
Abstract
This population-based cross-sectional study examined the 3-month prevalence of headache, migraine and tension-type headache (TTH) among adolescents aged 12-15 years in Germany Students (n = 3324) from 20 schools completed a questionnaire on general and headache-specific pain which included a sociodemographic module. The headache-specific questionnaire complied with the respective revised criteria of the International Headache Society (IHS). 'Modified criteria' changed the item 'duration' in migraine (>30 min instead of >4 h). The overall 3-month prevalence of headache was 69.4% (boys 59.5%, girls 78.9%), with 4.4% of the adolescents suffering from frequent (≥ 14 days/3 months) and severe (grade 8-10 on a 10-point visual analogue scale) headache and 1.4% (boys 0.9%, girls 1.9%) from headache ≥15 days/month. The 3-month prevalence of migraine was 2.6% (boys 1.6%, girls 3.5%) applying strict IHS criteria and 6.9% (boys 4.4%, girls 9.3%) with modified criteria; 12.6% (boys 8.3%, girls 16.7%) suffered from probable migraine, 0.07% fulfilled the criteria for chronic migraine, 4.5% (boys 4.6%, girls 4.3%) suffered from TTH, 0.2% from chronic TTH and 15.7% (boys 14.5%, girls 16.9%) from probable TTH. Headache and migraine were more common in girls than in boys and in teenagers, especially in girls, aiming at higher education. Recurrent headache and primary headache disorders are common complaints among German adolescents, especially among girls.
Introduction
Headache is a common problem among teenagers (1–3). It also constitutes a health problem, since recurrent headache is a risk factor for future chronic headache and other pain syndromes (4). Headache and its subtypes restrict teenage quality of life (5) and is a major cause of absence from school as well as an important factor in health-related costs among adolescents (6). The number of population-based studies assessing the prevalence of headache and its subtypes among teenagers is limited (7, 8). Some studies have reported a higher headache prevalence in teenage girls than boys (7–9). However, published prevalences for primary headache disorders vary considerably, within a prevalence range of 1.0–17.0% for migraine and 0.9–72.3% for episodic tension-type headache (TTH) (8). The use of different International Headache Society (IHS) criteria (strict vs. modified) for the classification of headache is discussed as a possible cause for these large prevalence differences. Also, variations in the specific wording for questionnaire items assessing the IHS criteria in different studies might have contribute to the observed variability of estimates (10).
In Germany, only two studies have assessed headache prevalence among adolescents. Overall headache prevalences of 90.0% and 75.4%, respectively, among teenagers have been reported (11, 12). One of the studies classified 11% of 8–16-year-old participants as migraine cases and 48.7% as TTH cases. Both studies were conducted in the western part of Germany. For the eastern part, data on the prevalence of primary headache disorders according to the IHS criteria are not available.
The aim of this study was the population-based assessment of the prevalence of headache, recurrent headache and primary headache disorders such as migraine and TTH in adolescents 12–15 years of age, the generation born directly after German reunification, in eastern Germany.
Methods
Study population
In the region of West Pomerania in north-eastern Germany on the Baltic Sea, 50% of all schools were randomly selected in a sampling stratified by school type. The latter included extended elementary schools, junior high schools, high schools and private schools. Schools for mentally or physically disabled children were excluded. All 20 sampled schools participated in the study. All students attending the 7th, 8th or 9th grade during school year 2003/2004 were invited to participate. In Germany, attending school for at least 9 years is compulsory for all children, thus nearly all teenagers in the respective age groups were eligible for the study. From a total of 3699 eligible students, 3324 participated and filled in a questionnaire, yielding a response rate of 89.9%. Reasons for non-participation were absence from school due to illness (6.0%), absence without excuse (1.7%), lack of parental consent (1.6%) and other reasons (0.8%). The vast majority of students (93.5%) were 12–15 years old, corresponding to the normal age range of teenagers in 7–9th grade in Germany. Because of low numbers in the respective strata, students in age groups 16–18 years were excluded (N = 212). In addition, 40 questionnaires were excluded from analysis because <50% of questions were answered. Thus, a total of 3072 questionnaires were used for this analysis.
Data collection
All sampled schools were informed about the study by an invitation letter, a telephone call and a personal visit of each school's director. Subsequently, a letter with detailed information about the study was sent by the school to parents of all students in the respective three grades. The letter explained that participation was voluntary and that parents could refuse participation of their child. The students filled in a self-completion questionnaire during one regular school lesson. The questionnaire took between 30 and 40 min to complete. In each classroom three trained study workers gave a short standardized instruction on how to fill in the questionnaire and answered procedural questions during the process of filling in the forms. All questionnaires were anonymized. Prior approval of this study was obtained from the Ministry of Education, Sciences and Culture Mecklenburg-West Pomerania and from the Ethics Committee of the Mecklenburg-West Pomerania Board of Physicians at the University of Greifswald.
Questionnaire
The questionnaire, designed especially for this study, included pain- and headache-related items and questions about various sociodemographic factors. The pain and sociodemographic questions are compatible with those used in the German Health Survey for Children and Adolescents (13). The questions in the headache module of the questionnaire were based on the German translation of the 2nd edition of the IHS classification (14, 15). Headache prevalences were assessed for 3 months and 7-day periods prior to data assessment. In case of positive answer to the question ‘Did you have headache within the last 3 months?’ with the answering categories ‘no’, ‘yes, once’, and ‘yes, more than once’, further information about frequency, duration, characteristics, symptoms, intensity of headache and medication relevant to the classification of headache according to the IHS criteria were solicited. The frequency of headache was assessed based on the number of headache-days per time period. Headache severity was measured on a visual analogue scale (graded 1, very low severity, to 10, very high severity). Classification of participants into the recurrent headache category was based on the answer in the screening question (‘yes, more than once’), whereas the classification of teenagers into the category recurrent frequent headache was determined by the number of headache days within the last 3-month period (≥14 days with headache/3 months).
Primary headache disorders (migraine, chronic migraine, probable migraine, probable chronic migraine, TTH and probable TTH, including the subtypes of TTH) were classified according to the IHS criteria for adults (14, 15). According to the IHS criteria, the classification of headache into probable migraine or probable TTH was used if the headache was fulfilling all but one criterion for a full diagnosis of respective primary headache disorder. For migraine, additionally modified criteria for children were used as suggested in the IHS classification with a shorter duration of headache (attacks between 30 min and 72 h instead of attacks between 4 h and 72 h). During a pilot study the questionnaire and all procedures were tested in one junior high school with 71 students. No indication of problems with particular questionnaire items, answer categories or study logistics was found.
Statistical analysis
Period prevalences for headache, recurrent headache and the IHS entities migraine, chronic migraine, probable migraine, probable chronic migraine, TTH (infrequent, frequent and chronic) and probable TTH (infrequent, frequent and chronic) were estimated based on the symptom frequencies provided in the questionnaire. Differences in prevalence between age groups, gender and school type were tested by non-parametric test for trend (Cuziak), χ2 test (nominal data) or by Mann–Whitney U- or Kruskal–Wallis tests (ordinal data), respectively. To classify the education level and the type of school attended by the adolescents the planed school exam (‘education track’) was used. Ninety-five percent confidence intervals (CIs) for the prevalence of migraine and TTH were calculated based on the definition of CIs according to Hays and Winkler (p. 104 in (16)) and were corrected for the respective sampling proportions. For the calculation of age-adjusted prevalences for recurrent headache for boys and girls in different education tracks, the 12–15-year-old population of the region West-Pomerania in 1-year age groups was used as the standard. Ninety-five percent CIs for standardized prevalences were calculated based on the definition of the standard error according to Cochran (17). Data analysis was performed with SAS, version 9.1 (SAS Institute Inc., Cary, NC, USA).
Results
Table 1 provides characteristics of participating schools and students. The 3-month prevalence of headache was 69.4% and differed significantly (P < 0.001) between girls and boys (Table 2). Of all students, 31.8% reported only one headache occurrence during the preceding 3-month period and a further 37.6% reported recurrent headache. The 7-day prevalence of headache was 31.6%, again with a significant gender difference (boys 21.7%, girls 41.0%; P < 0.001). Recurrent frequent headache defined as occurrence at at least 14 days within the preceding 3-month period was reported by 16.6% of the girls and 7.0% of the boys (P < 0.001) (Table 2). Only in girls there was a significant increasing trend of prevalence for overall headache (P = 0.001), recurrent headache (P = 0.001) and headache at at least 14 days/3 months (P = 0.011) with higher age (Table 2). Among those with headache, teenage girls reported significantly more days with headache in the preceding 3 months (mean 10.1 days,
Study population

Number of participating students and proportion of response by school type.
Ethnic background was defined by country of birth (Germany vs. all other countries combined).
Three-month prevalence of self-reported headache, recurrent headache and recurrent frequent headache among 3072 students 12–15 years of age in the region of West Pomerania, Germany

Recurrent headache, defined as more than one episode in the preceding 3 months (N = 1156), was more common in teenagers at higher educational levels (Table 3). 37.9% (age-adjusted rate) of the girls attending extended elementary schools but 52.3% of those at high schools reported recurrent headache. In boys, this difference was smaller and not statistically significant (age-standardized rates 23.0% vs. 27.5%, P = NS).
Prevalence of self-reported recurrent headache by type of school examination
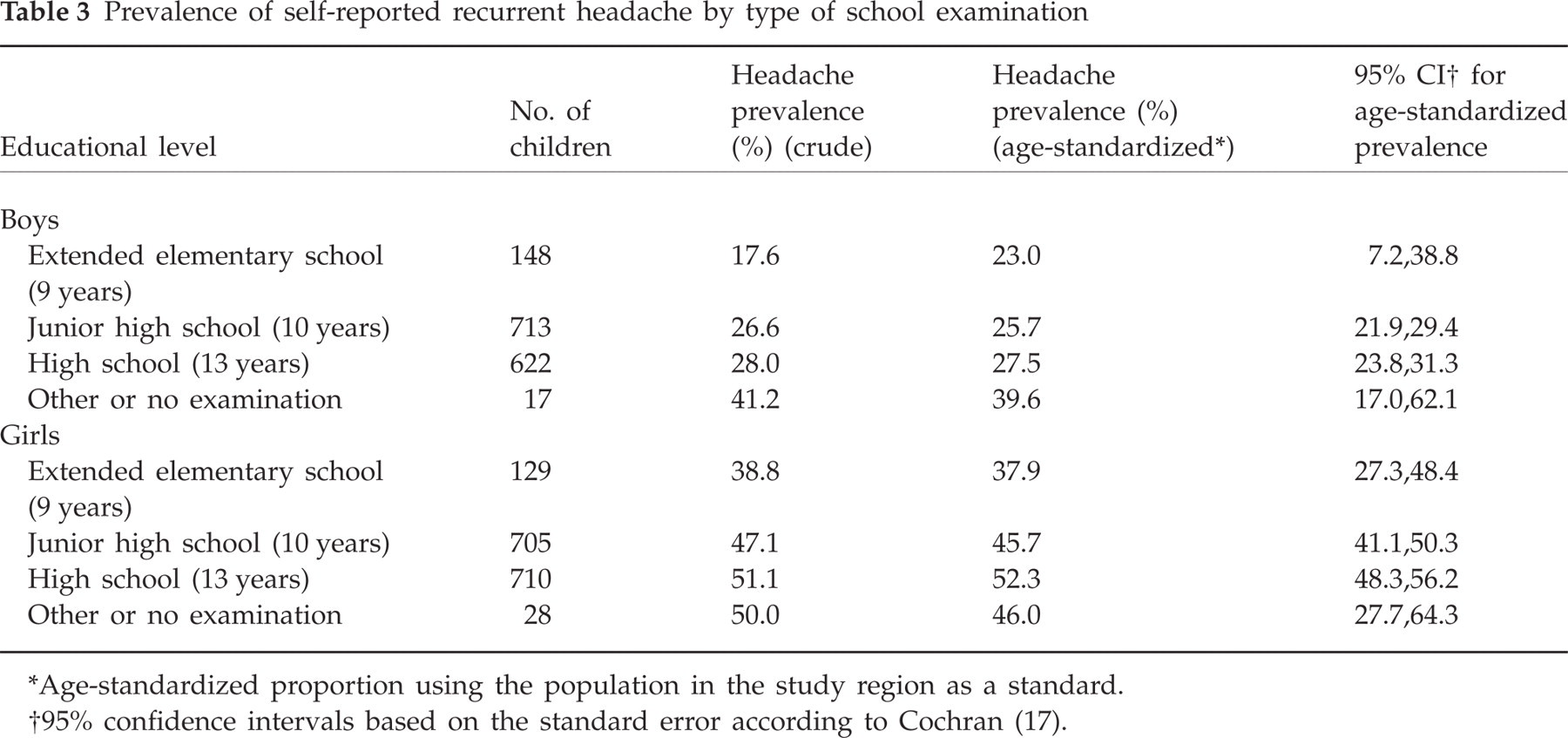
Age-standardized proportion using the population in the study region as a standard.
95% confidence intervals based on the standard error according to Cochran (17).
Applying strictly the criteria of the IHS classification (14, 15), the overall prevalence of migraine (Fig. 1) was 2.6% (boys 1.6%, girls 3.5%; P < 0.001). Two teenagers (0.07%) fulfilled the criteria for chronic migraine. Both took medication against headache, but less than 10 times within the 3-month period. Of the adolescents, 12.6% could be classified as suffering from probable migraine (boys 8.3%, girls 16.7%; P < 0.001). Six teenagers (0.2%) suffered from probable chronic migraine with a medication intake of >10 times within the whole 3-month period. Modifying one criterion (headache duration >30 min instead of ≥4 h) similar to the IHS classification criterion for children, the prevalence of migraine increased to 6.9% (4.4% in boys, 9.3% in girls; P < 0.001). Except for 12-year-old students, higher prevalences were found for girls in all age groups (Fig. 1).

Prevalence of migraine in boys and girls according to strict International Headache Society criteria for adults and to modified criteria (headache duration >30 min instead of ≥4 h). Error bars indicating 95% confidence interval, corrected for the respective sampling proportions.
TTH defined according to strict IHS criteria was reported by 4.5% of all teenagers (boys 4.6%, girls 4.3%; P = NS). Table 4 provides a summary of the prevalence of TTH, probable TTH and its subtypes. The criteria for both probable migraine and probable TTH were met by 2.6% of the adolescents and for TTH and probable migraine by 1.0%.
Three-month prevalence of tension-type and probable tension-type headache (TTH) for girls and boys aged 12–15 years in the region of West-Pomerania, Germany

Difference between prevalences in boys and girls significant with P < 0.01.
In N = 3 and N = 17 teenagers in the groups of TTH and probable TTH a classification into the TTH subtypes was not possible.
Discussion
In this population-based study, headache was a common problem in adolescents aged 12–15 years. More than two-thirds of participants reported headache during the last 3 months, 1/10 of them with a frequency of at least one episode per week. Slightly more than 4% of the children experienced severe and frequent headache. Girls reported headache and migraine significantly more often than boys. In girls there was an increase in headache prevalence with higher age. Hormonal changes during puberty have been proposed as one possible reason for this association (18), especially for increased prevalences of migraine. It is unlikely, however, that hormonal changes account for all of the observed increase in TTH and overall headache in a similar fashion (18).
The 3-month prevalence of recurrent headache, defined as more than one episode per month, migraine and probable migraine increased with higher educational level, especially in girls. Since age was adjusted for, it cannot be explained by slight differences in age distributions between students attending different types of school, nor by ethnic background, since this proportion was similar between all school types (Table 1). In Mecklenburg-West Pomerania there are three different school education levels (graduation after 9 years, after 10 years and after 12 or 13 years). The observed differences in headache prevalence may be due to increasing work demands (more lessons and homework) and pressure for better performance at higher educational levels. It has also to be considered that the type of school attended is positively correlated with social class in Germany (19, 20). The connection between headache and social class, however, is controversial. Whereas the German National Health Survey (GNHS) also reported higher headache prevalences in adults in higher social classes (21), two Scandinavian studies observed an increase in headache prevalence with decreasing social class (22, 23). Three other studies from Germany, Iceland and Greece have reported no association (11, 24, 25). Further investigation is necessary to clarify systematic differences in headache prevalence in different social classes and types of school.
Headache prevalences in the present study were consistent with the findings of the German study of pain in children (3-month prevalence 75.4%) and a Norwegian headache study (12-month prevalence 76.8%) (8, 12). Frankenberg et al. reported higher prevalence rates of overall headache (90.0–93.0%) in German teenagers. In their study, however, lifetime prevalences rather than a 3-month period were assessed (11). Compared with young adults (18–29 years old) in the GNHS, both 3-month (men 71.7%, women 83.1%) and 7-day prevalences (men 27.5%, women 48.5%) were only slightly higher than in the adolescents in our study (21). For recurrent headache the prevalences vary widely between 13.9% and 51.4% in the literature. This considerable range, however, is largely due to varying definitions and differing age groups (7, 8, 11, 22, 26–29). Recurrent headache, defined as more than one episode in the last 3-month period, however, was similar in our study (37.6%) to findings in Swedish teenagers (44.8%) (29).
The range of reported prevalences for migraine and TTH also varies widely (0.6–17% for migraine and 0.9–72.3% for TTH) in different studies (4, 8, 29–31). The main reason for this inconsistency is again that the studies used various criteria for the classification of primary headache disorders. Migraine prevalence in our study was similar to other studies that used the IHS criteria for classification, whereas results for TTH were relatively low in comparison with other studies from Western countries. However, we found relatively high prevalences of probable migraine or probable TTH in adolescents, which fulfilled all but one classification criterion. Thus, based on the answers of the standardized questionnaire items, 40.8% of the adolescent headache patients were classified as having a probable primary headache disorder, whereas only 10.1% of headache sufferers could be definitively classified as persons with either migraine or TTH. The remaining 49.1% of the students were not classifiable. One reason for this might be that these teenagers were not suffering from any specific primary headache disorder. It is more likely, however, this small proportion reflects lack of sensitivity of the respective arrays in the IHS classification in the context of an epidemiological study. This is supported by the relatively large number of teenagers with probable migraine or probable TTH. The issue of validity of the IHS criteria for the classification of headache in children and adolescents has been discussed. Maytal reported only 53% agreement of the diagnoses according to the IHS criteria compared with clinical diagnoses of migraine yielding a sensitivity of 27.3% (32). In our study, 5.1% of the adolescents described vomiting during headache. Using this symptom as a specific indicator for migraine, the 2.6% prevalence of migraine according to strict IHS criteria would appear too restrictive.
Similar to a study by Laurell (29), in our study the items headache duration for a positive diagnosis of migraine and headache frequency for TTH were identified as the most restrictive factors. In migraine, 79 adolescents had headache duration between 4 and 72 h, whereas 133 teenagers reported durations between 30 min and 4 h. Applying the modified criterion for children as suggested by the IHS classification, the prevalence of migraine increased to 6.9%. Headache duration other than between 4 h to 72 h was also the most frequent reason for being classified as probable migraine. Of all participants, 9.3% fulfilled all but the duration criterion for migraine. Other reasons for classification into probable migraine were less than five attacks (1.0% of all teenagers), 2.0% had neither phono/photophobia nor nausea nor vomiting, and only 0.2% had only one and not two of the four characteristics of migraine (unilateral location, pulsating quality, moderate or severe pain intensity, aggravation by or causing avoidance of routine physical activity). The figures are similar for TTH: of 483 teenagers classified as probable TTH sufferers according to IHS criteria (fulfilling all but one criterion for the full TTH diagnosis), 272 did not fulfil criterion A, because they had <10 lifetime episodes of TTH (N = 162) or used the answer ‘I don't know the number of previous attacks' (N = 110). Another 3.7% of all participants met all but the duration criterion, 2.4% reported either phono- and photophobia or nausea during headache without having migraine, and 0.8% had only one, not two of the four TTH characteristics (bilateral location, pressing/tightening quality, mild or moderate intensity, not aggravated by routine physical activity). Thus, further research should evaluate the required minimum number of attacks needed for a classification as TTH.
One of the strengths of this study is that it included a large, representative, population-based sample of adolescents at all types of school and had a very high response rate (89.9%). Six per cent of the students were absent because of illness on the study day. If in some of these the cause of absenteeism was headache, this might have resulted in a slight underestimation of the true prevalence. However, later examination of the absent students was impossible since data collection had to be completely anonymous.
One weakness of the study is that it was based on a self-completion questionnaire. However, the pain questionnaire used was an established instrument to assess frequency and localization of pain among children and adolescents and has been extensively used before (3, 33). We used the validated German version (12, 33), the suitability of which for the targeted age group of 12–15-year-olds has explicitly been shown before (34). We added specific questions for further subtype classification of headache into migraine and TTH that addressed the German translation of the most recent IHS criteria (14) for those two types of headache. The IHS criteria do not differ between adults and adolescents with the exception of the minimal attack length. This ensures that the validity of the diagnoses of primary headache disorders is as high as a direct implementation of the IHS classification allows. Additionally, this method ensures high comparability of our data to those of other studies.
We performed a pilot study that showed that students in the targeted region and age range were capable of understanding and completing the questionnaire. Additionally, trained study workers gave a formal and standardized introduction and answered all procedural questions during the completion of the questionnaires. Thus, a high item-specific response to most single questions was achieved. No information about expected results or specific information about headache was given before or during data collection, as such information may have influenced reporting (35).
In summary, the present study showed that a large number of German teenagers suffer from headache. Additionally, a high number of adolescents experience frequent and severe headache. Children with frequent headache may be at increased risk of developing chronic headache in adulthood (36). Our findings support the need for preventive efforts and research towards effective diagnostic and therapeutic management of headache in children and adolescents.
Note
Upon request, the authors will be glad to send the full questionnaire used in the study (in German).
Acknowledgements
The authors express their gratitude to participating students, the directors and all school staff members of the participating schools for their contribution to this study. This study is part of the ‘DMKG Headache Study’ and was supported by the German Migraine and Headache Society (DMKG) and unrestricted grants of equal share from Astra Zeneca, Berlin Chemie, Boots Healthcare, Glaxo-Smith-Kline, MSD Sharp & Dohme, Pfizer and Woelm Pharma. The analysis part was additionally supported by the German Federal Ministry of Education and Research (NBL3 program, reference 01ZZ0403).