disorder that affects the temporomandibular joint and/or masticatory muscles and related structures. 1 These conditions may present with pain in the TMJ and associated anatomical structures. The types of disorders this term includes is discussed later on, but it importantly excludes: non-painful conditions, TMJ pathology which may be congenital as well as traumatic and neoplastic TMJ conditions. TMD is also the most common painful chronic condition of non-dental origin pain in the head and neck region. 2 This condition often results in persistent pain, mandibular functional movement limitations and joint noises. 1 The prevalence of TMD varies between 31% in adults and 11% in adolescents. From the literature, disc displacement with reduction appears to be the most common condition among all TMD types. 3 TMD affects more women (15–26%) than men (8–15%), 4,5 occurs most often between the ages of 20 and 50 and commonly peaks in the fourth decade. 6 –9 According to the diagnostic criteria of the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) 10 and the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD), 11 TMD is categorised into the three groups: arthrogenous TMD (including disc disfunction and joint), myogenous TMD (masticatory muscle disorders), and headache attributed to TMD (Table 1). There are also other TMD diagnostic classifications by the American Association of Orofacial Pain (AAOP), 1 International Association for the Study of Pain (IASP) 12 and International Classification of Orofacial Pain (ICOP). 13 The IASP classification system covers several pain conditions and syndromes. TMD was included in the group of chronic headache and orofacial pain; it has very limited information regarding diagnosis of TMD. 14 The DC/TMD focused on the most common TMD classifications and provided a comprehensive assessment and validated value for each categorisation. The AAOP has now adopted the expanded DC/TMD taxonomy that includes validated diagnostic criteria for the most common TMDs as well as evidence-based criteria for less common TMDs. Recently, the International Headache Society (IHS) has developed the ICOP incorporating the DC/TMD diagnosis and pain taxonomy created by the IASP and also the International Classification of Diseases (ICD-11). 12 Although the ICOP adopts much of the terminology and criteria from DC/TMD, there are differences in terminology and in the distinction between primary and secondary pain.
Classification of TMD subtype.
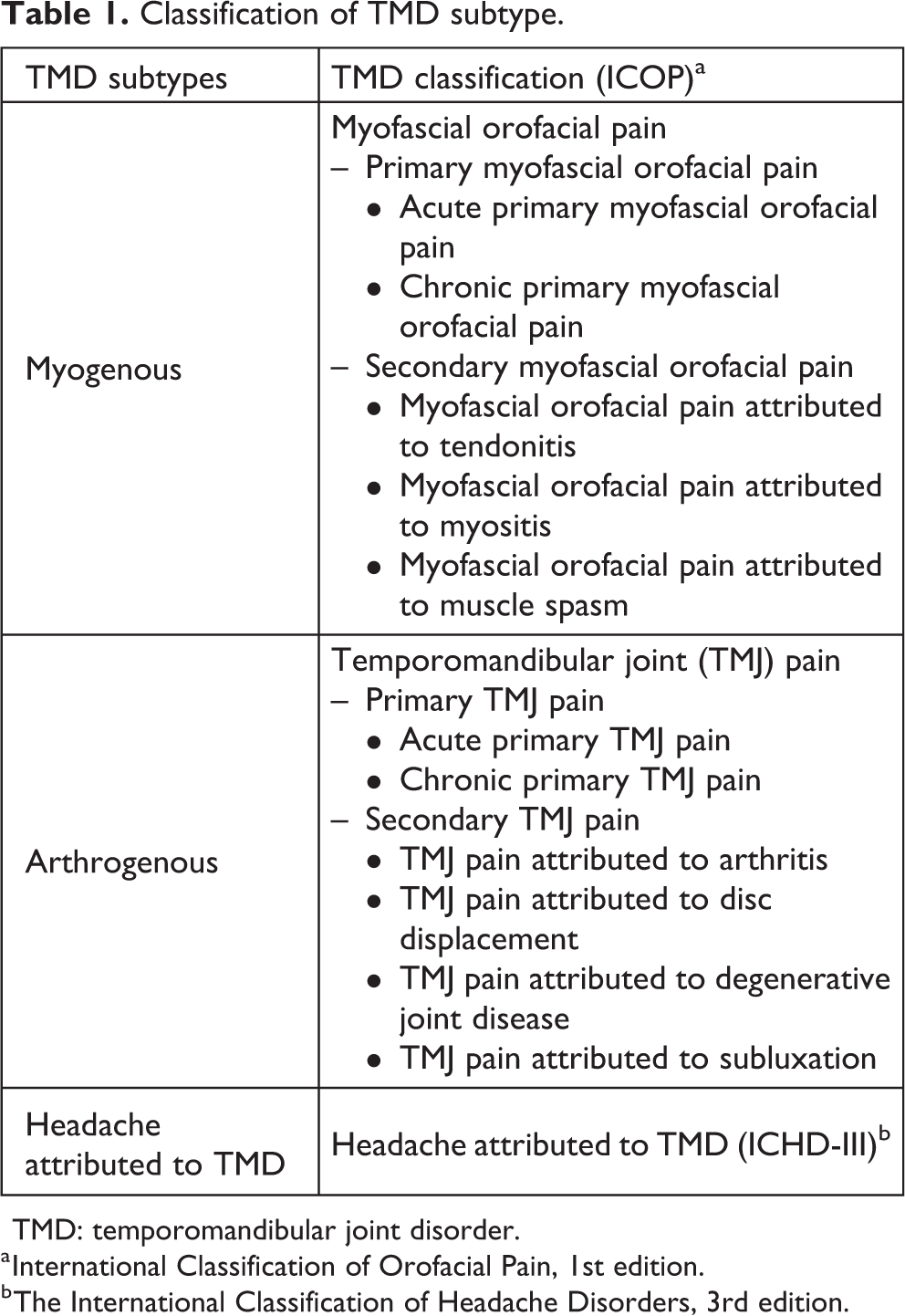
TMD: temporomandibular joint disorder.
a International Classification of Orofacial Pain, 1st edition.
b The International Classification of Headache Disorders, 3rd edition.
Among headache disorders associated with TMD, primary headache disorders such as migraines and tension-type headache, especially in their chronic forms, constitute the most frequently comorbid conditions. Patients with TMD are twice more likely to exhibit a chronic daily headache pattern with or without a migraine biology and a linear relationship between the severity of TMD symptoms and the load of migraine symptoms has been postulated. 15 Additionally, the presence of headache modified by or secondary to TMD is recognised as headache attributed to TMD in the diagnostic criteria of DC/TMD 11 and ICHD-III. 16 The DC/TMD defines headache attributed to TMD as a headache in the temple area secondary to TMD pain modified by jaw movement, function, or parafunction, and familiar headache occurs with provocation testing by the examiner. 11 Contrarily, the ICHD-III criteria did not mention the location of a headache in the temple area. Moreover, they suggested evaluating the temporal relationship, which means that the headache developed after the onset of TMD. 16
The relationship between primary headaches and TMD seems to be bidirectional, suggesting that the presence of the former condition increases the likelihood of experiencing the latter condition and vice versa. 17 Several elements may explain this relationship including gender similarities, peripheral sensitisation of anatomically shared structures, namely the trigemino-vascular system and central sensitisation of central nociceptive neuronal pathways, which may be shared in these conditions. 18,19 However, several aspects of the association between TMD and headache disorders remain unknown. Understanding the epidemiological aspects of this association is pivotal to correctly diagnosing and managing patients with these conditions. To date there are no systematic reviews and meta-analysis solely investigating the prevalence of co-occurring TMD and headache. Our aim is to systematically review the prevalence of this association by reviewing the published literature and perform a meta-analysis.
Methods
The search strategy and protocol were registered and available in the PROSPERO database. 20 Data was collected and a meta-analysis was then performed. This systematic review was conducted and reported according to the PICO model and PRISMA guidelines. 21
Search strategy
The following electronic bibliographic databases were searched: PubMed, CINAHL, Web of Science, MEDLINE, PsycINFO, Scopus, Embase and EBM Review Cochrane (published until April 2020). An additional literature search using Google Scholar, OpenGrey and reference lists of downloaded articles was also carried out. We used the following search terms for TMD: temporomandibular disorder, jaw joint pain, orofacial pain, facial pain, myofascial, aching jaw, mandibular dysfunction, masticatory system disorder, oro-mandibular disorder and combined with ‘AND’, followed by headache terms: headache, head pain and migraine. The search was conducted during April–May 2020.
Eligibility
All articles were accessible, published in English language and there were no time limitations. Observational study designs included prospective studies, case control studies, as well as cohort and cross-study designs. The review included studies with no participants of all ages, genders, and no other excluding factors. In order to be included in the review, the following criteria must have been used to diagnose TMD: Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD), Diagnostic Criteria for Temporomandibular Disorders (DC/TMD), The American Academy of Orofacial Pain (AAOP) and headache diagnosis: The International Classification of Headache Disorders (ICHD) or The International Headache Society (IHS).
Data extraction and analysis
The studies were selected on the basis of the previously mentioned criteria and presence of the proportion of TMD patients with comorbid headache or vice versa. Additionally, association measurement between TMD group and headache group (odd ratio, risk ratio, prevalence ratio) was also collected. One reviewer screened articles initially, and two more reviewers assessed full articles and retrieved data. Any disagreements between reviewers were discussed until a conclusion was reached. The following information was extracted from the included studies: – author and year of publication – study design – sample size and source of the sample – location of study – sample demographics – method of diagnosis of TMD and other pain conditions – outcomes
A meta-analysis was conducted by pooling prevalence rates from relevant studies. The articles pooled for meta-analysis diagnosed headache and TMD according to defined or standardise criteria such as the ICHD for headache and RDC/TMD or AAOP for TMD. The included studies diagnosed TMD by using structural questionnaires and/or clinical assessments. Fixed and random effects meta-analyses were conducted using Freeman-Tukey transformations to calculate weighted summary proportions. 22 Prevalence estimates were presented with 95% confidence intervals and Cochrans’ Q and I2 statistics calculated to indicate the presence of heterogeneity. Random effects modelling was employed to allow for the high heterogeneity values from the variance of included studies (I2 > 50%). 23 Forest plots were produced for all estimates. Analyses were conducted using SPSS (version 26.0, IBM) and MedCalc (MedCalc® Statistical Software).
Study quality
Rating for study quality was assessed by using The Newcastle-Ottawa Scale. 24 The checklist for quality criteria is shown in Table 2. The scoring of all criteria is based on the Newcastle-Ottawa guidelines. We adjusted the measure of sample size by rating one star if the number of participants was greater than or equal to 100 per group, which we considered an appropriate number of representative samples. In the case of difficulties or disagreements, reviewers discussed and reached a consensus.
Guideline for the Newcastle-Ottawa quality assessment scale regarding star awarding to assess quality and bias of studies (out of a total of nine stars).

Results
Search result and data collection
The results from the database searches are shown in Figure 1. Initially, all titles and abstracts were screened. Articles were assessed according to the eligibility criteria and their relevance to the review question. We reported two major groups of studies: headache prevalence in TMD patients (total studies = 16) and TMD prevalence in headache patients (total studies = 15). Tables 3 and 4 describe the characteristics and results of relevant investigations in headache prevalence found in TMD groups, while Tables 5 and 6 demonstrate TMD prevalence among headache patients. The estimated prevalence with confidence intervals for each analytic approach are shown in meta-analysis forest plots (Figures 2 to 10). Quality and risk of bias assessment of include studies is scored and shown in Tables 7 and 8. All published articles achieved equal to or greater than five stars (out of nine stars), representing moderate-to-high quality of the studies in this review.

Search result diagram.
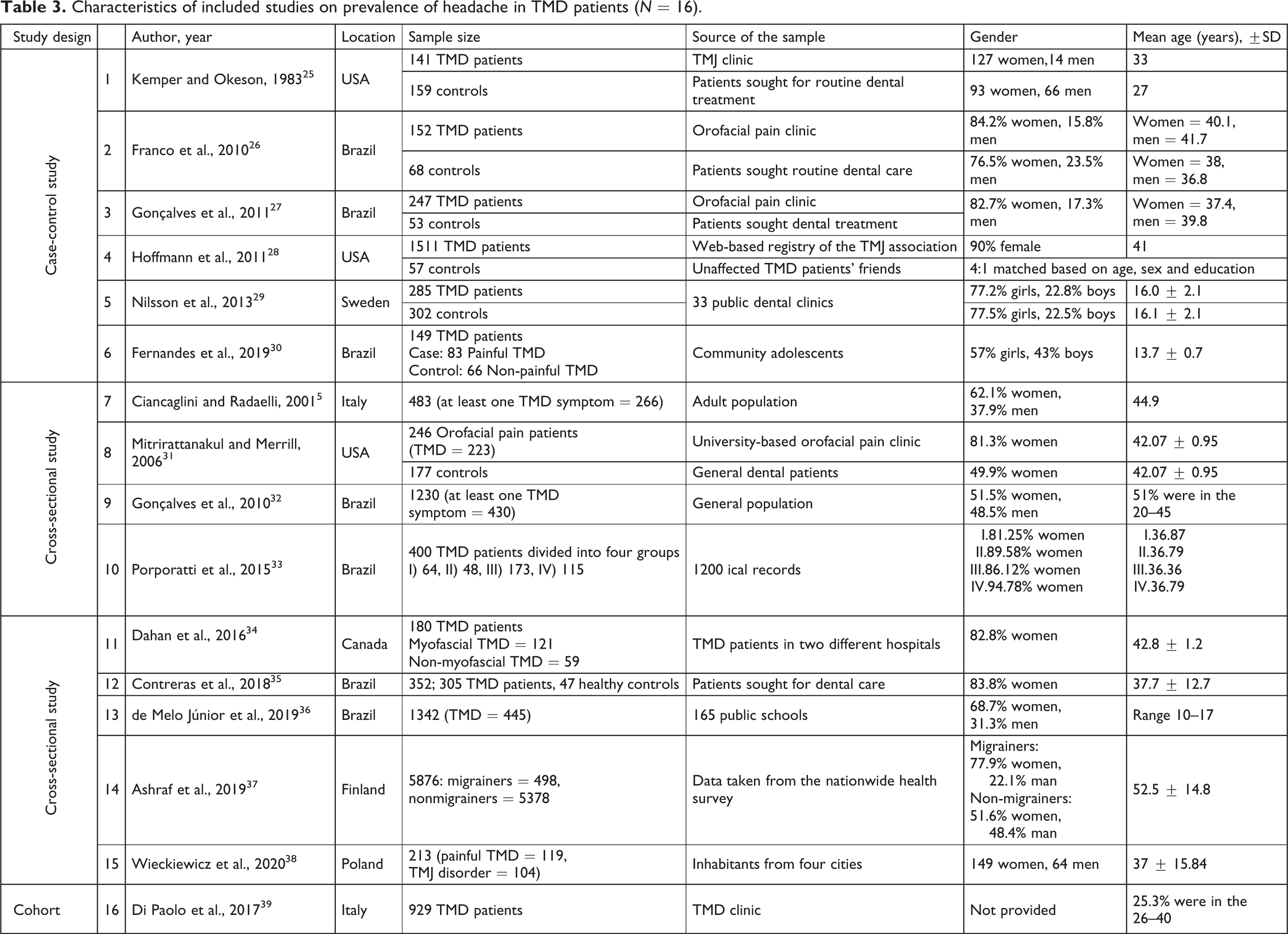
Characteristics of included studies on prevalence of headache in TMD patients (N = 16).
Outcome summary of included studies on prevalence of headache in TMD patients (N = 16).

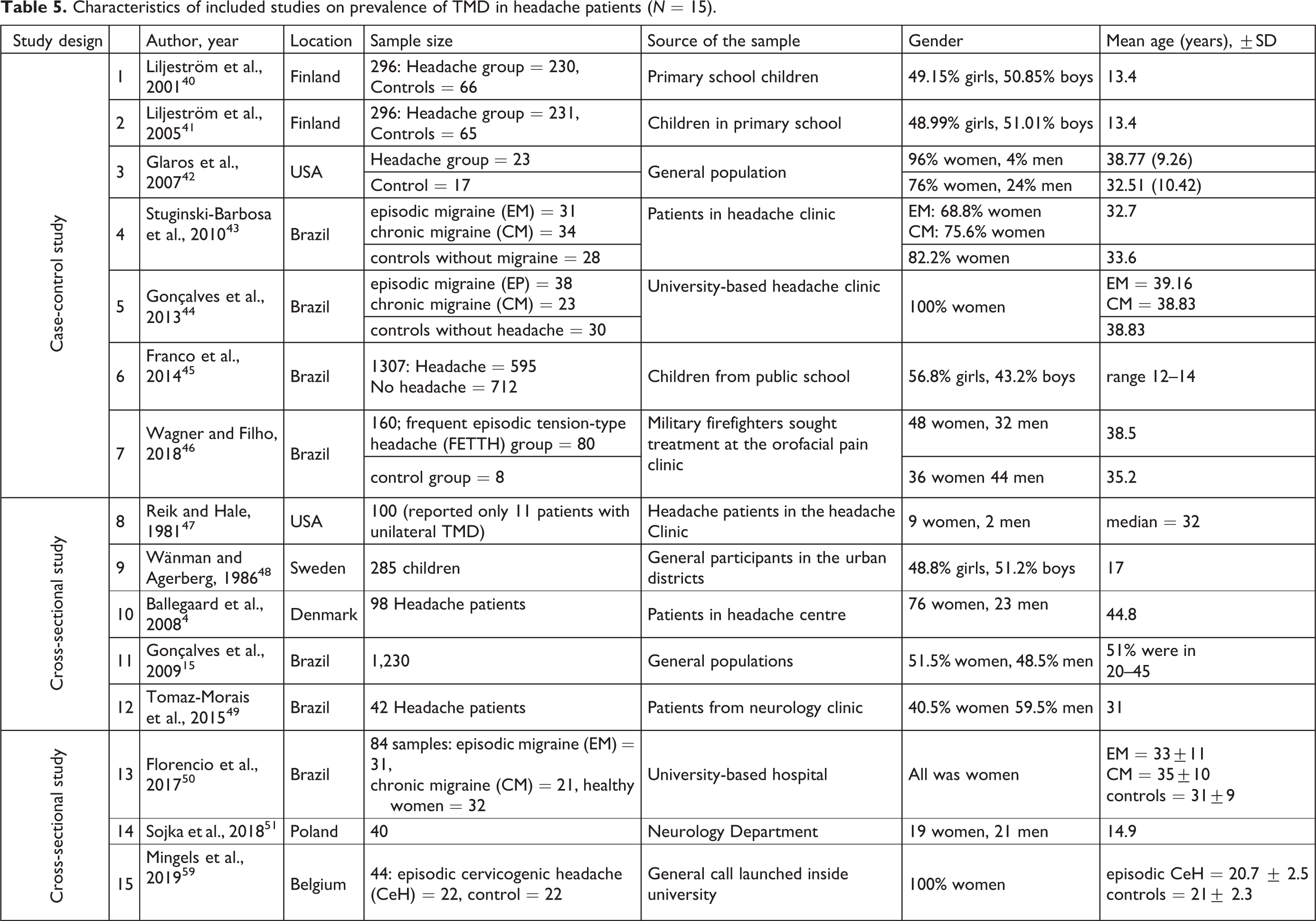
Characteristics of included studies on prevalence of TMD in headache patients (N = 15).
Outcome summary of included studies on prevalence of TMD in headache patients (N = 15).


Forest plot of prevalence of headaches in TMD.

Forest plot of prevalence of headaches in painful-TMD.

Forest plot of prevalence of migraine in TMD.

Forest plot of prevalence of migraine in painful-TMD.

Forest plot of prevalence of tension-type headache in TMD.

Forest plot of prevalence of tension-type headache in painful-TMD.
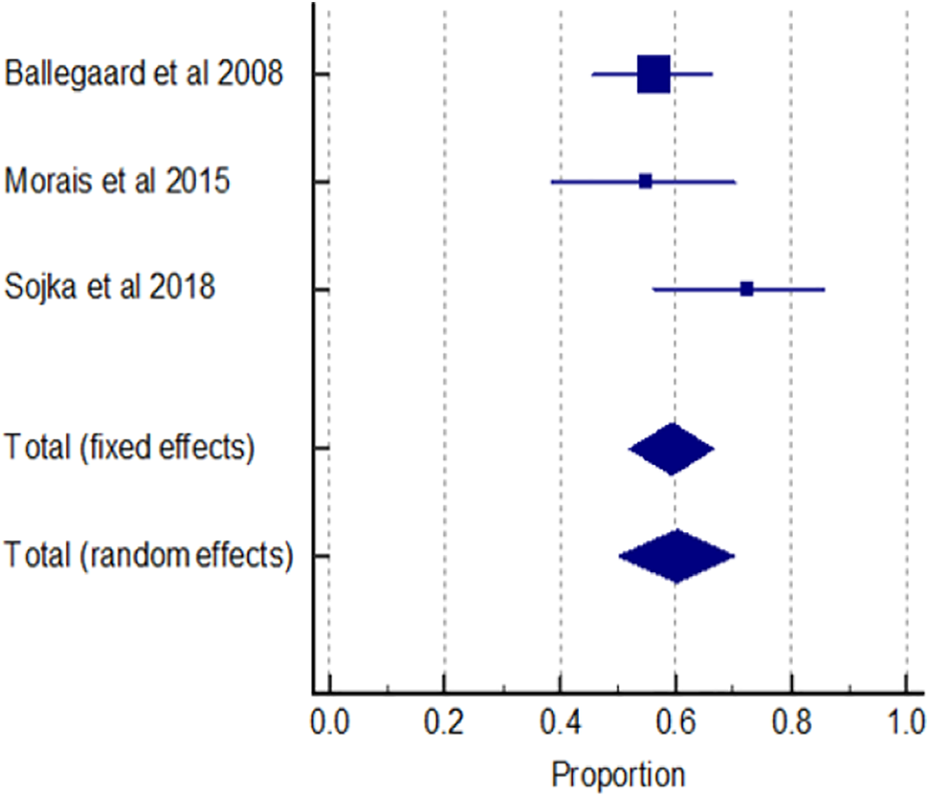
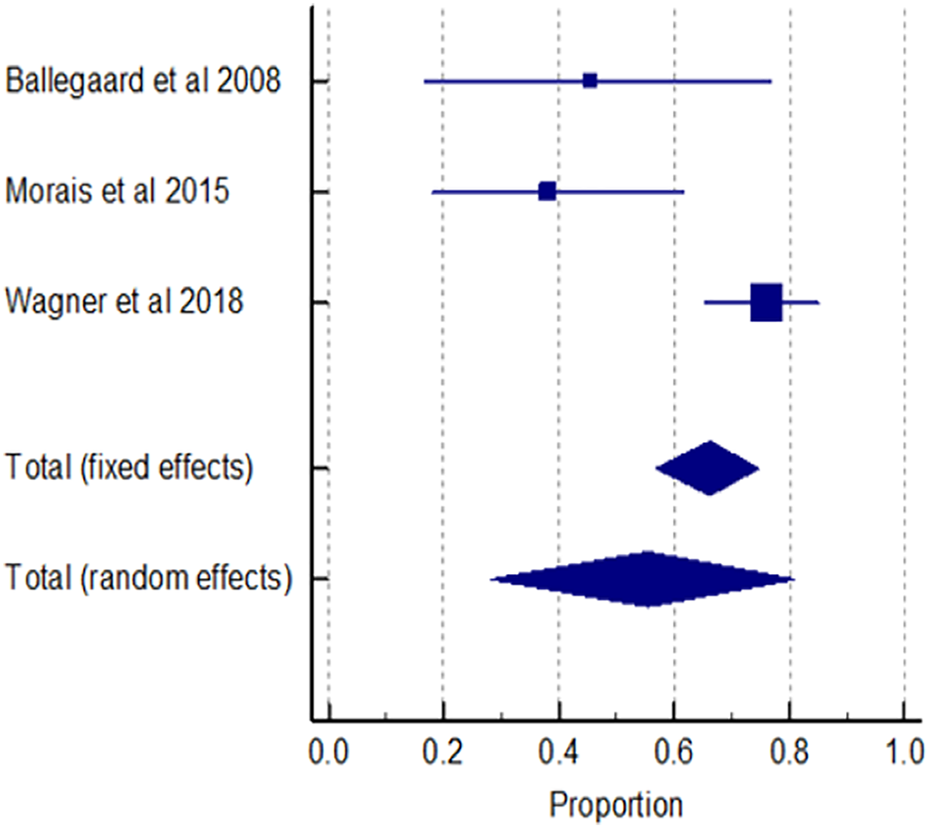
Forest plot of prevalence of TMD in headaches.

Forest plot of prevalence of TMD in migraine.
Forest plot of prevalence of TMD in tension-type headache.
Quality assessment of studies using Newcastle-Ottawa scale* for assessing included studies on prevalence of headache in TMD patients.

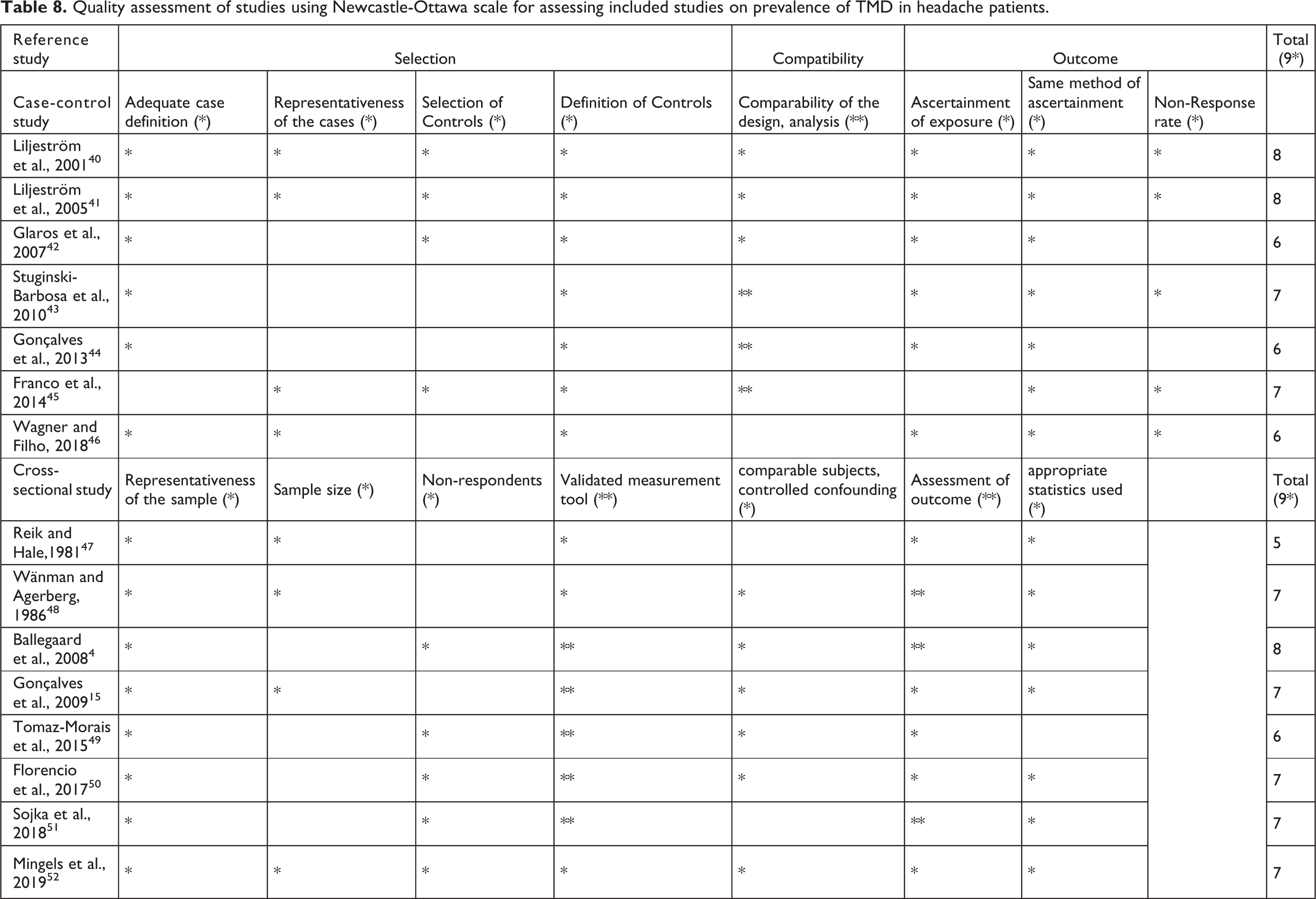
* Guideline for star allocation shown in Table 2.
Quality assessment of studies using Newcastle-Ottawa scale for assessing included studies on prevalence of TMD in headache patients.
Meta-analysis results
Throughout the data extraction process, reviewers found few studies that employed the exact same diagnostic criteria and type of assessment. For example, only two studies 26,27 used the RDC/TMD criteria for clinical TMD diagnosis and questionnaires based on ICHD-II classification for headache. As such, to enable pooling of prevalence data via meta-analytic techniques, we combined findings from those studies that used structural questionnaires or interviews as well as those employing clinical evaluations with clarified or standardised diagnostic criteria.
Prevalence of primary headache in TMD patients
The estimated prevalence of primary headache disorders and their subtypes in the TMD population is presented in Figures 2 to 10. After pooling data from six studies, the overall prevalence of headache in the TMD population was 61.58% (95% CI 45.26–76.66) (Figure 2) and considerable heterogeneity was found among these studies (I2 = 98.62%, 95% CI 98.04–99.03). We additionally investigated the prevalence of two primary headache subtypes and found that 40.25% (95% CI 35.37–45.23) and 18.89% (95% CI 12.36–26.44) of TMD patients suffered from migraine and tension-type headache TTH, respectively (Figures 4 and 6). The heterogeneity test for both analyses indicated moderate to high variability of included studies. Migraine prevalence in TMD resulted in I 2 = 61.19%, 95% CI 0.00–88.94 and TTH prevalence analysis showed I 2 = 85.10%, 95% CI 39.53–96.33.
Further analysis focusing on the painful-TMD group only revealed a prevalence estimate of headache of 82.80%, 95% CI 75.41–89.10 (Figure 3) with I2 = 80.95%, 95% CI 50.13–92.73. Regarding headache subtypes, 47.09% (95% CI 15.50–80.07) and 31.42% (95% CI 26.63–36.52) of painful TMD population experienced migraine and TTH, respectively (Figures 5 and 7). The measure of heterogeneity presented high inconsistency among pooled studies on migraine in TMD (I 2 = 99.32%, 95% CI 99.08–99.50) and moderate inconsistency in pooled studies on TTH in TMD (I 2 = 47.34, 95% CI 0.00–84.57).
Prevalence of TMD in headache patients
Four studies measuring TMD prevalence in headache patients were pooled using a meta-analytic approach. The proportion of TMD in all primary headache patients is presented in Figures 8 to 10. The result showed that 59.42% (95% CI 51.93–66.60) of the headache population had TMD (Figure 8) with a moderate I 2 value of 46.52%, 95% CI 0.00–84.26. In terms of the primary headache subgroup, 59.29% (95% CI 18.82–93.30) of migraine patients and 55.39% (95% CI 28.04–81.09) of TTH patients had TMD (Figures 9 and 10). There were high levels of heterogeneity for studies of TMD prevalence in migraine (I2 = 97.74% (95% CI 96.17–98.67)) and in the investigation of TMD prevalence in TTH (I2 = 84.24% (95% CI 52.88–94.73)).
Discussion
The present systematic review included 31 studies investigating the prevalence of primary headache among patients with TMDs and vice versa. TMD and headache diagnostic criteria differed across the studies because of the evolution of classification systems overtime. The diversity of diagnostic criteria, study designs, as well as population demographics contributed to a challenge in the meta-analytic approach and resulted in a high degree of heterogeneity among pooled studies.
Some of the included studies which used a clinical assessment of patients for headache and TMD 31,33 reported a lower prevalence of these conditions compared to those studies which only used a standalone questionnaire to diagnose these conditions. 26,27 This might be because clinical examination is more validated than questionnaires and results in lower proportion of participants recruited in research. From the perspective of sample size and source, larger samples in population-based studies appeared to indicate a lower prevalence of disorders 28,32,37 compared with smaller studies performed in hospitals. 25,34,35 Even though such studies are more feasible in tertiary care or university-based hospitals, the higher prevalence estimates are often found in epidemiological research due to the higher rate of disease than in the general population.
Most studies in this review used standard and widely acceptable diagnostic guidelines, RDC/TMD, ICHD-II etc., but undertook different methods of assessment which included: self-reported questionnaires, face-to-face or telephone interviews, or formal physical examination. Participants of the included studies had non-specific occupations, were of middle-age and included both genders. However, one study only examined firefighters 46 and there were other studies which only examined young participants 29,30,36,41,45,48 or female adults. 44,50,52 Our review showed that epidemiological studies favoured investigating younger populations and the female population, which may be due to the high prevalence of TMD occurring in these two subgroups. 53 It has been suggested that women are almost two times more likely to suffer from headache compared to men which may account for these differences. 54
Our review showed that the prevalence of headache in the TMD population was 61.58%. Gonçalves et al. 27 reported the highest headache frequencies at 85.42% while Mitrirattanakul and Merrill 31 obtained the lowest of that at 27.24%. Migraine is the most common headache subtype in all TMD patients with a prevalence of 40.25%, which is much higher than the prevalence of headaches in the general population and twice as high as the prevalence of tension-type headache (18.89%). Chronic daily headache (CHD) is an umbrella term, not a diagnosis, comprising of several primary and secondary headache disorders. Despite the lack of a sufficient number of studies in the literature, it seems that the prevalence of TMD in CHD ranged between 5.12% in one study 32 and 35.22% in another study, 27 while the prevalence of CHD in TMD was 66.7%. 15 This suggests that TMD is frequently associated with a daily headache disorder, often migraine and TTH and perhaps other chronic headache disorders, likely chronic migraine maybe associated with TMD.
We performed an additional subgroup analysis of painful and non-painful TMD. A very high prevalence of headache (82.80%) was seen in painful-TMD patients, with small variations between studies (from 73.94% to 86.75%). 30,45 Migraine remains the most common comorbid condition among these patients (47.08%) followed by tension-type headache (31.42%). After pooling studies on non-painful TMD, we found only one study based on the clear definition of non-painful TMD with the recognised assessment – DC/TMD. 38 This study only investigated non-painful TMD in TTH and migraine patients, reporting a proportion of headache in non-painful TMD patients of 78.85%, mostly migraine (31.93%), followed by TTH (20.19%). 38 The prevalence of headache in non-painful TMD is almost as high as the prevalence in painful TMD, with interesting pathophysiological implications that should be explored in future studies. The analysis of studies investigating the prevalence of headache in the subgroup of TMD suggested that migraine is particularly associated with painful muscular TMD, but not with joint-related pain. 37 Individuals with painful muscle-related TMD symptoms had a 1.6-fold higher risk of having migraine than those with other TMD symptoms. In addition, TMD pain, either muscular or joint-related origin, that presented with migraine was also associated with higher migraine frequency and higher prevalence of medication use headache. 37
We also explored the prevalence of TMD in the headache population. Most studies investigating TMD in headache patients rarely classified TMD subgroups; instead, they differentiated by headache subtypes. The results showed that 59.42% of headache patients suffer from TMD, with variation in percentage between 54.76% and 72.50%. 49,51 Migraine patients are slightly more likely to have TMD in comorbidity compared to tension-type headache patient (respectively 59.29% and 55.39%). Although our meta-analysis didn’t include TMD prevalence in non-headache population, it was evident that the prevalence of TMD was higher in patients with headache compared to people without headache; additionally, myogenous TMD patients were more likely to report headaches than those with arthrogenous TMD. 5 The relationship of myogenous TMD and headache was also consistent with Sojka et al.’s study, 51 who found headache patients suffered mostly from muscle dysfunction (40%) and 32.5% from disc displacement with reduction.
The prevalence of comorbid headache in TMD and concurrent TMD in headache from this review are quite similar (61.58% and 59.42%). Despite the large variance across included studies, the review therefore suggests a high co-occurrence of the two disorders in the general and clinical populations. Headache is mostly found in painful TMD sufferers and migraine appears to be most prevalent type of primary headache found among total TMD patients. Besides the main findings, results from measuring association of two conditions also showed significantly higher risk of having headache in TMD group compared to healthy controls. 6,26,29 –32,38,55 However, some of the included studies were conducted in tertiary university-based hospital with small sample sizes. Further epidemiological studies should be performed in large population-based investigation. Other studies focusing on the relationship and mechanism or aetiologies between the two pathologies should also be conducted to provide better understanding and management in patients with both conditions.
The pathophysiology of TMD and headache involves the peripheral and central nervous systems. The trigeminal pathway is a key component in the nociceptive transmission and processing of TMD pain and headache. 10,18 Trigeminal nerve activation is therefore thought to play a significant role in the underlying mechanisms of headache and facial pain disorders, including TMD. 10,18,19 Peripheral and central sensitisation may contribute to the overlap of the two disorders and lead to the difficulties in distinguishing both conditions. Therefore, headache and TMD may occur as separate or overlapping entities. Although there is no evidence to date of a causal relationship between TMD and primary headaches, they may be related in a bidirectional fashion. TMD signs and symptoms may be a perpetuating factor for the primary headache and the primary headache may similarly act as a triggering pain for the TMD condition. 17 This could be a supporting explanation for Gonçalves et al.’s study, 56 which revealed the significant improvement in migraine when TMD was treated in patients with TMD comorbid with migraine.
This review showed a high prevalence of TMD and primary headache disorders in the same individual. This implies that an association between two conditions may exist. This finding highlights the importance routine TMJ evaluation in headache clinics as well as careful headache phenotyping in dental/maxillo-facial settings, to fully assess our patients’ symptoms. When TMD and headache coexist, the management of both conditions may lead to a better outcome and patient satisfaction.
Limitation of the review
This systematic review analysed multiple study designs, including studies without control groups, but the difference in prevalence estimates between patient and control samples related to comorbid conditions were not assessed in the meta-analysis. In addition, only English-language articles were included in our systematic review. Without a language restriction, the review could capture more information and thus eliminate systematic bias. Another point to consider is that the data from this review were pooled across studies using different diagnostic criteria and methods. Therefore, a degree of caution in interpreting the findings is warranted. Although the prevalence estimates obtained show moderate to high heterogeneity, subgroup analyses are of little use when the number of studies included in the meta-analysis is too small to conduct meaningful subgroup analyses. Additionally, this review only estimated the prevalence of headaches associated with TMD. Importantly, chronic pain in localised areas, such as headache and TMD, which may occur concurrently, may be a feature of FMS. Clinicians should not ignore this and should investigate other areas of pain in the body besides headache or TMD pain.
Conclusions
The findings of this systematic review suggest that primary headache disorders are highly prevalent in TMD. Migraine and TTH are the most prevalent headache disorders associated with TMD and they often occur in their chronic subtype. Migraine is the most frequent headache condition associated with painful myogenous TMD. Similarly, a high proportion of patients with primary headache disorders suffers with TMD, though it is unclear which subtypes of TMD are more prevalent in headache patients. Migraine and TTH seem to be the headache conditions more often associated with TMD.
Large population-based studies using uniform diagnostic criteria are needed to clarify the details of the epidemiological association between TMD and headache. However, current available data highlights the importance of their association in terms of similar pathophysiological mechanisms, chronification mechanisms, and overlapping treatments. In light of this research need, future studies should shed light on the epidemiological, clinical, pathophysiological and treatment aspects of this association.
Article highlights
Primary headache disorders are frequent in TMD and vice versa.
Migraine and TTH appear to be the most common headache disorders associated with TMD.
Migraine is the most prevalent headache condition associated with painful TMD.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.