
Abstract
To investigate overlaps between headache and temporomandibular disorders (TMD) in a clinical headache population and to describe the prevalence of TMD in headache patients, 99 patients referred to a specialized headache centre were diagnosed according to Research Diagnostic Criteria for TMD (RDC/TMD) and classified in headache groups according to the International Classification of Headache Disorders, second edition for headache diagnoses in a blinded design. The prevalence of TMD in the headache population was 56.1%. Psychosocial dysfunction caused by TMD pain was observed in 40.4%. No significant differences in TMD prevalence were revealed between headache groups, although TMD prevalence tended to be higher in patients with combined migraine and tension-type headache. Moderate to severe depression was experienced by 54.5% of patients. Patients with coexistent TMD had a significantly higher prevalence of depression—most markedly in patients with combined migraine and tension-type headache. Our studies indicate that a high proportion of headache patients have significant disability because of ongoing chronic TMD pain. The trend to a higher prevalence of TMD in patients with combined migraine and tension-type headache suggests that this could be a risk factor for TMD development. A need for screening procedures and treatment strategies concerning depression in headache patients with coexistent TMD is underlined by the overrepresentation of depression in this group. Our findings emphasize the importance of examination of the masticatory system in headache sufferers and underline the necessity of a multidimensional approach in chronic headache patients.
Introduction
Both headache and temporomandibular disorders (TMD) are very prevalent conditions in the general population (1–13), representing a serious health problem and a major impact on society and on the quality of life of affected individuals (14–16). TMD are defined as a cluster of symptoms and signs involving masticatory muscles, the temporomandibular joints (TMJs) or both (17, 18). Population-based studies have reported the prevalence of TMD to be from 8% to 15% for women and from 3% to 10% for men (8), indicating that TMD are major causes of non-dental pain in the orofacial region. The aetiology of TMD is still not well understood. It is generally accepted that they are multifactorial conditions with both psychosocial and neurobiological aspects as important aetiological co-factors (19).
The most widely internationally used tool for TMD diagnosis is the Research Diagnostic Criteria for TMD (RDC/TMD) developed by Dworkin and LeResche (17) and is useful due to its high degree of reliability (20–26).
The International Classification of Headache Disorders, second edition (ICHD-II) contains both classification and diagnostic criteria for headache disorders. This system is widely accepted as a standard for classification of headache disorders (27).
Several clinical and epidemiological studies have demonstrated an association between headache and TMD, indicating that individuals with headache and TMD have a number of symptoms and signs in common (11, 28–42). Despite this, the exact relationship between those two entities is still largely unknown.
The objective of this study was to investigate the overlap between primary headaches and TMD in a clinical headache population and to describe the prevalence of TMD in headache patients using the RDC/TMD questionnaire and examination method.
Materials and methods
Participants
All patients referred to the Danish Headache Centre (DHC) at Glostrup Hospital from a neurological pre-consultation in a 6-month period, who were > 18 years old and gave verbal consent for participation in the study were candidates for inclusion. A total of 100 patients were included. The following patients were excluded: patients unable to communicate in Danish, unable to cooperate during the examination process and pregnant patients. One patient was excluded due to incomplete filling of the questionnaire based on poor language skills in written Danish.
The DHC is a tertiary headache centre specializing in interdisciplinary treatment of patients with severe or rare types of headache or facial pain. Patients are referred from all parts of Denmark as well as from abroad, from primary care physicians and from neurologists.
Patients were selected consecutively in the DHC after a systematic process. In the DHC all patients are initially examined by neurologists and subsequently referred to an interdisciplinary team. After the initial consultation, patients were examined by the same investigator (V.B.), who was blinded to all information about headache diagnosis and characteristics. In the waiting area the patients were introduced to possible participation in the study. If more than one patient was present in the waiting area, the first patient on the list of consultations was asked to participate. If this patient refused to participate, the second listed patient was asked, and so on. Informed oral consent was obtained from all patients prior to participation.
ICHD-II
As part of the planned consultation, patients were diagnosed according to ICHD-II by different neurologists. Diagnosis was based on standardized record forms and prospective diagnostic diaries for at least 4 weeks. The neurologists had no knowledge of the inclusion in the study. After finalization of the clinical part, one neurologist (P.T.S-H.) classified the patients into the following ICHD-II groups: migraine with and without aura (MIG), cluster headache (CH), chronic post-traumatic headache (CPOH), tension-type headache (TTH), medication overuse headache (MOH), trigeminal neuralgia (TN) and headache unspecified. P.T.S-H. was blinded to the outcome of the TMD investigations.
RDC/TMD questionnaire (axis II) and examination (axis I)
The RDC/TMD is a diagnostic tool for advanced TMD research, standardizing evaluation and classification of patients with TMD containing both measurement for physical disorder factors and psychosocial illness impact factors, axis I and axis II (17). The RDC/TMD is based on the consensus of world leaders among researchers and clinicians and includes operationalized diagnostic criteria. Importantly, it has also been subject to extensive testing in terms of reproducibility (43, 44). The clinical examination takes about 10–15 min, whereas the questionnaire may take about 30–45 min.
The purpose of the questionnaire is to assess and classify the global severity of the pain condition in terms of: pain intensity, pain-related disability, depression and non-specific physical symptoms. Information on sociodemographic factors is also included (17). The questionnaire can be found in its full form at http://www.rdc-tmdinternational.org.
Patients were asked to fill out the questionnaire with the purpose of obtaining knowledge on TMD among headache patients. The investigator was available for questions, but did not otherwise interfere. The results from the questionnaire were analysed after the TMD examination in order to keep the investigator blinded.
If the patient reported any TMD pain in the previous month the results from the questionnaire were scored according to the Axis II Scoring Protocol for Graded Chronic Pain (17).
The RDC/TMD examination was carried out by V.B., who was trained and calibrated in a standardized examination procedure at the DHC and at the Dental School in Aarhus. Interobserver reliability was tested in this setting.
The examination included measurement of the range of mandibular motion, assessment of pain in joints and muscles in movement, and palpation of clicks or crepitus on movement of the mandible. The following areas were palpated bilaterally (tenderness graded as no pain, mild pain, moderate pain and severe pain): posterior/middle/anterior temporal muscle, superior/middle/inferior masseter muscle, posterior mandibular region, submandibular region, lateral/posterior pole of the temporomandibular joint, lateral pterygoid area and tendon of temporal muscle.
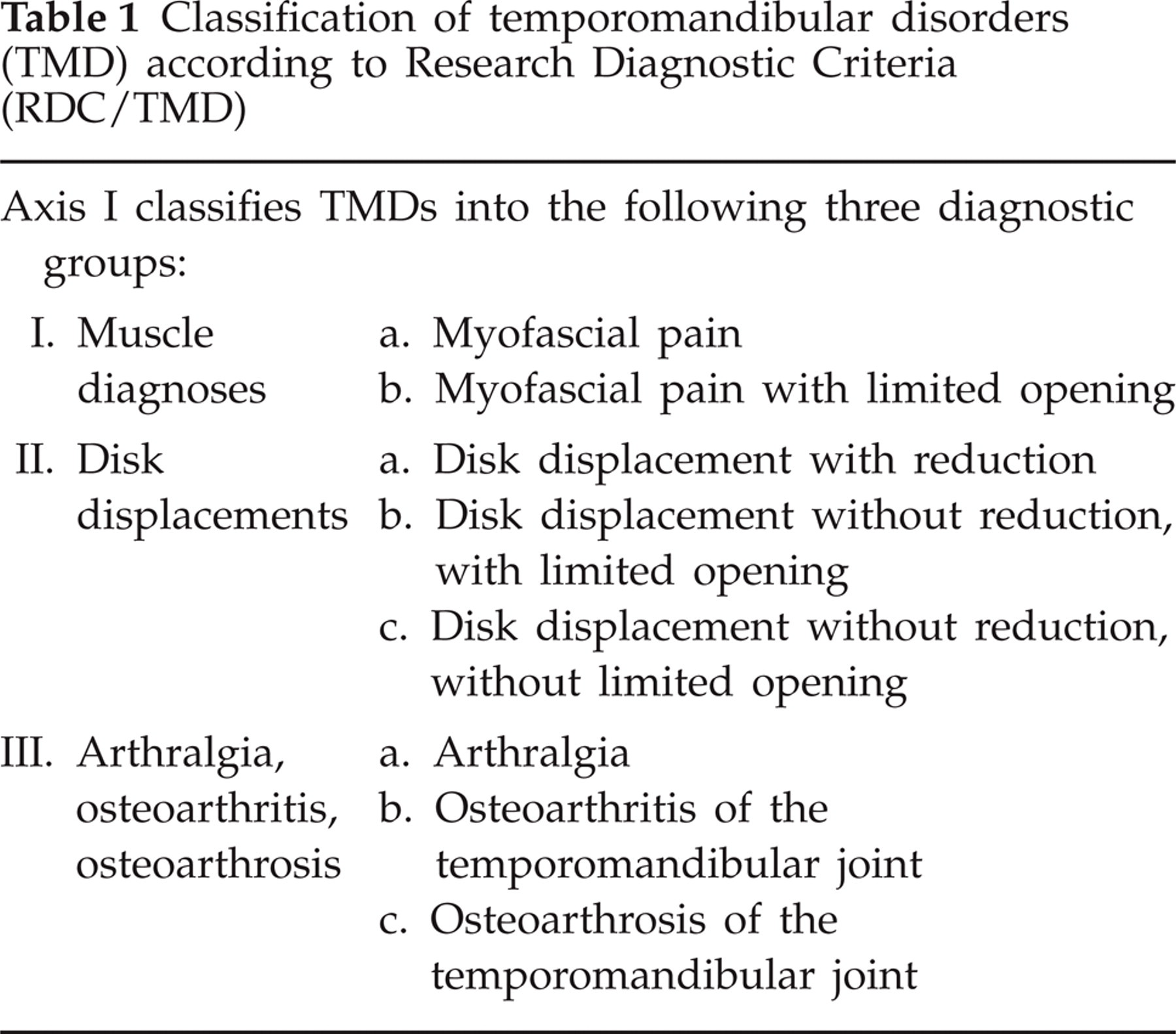
Using the observed signs and symptoms, the RDC/TMD specifies algorithms with classification into three main groups of TMD diagnoses with subdivision into eight subgroups (Table 1). This system of classification deals only with the most common TMD diagnoses.
Classification of temporomandibular disorders (TMD) according to Research Diagnostic Criteria (RDC/TMD)
Statistical analysis
Comparison of groups was performed with Fisher's exact test and χ2 test. The level of significance was set at P < 0.05.
Results
A total of 99 patients (76 female, 23 male) with a mean age of 44.8 years (range 18–88 years) participated. Table 2 shows the representation of different headache diagnoses in the study population. Combined migraine and TTH, or combined migraine, TTH and MOH were the most prevalent combination of diagnoses (each 20.2%); 60.7% of patients had more than one headache diagnosis. Migraine was the most prevalent single diagnosis (15.2%), followed by TTH (11.1%).
Characteristics of the headache population (IHCD-II diagnoses) (n = 99). Values in percentages are given in parentheses

Females were overrepresented in all headache groups, with the exception of CH, combined migraine and MOH, or combined TTH and MOH (Table 2). No significant differences in age distribution between groups were found.
Due to the small number of subjects in the groups, non-classifiable headache (n = 1) and TN (n = 4) statistical tests were not conducted in these groups.
RDC/TMD
All 99 patients completed the RDC/TMD questionnaire. Ninety-eight patients were examined according to the RDC/TMD examination, as one patient refused to participate due to serious pain in palpated areas. A TMD diagnosis (axis I) was identified in 55 out of 98 patients (56.1%) and a total of 82 patients (82.8%) reported facial pain according to the RDC/TMD axis II chronic pain grade classification.
TMD diagnosis (axis I)
Of the 55 patients with a TMD axis I diagnosis, 46 were female (83.6%) and nine male (16.4%), but no significant gender difference could be detected (χ2 test; P = 0.07). The mean age was 44.6 years (range 18–70 years) for patients diagnosed with TMD, which was not significantly different from non-TMD patients. The prevalence of TMD diagnoses is shown in Fig. 1.

Prevalence of temporomandibular disorder (TMD) diagnoses in 98 headache patients diagnosed according to the Research Diagnostic Criteria (RDC/TMD). I, muscle diagnoses; II, disk displacements; III, arthralgia, osteoarthritis, osteoarthrosis.
The most prevalent diagnosis, myofascial pain, was diagnosed in 46 patients (46.9%). Discus displacement with reduction was diagnosed in seven patients (7.1%), and three of these had coexisting myofascial pain. Arthralgia, osteoarthritis and osteoarthrosis were diagnosed in 10 patients (10.2%). Three had arthralgia (two with coexistent myofascial pain), three had osteoarthritis (one with coexistent myofascial pain) and four had osteoarthrosis (two with coexisting myofascial pain). No significant difference in age distribution between the TMD groups was found.
The prevalence of TMD diagnoses in relation to headache diagnosis indicated differences between the groups. The highest percentage of TMD (75%) was observed in patients with a combination of migraine and tension-type headache (MIG+TTH), and the lowest percentage (45.4%) was observed in patients with TTH as a single diagnosis (Table 3).
Prevalence of patients with temporomandibular disorder (TMD) diagnoses (axis I) in the headache groups: migraine with and without aura (MIG), tension-type headache (TTH), MIG+TTH and MIG+TTH + medication overuse headache (MOH). Values in percentages are given in parentheses

Total prevalence of TMD in the headache groups is tested for significant differences compared with the rest of the headache population (performed with two-tailed χ2 test).
The prevalence of TMD in the MIG+TTH group tended to be higher than that in the rest of the headache population (χ2; P = 0.0501). However, none of the differences in TMD prevalence between the headache groups was significant (Fisher's exact test; P > 0.05). Thirty-one patients had other types of headaches (or headache combinations) than those mentioned above; 20 patients with different combinations of headaches, six patients with CH (two with TMD) and five with CPOH (three with TMD). Due to small number of subjects in each subgroup, these patients were omitted from statistical tests.
Chronic pain grade classification and depression (axis II)
Of the 82 patients reporting facial pain according to the RDC/TMD axis II chronic pain grade classification, 79.3% were female and 20.7% were male. The mean age was 44.4 years (range 18–88 years). The number of subjects in each group (I–IV) did not differ significantly, nor did the distribution of gender (Fig. 2).
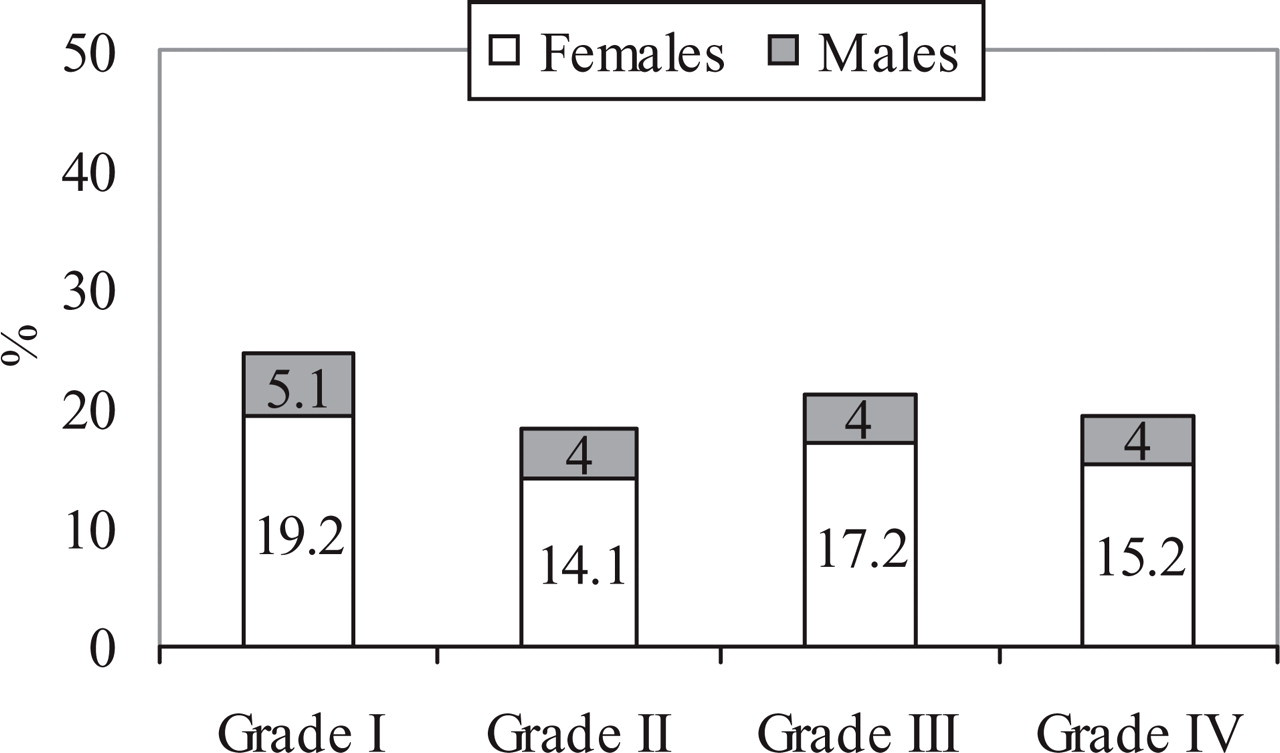
Prevalence of grade I–IV on the chronic pain grade classification in 99 headache patients scored according to the Research Diagnostic Criteria/ temporomandibular disorder (RDC/TMD). Grade I, low intensity; Grade II, high intensity; Grade III, moderately limiting; Grade IV, severely limiting.
Table 4 shows the distribution of chronic pain in the different headache groups. A significant difference regarding grade III was seen between TTH and the combined group MIG+TTH (Fisher's exact test; P = 0.028).
Prevalence of patients with different grades of chronic pain according to the chronic pain grade classification (axis II) in the headache groups: migraine with and without aura (MIG), tension-type headache (TTH), MIG+TTH and MIG+TTH + medication overuse headache (MOH). Values in percentages are given in parentheses

All 99 patients completed the scale for depression and non-specific physical symptoms. Only prevalence of depression was analysed in this study.
The overall prevalence of moderate to severe depression in the headache population was 54.5%. A significantly higher prevalence of moderate to severe depression was observed in headache patients with coexistent TMD, as 70.9% of patients with coexistent TMD had moderate to severe depression, compared with 34.1% of patients without coexistent TMD (χ2; P = 0.0002). The prevalence of moderate to severe depression in the different headache subgroups is shown in Fig. 3, showing a significant overrepresentation of depression in patients with combination headache (MIG+TTH+MOH and MIG+TTH) and coexistent TMD.
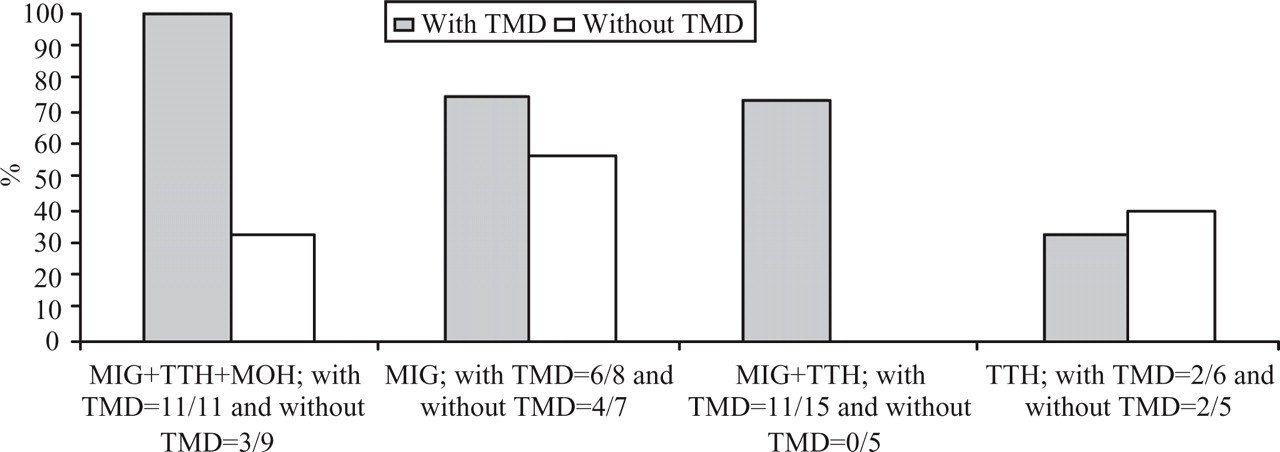
Percentage prevalence of moderate to severe depression in different headache groups [+/− coexistent temporomandibular disorder (TMD)]. Groups with significant difference between patients with and without coexistent TMD are migraine with or without aura plus tension-type headache plus medication overuse headache (MIG+TTH+MOH), P = 0.002, and MIG+TTH, P = 0.008.
Discussion
Most headache disorders and TMD are not well understood in terms of aetiology. A possible relationship between the conditions has been debated for many years, but a clear causal association is still lacking.
The reported 1-year prevalence of headache in the general population using IHCD-II is 10.2–23.6% for migraine and 36–86.5% for TTH (4, 5, 10, 13, 45–55). A 1-year prevalence of migraine of 15.5% and of TTH of 86.5% in a young Danish population has recently been demonstrated (13).
The range of reported TMD prevalence in the general population is wide, probably because many different criteria and methods are used. In a meta-analysis from DeKanter et al., the average prevalence of clinical signs and symptoms was 44% in population surveys (12). A very recent study has reported the incidence of clinical signs and symptoms of TMD at 49.9% (6). To our knowledge, large-scale population surveys based on RDC/TMD criteria do not exist. Smaller studies have recently been performed reporting the prevalence of TMD as 27% (56, 57).
TMD diagnoses (axis I)
The prevalence of clinically assessed TMD in the present population was 56.1%, indicating a probable higher prevalence of TMD in headache populations than in the general population. This is comparable to earlier studies on TMD in headache patients. Schokker et al. found that 66% (n = 50) of patients diagnosed with headache had signs and symptoms of TMD (34). Likewise, a population study has reported that approximately 70% of subjects (n = 483) with headache also had TMD symptoms (11). A very recent study reported that a significantly higher proportion of headache patients (n = 23) received a RDC/TMD diagnosis compared with non-headache controls (58). Larger patient population studies with an age- and gender-adjusted control group have to be carried out to confirm this overrepresentation of TMD in headache populations.
A tendency towards a higher prevalence of women in TMD compared with non-TMD patients was shown in our study. Especially, TMD pain has been shown in some studies to be approximately twice as common in women (8, 12, 59). In this study the overall skewness of the male/female ratio was 1:3.3. This may reflect a higher female acceptance of participation, in addition to a higher rate of females in the patient population at the DHC (1:2.4). A female preponderance in headache is well established, with a 1:2–3 ratio for migraine and a 1:1.5 ratio for TTH in the general population (51).
The most prevalent TMD diagnosis in this headache population was myofascial pain (group I) (46.9%); 10.2% had arthralgia, osteoarthritis and osteoarthrosis (group III) and 7.1% had disc displacement (group II).
In a recent multicentre study based on RDC/TMD results from 10 international TMD centres, the median prevalence of myofascial pain was 59%. Disc displacement was 33% and arthralgia, osteoarthritis and osteoarthrosis was 29% (43). All studies have confirmed that muscle disorders are the most prevalent. Our population differed from the general TMD population with respect to group II and III diagnoses, whereas the prevalence of myofascial pain was very similar among the studies.
Results from non-TMD populations using RDC/TMD are infrequent. A Finnish study with a sample (n = 241) of non-patients found myofascial pain in 14%, disc displacement with reduction in 18% and no arthralgia, osteoarthritis and osteoarthrosis (56). Gesch et al. did not use RDC/TMD, but found a prevalence of masticatory muscle tenderness of 15%, TMJ tenderness of 5%, TMJ sounds 25%, limited mouth opening 9%, pain upon movement of the mandible 1% and irregular jaw movements 28% (6).
Pain in the temporomandibular region is known to be relatively common, recently confirmed by Ciancaglini and Radaelli, where 15.2% in a population survey suffered from TMD pain (11). In 1993 the prevalence of self-reported TMJ disorders in a Danish health survey was 3% (2).
In conclusion, our study has indicated that the prevalence of TMD pain, in particular, is higher in headache populations than in the general population, whereas other non-painful TMD diagnoses were very similar represented.
Our study has shown that the prevalence of TMD in the combined migraine and TTH group tended to be higher than the prevalence in the rest of the population. Patients with TTH (single diagnosis) tended to have the lowest prevalence of TMD (45.4%). Studies with larger headache populations will have to be performed in order to investigate these interesting trends further.
A possible association between TMD and TTH and combination headaches has been described in a few studies (38, 60), but attention has mainly been drawn towards the association between TMD and TTH (61–64). A Finnish study has investigated the association between different types of headache and TMD in children. No association was found (65). Many studies have found a correlation between severity and frequency of headache and TMD (39, 40, 42, 66). This may match our results, as patients with combination headaches may experience more severe symptoms and could be more affected (67). The general association between TMD and unspecified headache has been relatively well investigated. A recent study from Italy based on interviews has revealed a significant relationship between headache and symptoms of TMD in a general adult population (11). In many studies it has been shown that headache is a typical symptom among patients who suffer from TMD (11, 30, 31, 40–42). Likewise, several studies have indicated TMD as a frequent diagnosis among headache patients (34–36, 38–40, 42, 66, 68).
Chronic pain grade classification and depression (axis II)
Of the patients in our study, 82.8% reported facial pain according to the RDC/TMD axis II chronic pain grade classification, illustrating that 26.7% of headache patients experienced orofacial pain within the last month without obtaining a clinical TMD diagnosis. A reason for this could be a fluctuation of TMD symptoms (69, 70) and absence of pain during the examination. Another reason could be possible interference associated with the headache (e.g. temporal headaches). Of patients in the present population, 40.4% scored high disability on the chronic pain grade classification (grades III and IV), with an almost equal distribution between moderately and severe limiting. In a study from 2002 with a population of TMD patients, only 4.7% had a high disability chronic pain grade classification (71). This indicates marked differences between headache and TMD populations, with patients being more affected by TMD pain in the headache population than in a pure TMD population.
The SCL-90 depression scale developed by Derogatis (72) was later implemented to the RDC/TMD by Dworkin et al. (17). The usefulness of the SCL-90 scale in the RDC/TMD questionnaire has recently been validated (73), also in Danish patients (74). Axis II assessment of psychological status showed that 54.5% of patients in the headache population experienced moderate to severe depression. In a recent study the prevalence of major depression in the Danish population was 3.3% (75). This indicates that co-morbidity of depression might be an important factor in clinical headache populations. Co-morbidity of headache and psychiatric disorders (especially anxiety and mood disorders) is a well-recognized clinical phenomenon (14, 76–79). Our study has shown that a significantly higher proportion of headache patients with TMD than without TMD had moderate to severe depression, especially in those with combination headaches with TMD than in those without TMD.
Several studies have shown that many TMD patients are depressed. Yap et al. found that 39% of patients experienced moderate to severe depression (26, 71). Other studies have demonstrated overrepresentation of psychological symptoms in several pain conditions (29), particularly in patients with chronic daily headache and facial pain disorder (80).
Our results indicate that the co-morbidity of TMD in headache patients could be a risk factor for depression, or vice versa. This is specifically the case when dealing with combination headache patients. This corresponds to earlier studies, showing that the reported number of non-specific pain conditions may be a predictor of psychosocial dysfunction, depression and somatization (81), and that the number of pain conditions is a better predictor of major depression than the severity of the pain (82).
Conversely, those with moderate to severe depressive symptoms are also more likely to develop headache pain (83). The cause–effect relationship is unclear.
Pitfalls and strengths of this study
The patient population at the DHC is a highly selected group of the total headache population in Denmark, and as such not representative of the background population. Furthermore, the study sample is relatively small but fairly representative of the headache diagnosis in the Centre (84). This study has no control group, and in future studies we recommend an age- and gender-adjusted control group.
The RDC/TMD questionnaire is primarily designed to investigate TMD in groups of patients with orofacial problems, but has also been used to a large extent to assess the prevalence of TMD in general populations. When used on this specific group of patients it raised some problems. The RDC/TMD questionnaire used the word ‘facial pain’ for TMD pain, and some of the headache patients found it difficult to distinguish between facial pain and headache. In this study, the patients were told that facial pain signifies pain in the face, jaw, temple, in front of or in the ear.
Both RDC/TMD and IHCD-II are internationally accepted criteria (17, 27), and the results from our study are subsequently comparable to those of earlier studies. The reliability of RDC/TMD axis I diagnoses when using a trained and calibrated examiner has been demonstrated in a recent study (23).
The setting allowed cooperation between the neurologist and the investigator, but with a strict blinding, because the exact diagnosis was made only after all patients had been examined. It is an advantage that the present study is interdisciplinary, because symptoms and treatment of patients with complicated headache disorders most often cover several clinical areas.
Conclusion
Our findings of a high prevalence of TMD (particularly myofascial pain) in the headache population, compared with earlier findings from the general population, lends some support to the view that examination of the masticatory system should be included in the medical diagnosis of all headache sufferers. Our studies indicate that a high proportion of headache patients have significant disability because of ongoing chronic TMD pain.
The high prevalence of TMD in patients with combined migraine and TTH compared with other headache groups suggests that the combination headache may be a risk factor for development of TMD, or that TMD could be a risk factor for development of several coexistent types of headache.
A need for screening procedures and treatment strategies concerning depression in headache patients with coexistent TMD is underlined by the overrepresentation of depression in this group. More interdisciplinary research is necessary in this area.
Finally, the possible co-morbidity between combination headaches, TMD and depression that this study reveals calls for an integrated and multidimensional approach concerning physical and psychosocial factors when treating patients with complicated headache disorders. In the long term, identification of common features or associations between TMD and headache may have a major impact on future treatment strategies and clarify the importance of an interdisciplinary effort between different specialities, e.g. dentists, psychologists and neurologists. Larger-scale studies and interdisciplinary research are essential for further advances in this area.