
Abstract
The aim of this study was to examine the prevalence of headache and primary headache disorders like migraine and tension-type headaches among adolescents, and to explore the differences in headache prevalence and frequency by gender and age. This cross-sectional study was conducted in Nord-Trøndelag county, Norway, during the years 1995-97. In total, 8984 (88%) out of 10 202 invited adolescents aged 12-19 years participated in the youth part of the Nord-Trøndelag Health Study [Helseundersøkelsen i Nord-Trøndelag (HUNT)]. The total study population in this study consisted of 8255 individuals after exclusion of invalid questionnaires and students outside the target range of 13-18 years of age. The students completed a comprehensive questionnaire, and one of the questions was whether the students had experienced any headaches during the last 12 months. In addition, 5847 of these students were also subject to an interview in which they were asked whether they had experienced recurring headaches during the last year and, if so, were they classified as migraine (MI), tension-type headache (TTH) or non-classifiable headache. In the total questionnaire-based population, 76.8% reported having had headaches during the last 12 months (69.4% boys and 84.2% girls). Among those who also were interviewed, 29.1% reported having recurrent headaches (21.0% boys and 36.5% girls). The overall 1-year prevalence of migraine was 7%, of tension-type headache 18%, and of non-classifiable headache 4.8%. Higher prevalence rates were found for girls in all age groups and for all headache categories. The overall frequency of recurrent headaches did not vary significantly with age, but girls had significantly more frequent headaches than boys. We concluded that headache in general, and recurrent primary headache disorders like migraine and tension-type headaches, are common somatic complaints among Norwegian adolescents, especially among girls.
Introduction
Headache is one of the most frequent somatic complaints among children and adolescents (1), but the estimated prevalence rates of primary headache disorders like migraine (MI) (2–24) and tension-type headaches (TTH) (2–4, 15, 17, 24–26) vary between different studies. The observed discrepancy is most likely due to differences in classification, study methodology and population samples (27). In epidemiological studies, appropriate case definitions are necessary to obtain reliable and valid diagnoses. The International Headache Society criteria (IHS) (28) provide standardized definitions, but the applicability of the IHS criteria in the paediatric population has been debated (29–38), and some modifications have been proposed (35). Another important aspect is the assessment of the headache diagnoses. Clinical interviews are regarded as the gold standard (39), but clinic-based studies are prone to selection bias and clinical interviews in large population samples are often difficult to apply. Performing short interviews where headache diagnoses are based on recognition of typical headache descriptions has proven to be an efficient and reliable way to identify MI and TTH headache sufferers among adolescents (40).
The main purpose of the present study was to estimate the prevalence of headache and primary headache disorders like MI and TTH headache among adolescents, and to estimate headache frequency among girls and boys in different age groups.
Materials and methods
Nord-Trøndelag, which is one of 19 Norwegian counties, is located in the middle part of the country. The county has about 127 000 inhabitants, and consists of rural and industrial areas with small social differences. The population is scattered, and no city has more than 21 000 inhabitants. The county is, however, a fairly representative cohort of the Norwegian population (41, 42).
During a 2-year period from August 1995 to June 1997, all students in junior high schools (aged 12–15 years) and high schools (aged 16–19 years) in Nord-Trøndelag county in Norway were invited to participate in the youth part of the Nord-Trøndelag Health Study [Helseundersøkelsen i Nord-Trøndelag (HUNT)]. Junior high schools are obligatory in Norway, and even though high schools are not, most adolescents do attend high school. Individuals not registered in high school were identified by the ‘follow-up service’ of the County Education Authorities. In total, 8984 (88%) out of 10 202 invited individuals participated in the study. Young people not participating were mostly not in school on the day of the study, some did not get consent from their parents and some did not want to participate. The study followed the school year instead of the calendar year. As adolescents usually graduate from high school the calendar year they become 19, about half of the 19-year-olds had left school and were not invited. Accordingly, the 19-year-old students in the study population were excluded (n = 382). In addition, some 12-years-olds in the first year of junior high school were excluded because of the low number (n = 126). The participating students completed a self-administered questionnaire with more than 100 health-related items. One of the questions was whether the students had experienced any headache during the last 12 months. The questionnaire was filled in during one school hour. Questionnaires where the headache question had not been answered (n = 221) were excluded, leaving a total study population of 8255. A description of the study population is displayed in Table 1 and has been published previously (41, 42). Within a month after completing the questionnaire, a clinical examination was performed in schools during school hours and included spirometry, weight, height and blood pressure measurements. The intention was to interview the whole population in connection with the clinical examination, but we were not able to start with the interviews until February 1996, which explains the lower number of interviewed individuals. During the ‘missed’ period, both rural and industrial areas were studied and, as shown in Table 1, there were no major differences in sex and age distribution between the total questionnaire-based study population and the questionnaire-based study population that also were interviewed. The total interviewed study population within the age range of 13–18 years was 5847. The interviews were performed at the schools during school hours along with the clinical examination. The nurses asked the students whether they had experienced recurring headaches that were not related to cold, fever or any other disease in the last 12 months. Two typical headache-symptom history descriptions, one for MI and one for TTH, were then read for those students who reported having had recurring headaches, and they were asked to classify their headache(s) according to the descriptions. The students were also given a third alternative (‘non-classifiable headache’), in case none of the two descriptions resembled their own symptoms. If more than one headache type was reported, both types were included in the prevalence count. The average number of days with headaches in the past year was recorded according to the following categories; less than 1 day per month (less than monthly), 1–3 days per month (monthly), 1–5 days per week (weekly), or more than 5 days per week (daily).
Study population
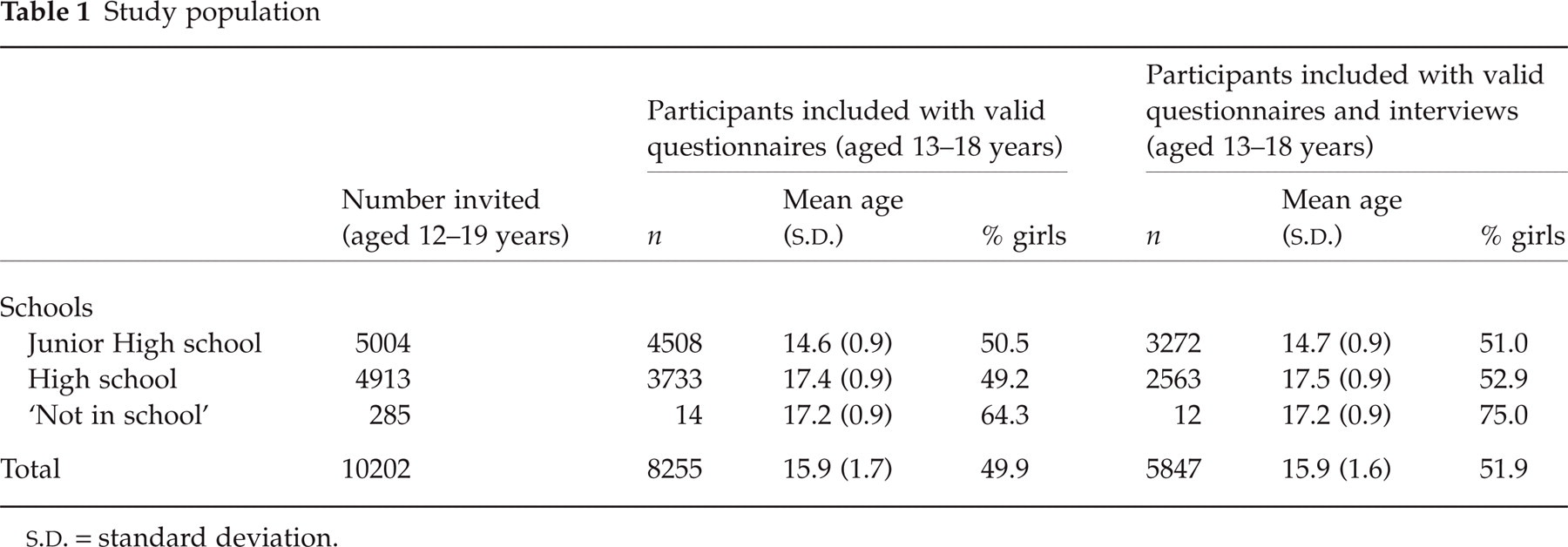
S.D. = standard deviation.
The ‘recognition-based’ headache diagnoses obtained by the nurses have been validated previously against extensive semi-structured interviews by neurologists’ (40). In short, the overall chance-corrected agreement (kappa) between the nurse and the neurologist interviews was 0.76 [confidence interval (CI); 0.66–0.86], which is considered good (43). For MI, the positive and negative predictive values were 89 and 90%, respectively, and the chance-corrected agreement (kappa) was 0.72 (CI; 0.58–0.87). For TTH, positive and negative predictive values were 83 and 91%, respectively, and the chance-corrected agreement (kappa) was 0.74 (CI; 0.62–0.87). For non-classifiable headache, the positive and negative predictive values were 96 and 71%, respectively, and the chance-corrected agreement (kappa) was 0.67 (CI; 0.46–0.88) (40).
A written consent from the parents was required for students less than 16 years of age. The Regional Medicine Ethical Committee and the Norwegian Data Inspectorate Board approved the study.
Statistical analyses
The prevalence rates for the various headache categories were estimated for 2-year age categories for each sex separately. The differences in headache frequencies between the age groups were evaluated with the Kruskall–Wallis test, and the differences between headache frequency between boys and girls were assessed with the Mann–Whitney test. Data analysis was performed with SPSS, version 10.0 (SAS, Chicago, IL, USA).
Results
Out of 8255 students answering the questionnaires, 76.8% reported having had any headaches during the last 12 months (69.4% boys and 84.2% girls). Among the 5847 students that also were interviewed, 77.6% reported in the questionnaire having had any headaches during the last 12 months (69.3% boys and 85.2% girls) and 29.1% reported in the interviews having had recurrent headaches (21.0% boys and 36.5% girls).
The overall frequency of recurrent headaches for boys and girls combined did not change significantly with age (Kruskall–Wallis test, P = 0.81), Fig. 1.

Relative headache frequency of recurrent headaches within different age groups for boys and girls combined. ▪, < Monthly; ▪, monthly; □, weekly; h, daily.
The prevalence of recurrent headaches for girls and boys combined in the present population was 5.5% for less than monthly, 14.1% for monthly, 7.6% for weekly and for 0.5% for daily headache. Weekly and daily headache was more common in girls than in boys (Mann–Whitney test, P < 0.001), Fig. 2.
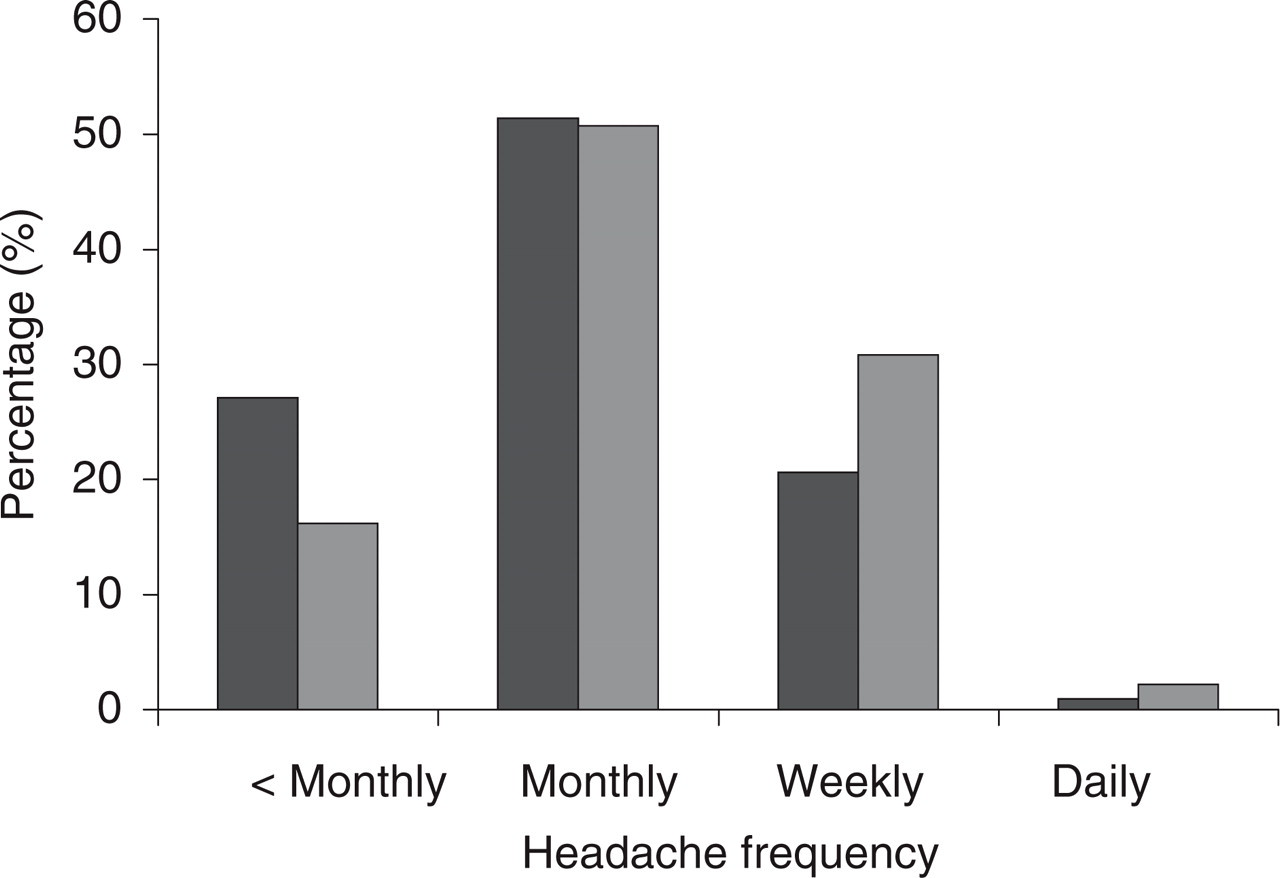
Relative headache frequencies in boys (▪) and girls (□) with recurrent headaches, all age categories combined. Sum of boys = 100%, and sum of girls = 100%.
As shown in Table 2, higher prevalence rates were found for girls in all age groups for MI, TTH and non-classifiable headache. The overall 1-year prevalence of MI was 7.0% (9.1% for girls and 4.8% for boys), of TTH 18.0% (23.2% for girls and 12.5% for boys) and of non-classifiable headache 4.8% (5.4% for girls and 4.2% for boys). There were 69 individuals who had a combination of MI and TTH. The female–male ratio for migraine increased gradually from 1.4 among 13–14 year-olds to 2.6 for 17–18-year-olds.
Prevalence of migraine (MI), tension-type (TTH) and non-classifiable headache (Non-class) among boys and girls (n = 5847)

∗Sixty-nine individuals had a combination of MI and TTH, and these were included in prevalence count in both diagnostic groups.
Table 3 shows headache prevalence data from various epidemiological studies, including the present one.
Results from some recent studies on headache prevalence in adolescents
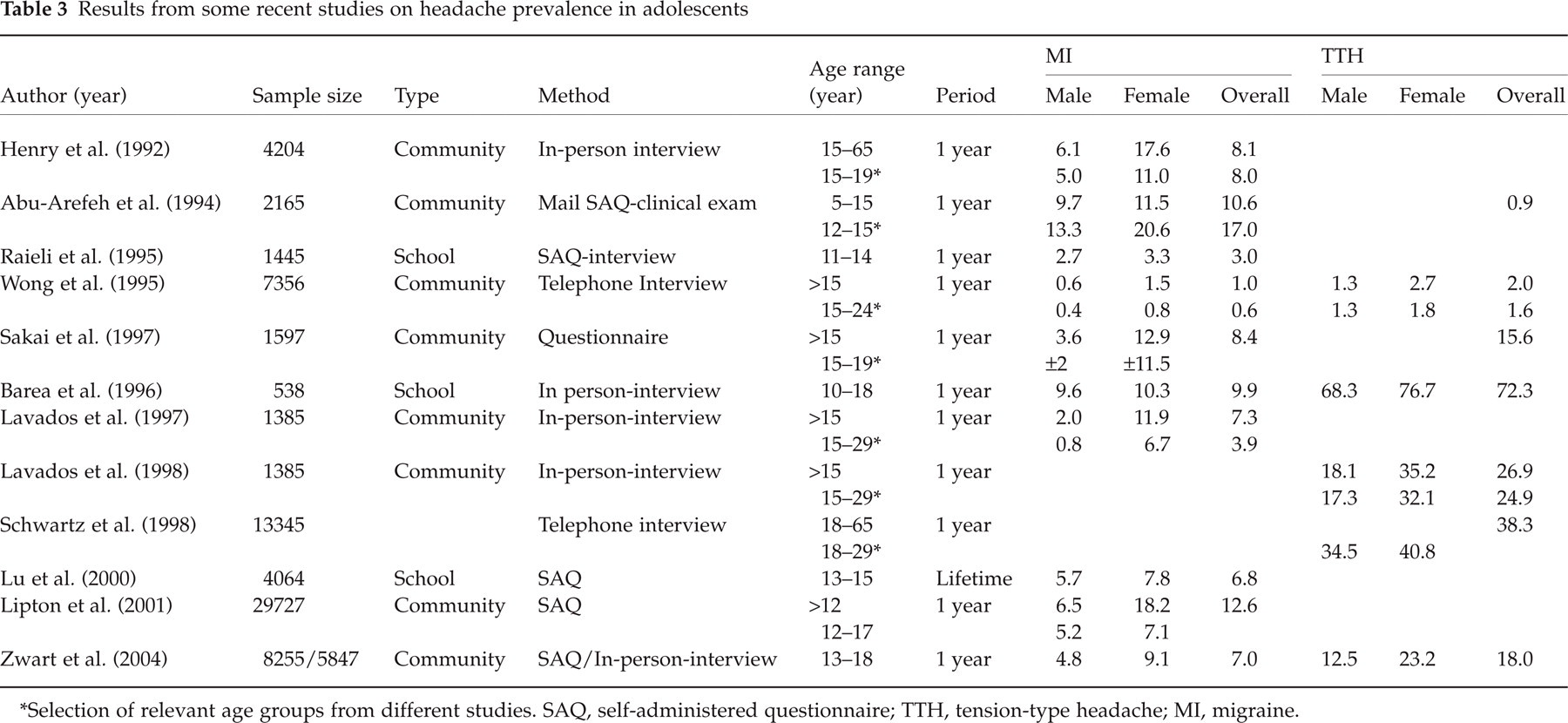
∗Selection of relevant age groups from different studies. SAQ, self-administered questionnaire; TTH, tension-type headache; MI, migraine.
Discussion
This is the first large-scale population-based study among adolescents in Norway assessing the prevalence of recurrent headaches based on validated interviews. The main results from this population-based study are the following: (i) The majority of the students reported having had one or more headaches during the last 12 months, while slightly less than one-third reported having recurrent headaches. (ii) The overall frequency of recurrent headaches did not change with age, but girls had headaches significantly more often than boys. (iii) Among youth with recurrent headaches, migraine, tension-type and non-classifiable headache were more prevalent among girls than boys, in all age groups studied.
Among the interviewed students, only 29% reported having recurrent headaches, whereas the prevalence of any headache during the last 12 months, based on information from the questionnaire was 77%. The large proportion of non-recurrent headaches are probably secondary headache disorders related to cold, fever or other diseases, or they may be very rare primary headache attacks. A clinic-based study among children in a Dutch general practice, found that more than half of the headache episodes reported were related to an infectious disease (44). The recurrent headache rates in the present study are similar to the study by Raieli et al. (16), where 23.9% of the students aged 11–14 years reported recurrent headaches, with higher rates for girls (28.1%) than boys (19.9%). In this study, 80% of the headache population had one or more attacks per month (16), which is the same as in the present study, where only 20% of those with recurrent headaches reported having headaches less than monthly. Sillanpää reported among 14-year-old students that 41% had headaches less than 10 times during the last 12 months (20). Thus, one might suspect that students in the present study with less frequent headaches, of all types, do not define their headaches to be recurrent. This would accordingly result in an underestimation of the prevalence rates. Significantly more girls had frequent headaches compared with boys. Others have reported a female preponderance of recurrent headaches (18, 19, 24, 45), and higher rates of any headache among girls (84%) than boys (69%) in the present study are also in accordance with other studies (2, 4, 7, 10, 12, 13, 17–20, 23, 45).
The overall 1-year prevalence of migraine in the interviewed population was 7.0% (9.1% for girls and 4.8% for boys), which is consistent with most studies from the Western countries utilizing the IHS criteria (Table 3). A predominance of migraine among girls after the age of 13 has been well documented and is reflected by the female–male ratio. Linet et al. (10) reported a female–male ratio of < 2 at the age of 12, with an increase thereafter, which is in accordance with our results. The female–male ratio increased from 1.4 in the youngest to 2.6 in the oldest age group.
For TTH, the overall 1-year prevalence in the present interviewed population was 18.0% (23.2% for girls and 12.5% for boys). There are few studies reporting the prevalence of TTH among adolescents, and the prevalence data vary as displayed in Table 3. Lavados et al. (9) from Chile found among 15–29-year-old individuals an overall prevalence of episodic TTH of 23.7%, higher among girls (30.5%) than boys (16.5%). Schwartz et al. (26) found, in a study from the United States, a prevalence of episodic TTH in the youngest age group (18–29 years) of 34.5% in men and 40.8% in women. Among subjects between 15 and 24 years of age in Hong Kong, Wong et al. reported TTH to be 2–3 times more frequent than migraine (24). The prevalence rates are, however, lower than studies from the Western part of the world. Higher prevalence rates have been reported by Barea et al. (4), while Abu-Arefeh et al. (2), in a study from the UK, reported an overall prevalence of TTH of 0.9%. In this study, however, only children with severe headaches were invited for clinical interviews. Differences in study methodology may accordingly explain some of the discrepancy, but it may be that the relatively low prevalence rates for TTH in the present study is due to the fact that individuals with only sporadic TTH do not report having recurrent headaches. In addition, the recognition-based technique may underestimate the occurrence of more than one headache, thus those with MI may not report also having TTH (40).
The high participation rate in the questionnaire-based part of the study indicates that the study cohort represents the population fairy well, and that no serious selection bias was present. It also seems reasonable to assume that the prevalence rates of recurrent headaches based on data from the interviewed population are fairly representative. There were no systematic selection of subjects and no major differences in age and sex distribution between the total questionnaire-based study population and questionnaire-based study population that were also interviewed. It is, however, possible that students absent from school, and accordingly not included in the study, might have more health problems than the responders, which in turn would underestimate the observed prevalence rates of different headache disorders.
A total of 4.8% of the interviewed population were categorized as non-classifiable headache (5.4% for girls and 4.2% for boys). Subjects who reported their headache not to be consistent with either MI or TTH were included in this group. Future follow-up studies will provide information about the prognosis of these primary headache disorders.
In conclusion, this population-based study shows that headache in general and recurrent primary headache disorders like migraine and tension-type headaches are common somatic complaints among Norwegian adolescents, especially among girls.
Footnotes
Acknowledgements
The Nord-Trøndelag Health Study (The HUNT study) is a collaboration between The HUNT Research Centre, Faculty of Medicine, Norwegian University of Science and Technology (NTNU), Verdal, The Norwegian Institute of Public Health and Nord-Trøndelag County Council. This part of the study (The Head-HUNT Youth Study) was also supported by an unconditional grant from Pfizer, Norway. John-Anker Zwart receives a research grant from the Norwegian Research Council.