
Abstract
The aim of this study was to estimate the 1-year prevalence of headache, migraine, tension-type headache (TTH) and chronic daily headache (CDH), and the degree of association of migraine with some sociodemographic characteristics of the population of Florianopolis, Brazil. This is a cross-sectional, door-to-door, population-based study. In 300 randomly selected households, 625 subjects, aged 15–64 years, responded to a structured questionnaire. The 1-year prevalence of headache was 80.8%, of migraine 22.1%, of TTH 22.9%, and of CDH 6.4%. Migraine and CDH were significantly more prevalent in females than in males. Migraine was significantly associated with the following variables: low household income, low electricity consumption, and divorced or widowed marital status. We have shown high prevalences of migraine and CDH in Florianopolis, close to the higher rates of previous studies. There was a preponderance of migraine in females, divorced or widowed, with a low socioeconomic level.
Introduction
Headache is a frequent symptom in internal medicine and neurology clinics (1, 2). The first epidemiological studies of headache were done with either patients of medical and neurological wards or in headache tertiary care units. These studies do not reflect population data, because they do not include a great number of patients with headache who never consulted a physician. Population-based studies actively seek these patients (3, 4).
The 1-year prevalence of headache, migraine and tension-type headache (TTH) has been estimated in many population-based studies, applying the 1988 International Headache Society (IHS) diagnostic criteria for headache and head pain (5). The 1-year prevalence of migraine has been estimated to be from 1 to 28%(6–31). Migraine prevalence seems to be higher in countries of Europe and North America than in those of Latin America, Africa and Asia. The 1-year prevalence of TTH ranges widely from 2 to 74% (6, 8–10, 17, 22–25, 27, 28, 32–34). The 1-year prevalence of chronic daily headache (CDH) has been estimated to be from 2.98 to 4.7%(35–38).
A possible association between migraine and some sociodemographic characteristics of the population has been described. Some studies in the USA have found a higher prevalence of migraineurs with a low income (4, 15, 16, 30). This was not found in other countries (10–12, 17–19, 39). Stang and Osterhaus (4), in the USA, reported a higher prevalence of migraine in highly educated subjects, but this association was not statistically significant in other studies (8–10, 16, 39). No statistically significant association was found between migraine and marital status (9, 16, 39).
In Brazil there have been no epidemiological population-based studies of headache in adults. Barea et al. (40) described the prevalence of headache in school children of Porto Alegre, Rio Grande do Sul. Rabello (41) and Bigal et al. (42) estimated the prevalence of migraine in hospital workers. In Florianopolis, Costa et al. (43) described the prevalence of headache in medical students.
The objectives of this study were to estimate the 1-year prevalence of headache, migraine, TTH and CDH, and to estimate the degree of association of migraine with some sociodemographic characteristics of the population.
Methods
This is a cross-sectional, door-to-door, population-based study. We randomly selected 300 households in the central area of Florianopolis, Santa Catarina, Brazil, including downtown and 23 suburbs, which comprise 58.5% of the entire population. According to the 1996 Brazilian Census, Florianopolis had 271 281 inhabitants (185 466 from 15 to 64 years of age). The sample size was calculated with the software Epi Info 6.04b, for an expected migraine prevalence of 5 ± 2%, and a 95% confidence interval. We have chosen the 5% expected rate because this was close to the estimated 1-year prevalence of migraine in previous Latin American studies (19, 20). The calculated number of required participants was 454. We added 20% to correct the design effect (cluster sampling), and an additional 20% expecting some dropouts, totalling 654 subjects to be interviewed. Because the mean number of subjects from 15 to 64 years old in each household is 2.36, according to the same census, the calculated number of households to be visited was 300.
The 300 households were stratified into three groups, based on electricity consumption, in kilowatt-hours (kWh) per household per month: low consumption ≤150 kWh, medium consumption 151–350 kWh, high consumption >350 kWh, expecting to select subjects of different socioeconomic levels. In underdeveloped countries, it is believed that this is a good way of measuring peoples’ socioeconomic status (44). The number of households selected in each group was proportional to the total number of households of that group: low consumption, 91 households; medium consumption, 143 households; and high consumption, 66 households.
In each household, every subject from 15 to 64 years old responded to a structured questionnaire. The questionnaire had not been previously validated, but it was tested in 100 headache patients of the Neurology Clinics of the University Hospital of the Universidade Federal de Santa Catarina (UFSC). It included seven questions about the sociodemographic characteristics of the population as well as 20 questions about the headache, based on the 1988 IHS diagnostic criteria for headache and head pain (5). In order to minimize recall bias, the complete interview was done only with subjects who reported headaches within the last year. Trained medical students conducted the direct interviews. The students received lessons about the diagnostic criteria of migraine and tension-type headache, and instructions on how to interview subjects without inducing the answers. Before going into the field, they interviewed headache patients of the Neurology Clinics of the University Hospital of the UFSC, under the supervision of the senior author (L.P.Q.). The data were collected from March to July 2000. The senior author (L.P.Q.) randomly re-interviewed 6% of the sample, with a good concordance rate (
Headache diagnoses were based in the 1988 IHS diagnostic criteria for headache and head pain (5). At that time the 2004 IHS classification was not available. Migraine and TTH were diagnosed when all criteria were fulfilled. The diagnosis of ‘migrainous disorder’ and ‘tensional disorder’ was given when all criteria were fulfilled but one. Subjects were told to answer the questions based on their most frequent type of headache, if they had more than one type. Therefore, we gave only one diagnosis for each subject with headache within the last year.
CDH, in this study, was diagnosed when the frequency of head pain was ≥180 days per year, based on a question about the frequency of the headache. Scher et al. (37) used this same criterion. We gave the diagnosis of ‘chronic migraine’ to subjects who also fulfilled the criteria for migraine or ‘migrainous disorder’, and the diagnosis of ‘chronic tension-type headache’ to those who also fulfilled the criteria for TTH or ‘tensional disorder’. Many subjects classified as ‘chronic migrainous disorder’ reported headaches of <4 h, but fulfilled all other criteria for migraine.
For the study of the association of migraine with some sociodemographic characteristics of the population, we grouped subjects with migraine and ‘migrainous disorder’. To analyse the relationship between electricity consumption and migraine, we calculated the electricity consumption in kWh per capita per month.
Prevalence rates were calculated, with 95% confidence interval (95% CI). The prevalence ratio (PR), with 95% CI, was used to study the magnitude of possible associations between headache types and some sociodemographic variables. χ2 test was used to analyse nominal variables, such as gender and marital status; and the linear trend χ2 test (LT χ2) to analyse ordinal variables, such as energy consumption and household income. Statistical significance was defined as P < 0.05.
The Ethics Committee of the UFSC approved this study.
Results
From 719 eligible individuals, 625 responded to the questionnaire. The participation rate was 87%. The sociodemographic characteristics of the respondents are shown in Table 1. Non-responders did not differ from responders in any sociodemographic variable except gender. We did not interview more males (64.9%) than females (35.1%).
Distribution of the respondents, by sociodemographic characteristics (n = 625)

kWh, kilowatt-hours; BMW, Brazilian Minimum Wage.
Headache within the last year was reported by 505 subjects. The 1-year prevalence of headache was 80.8% (95% CI 77.5, 83.8). Headaches were significantly more prevalent in females (88.7%) than in males (71.5%) (χ2 = 29.60; P < 0.001).
The 1-year prevalence of some types of headache is shown in Table 2. The prevalence of migraine and TTH was about the same, including only subjects who fulfilled all IHS criteria for these diagnoses. If we grouped together subjects with migraine and ‘migrainous disorder’, the prevalence would be 40.3%, and for subjects with TTH and ‘tensional disorder’, 33.0%. Figure 1 shows the 1-year prevalence of migraine and TTH by gender. Migraine was significantly more prevalent in females than in males (χ2 = 19.10; P < 0.001), with a 2 : 1 female/male ratio. This difference was not significant for TTH. Figure 2 shows that the 1-year prevalence of all headaches peaked at the ages of 25–34 years; migraine was more prevalent at the ages of 35–44 years; and the prevalence of TTH was highest from 15 to 24 years of age.
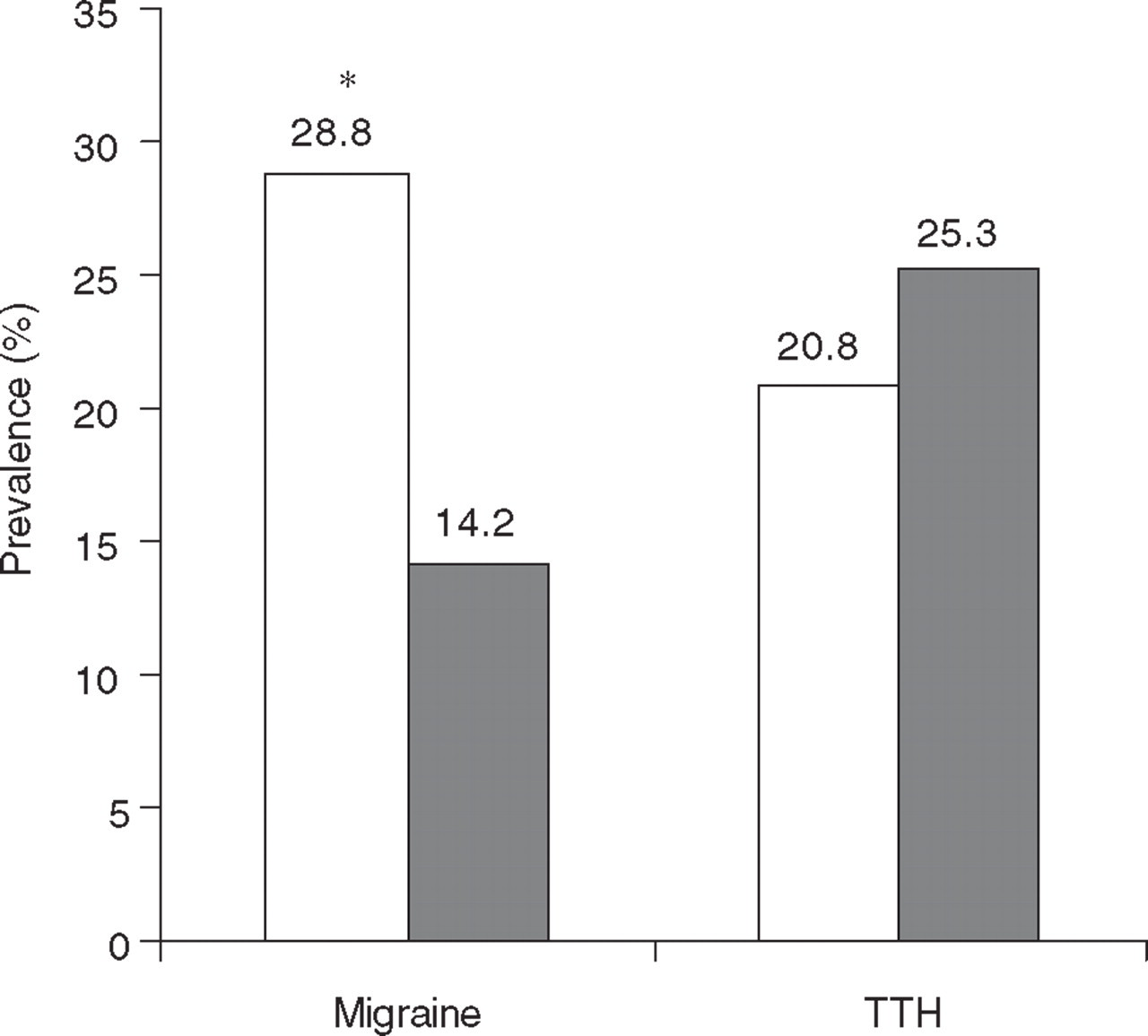
Estimated 1-year prevalence of migraine and tension-type headache (TTH), by gender. □, Female; ▪, male. ∗P < 0.001.

Estimated 1-year prevalence of headache (□), migraine (▵) and tension-type headache (▪), by age.
Estimated 1-year prevalence of some types of headache

The 1-year prevalence of CDH was 6.4% (95% CI 4.7, 8.7). The prevalence was 10.1% in females and 2.1% in males, with a 5 : 1 female/male ratio. This difference was statistically significant (χ2 = 16.59; P < 0.001). From the 40 subjects (34 females and five males) with CDH, 32 (80%) had the diagnosis of ‘chronic migraine’ and eight (20%) of ‘chronic tension-type headache’.
Table 3 shows that there is an inverse significant linear trend between electricity consumption and migraine prevalence: the lower the electricity consumption, the higher the prevalence of migraine. Subjects who had a consumption per month of <48.33 kWh reported 1.54 times more migrainous headache than subjects who had a consumption of >105.5 kWh. This inverse relationship was also observed between household income and migraine prevalence (Table 4). Subjects with a family income of less than 5.1 Brazilian Minimum Wages (BMW) per month had 1.54 times more migrainous headache than subjects with a family income of more than 20 BMW.
Distribution of the 1-year prevalence of migraine and ‘migrainous disorder’, with prevalence ratio (PR) and 95% confidence interval (CI), according to the electricity consumption per capita per month, in kWh (quartiles)
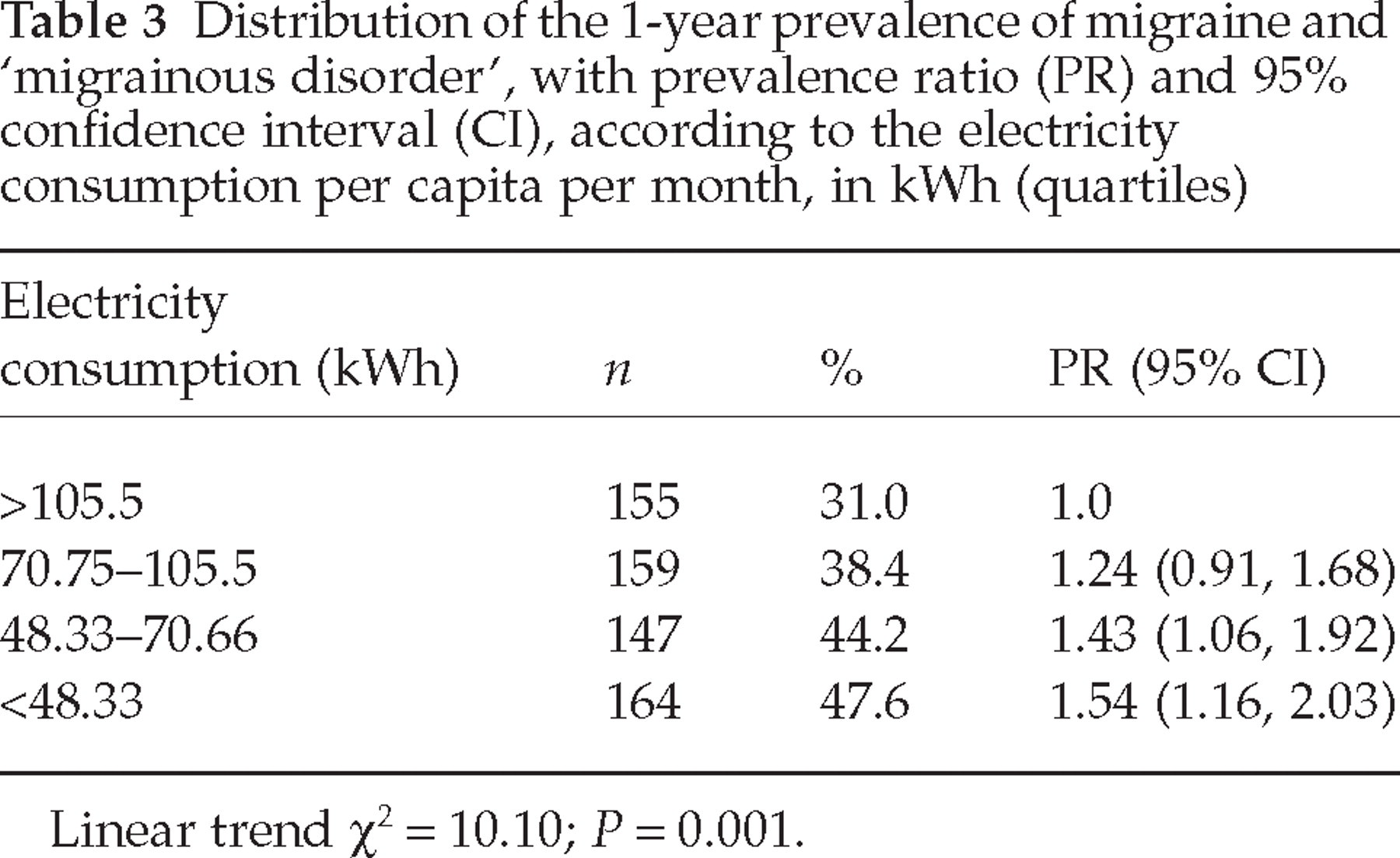
Linear trend χ2 = 10.10; P = 0.001.
Distribution of the 1-year prevalence of migraine and ‘migrainous disorder’, with prevalence ratio (PR) and 95% confidence interval (CI), according to the household income, in Brazilian Minimum Wages (BMW)
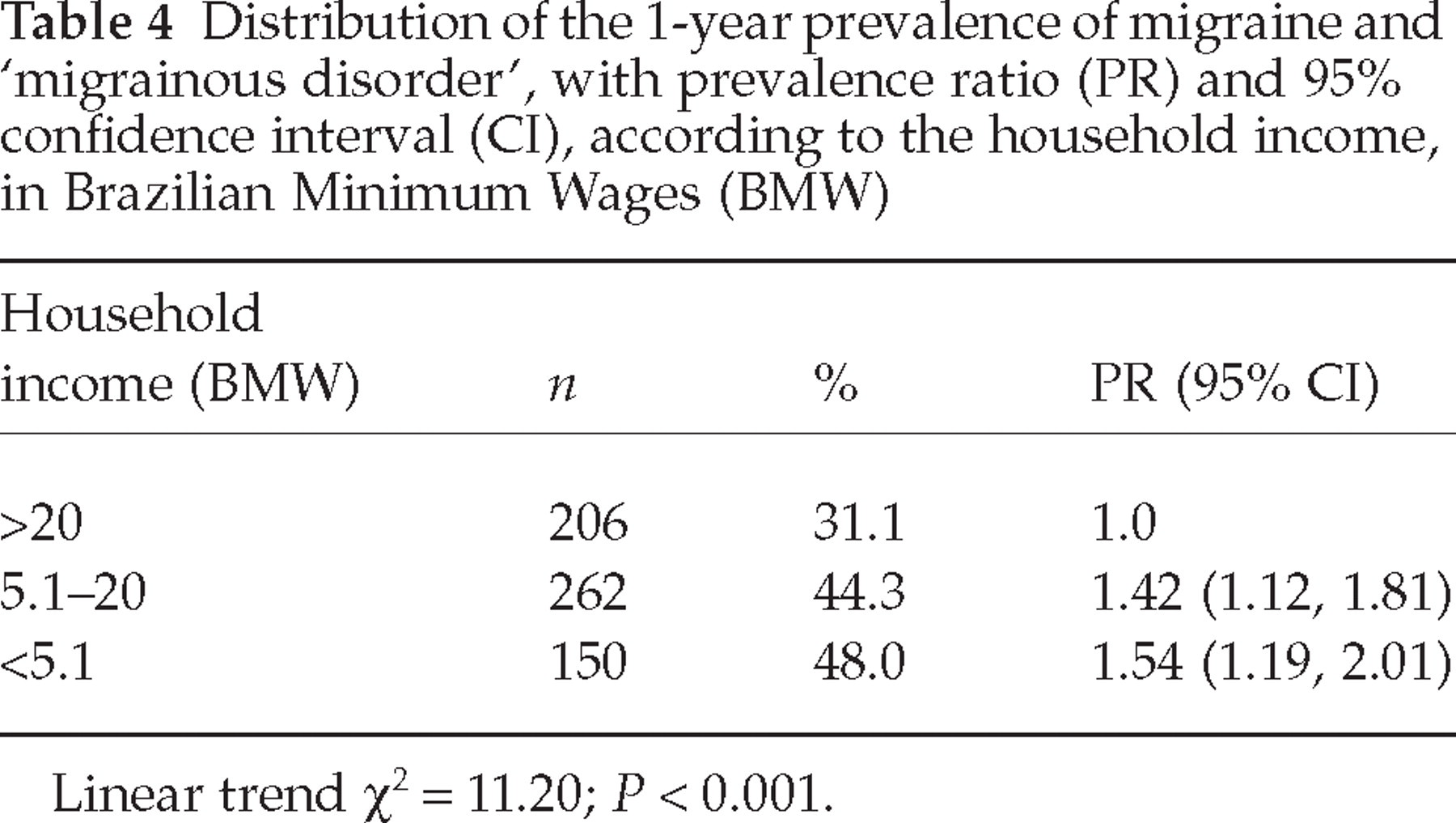
Linear trend χ2 = 11.20; P < 0.001.
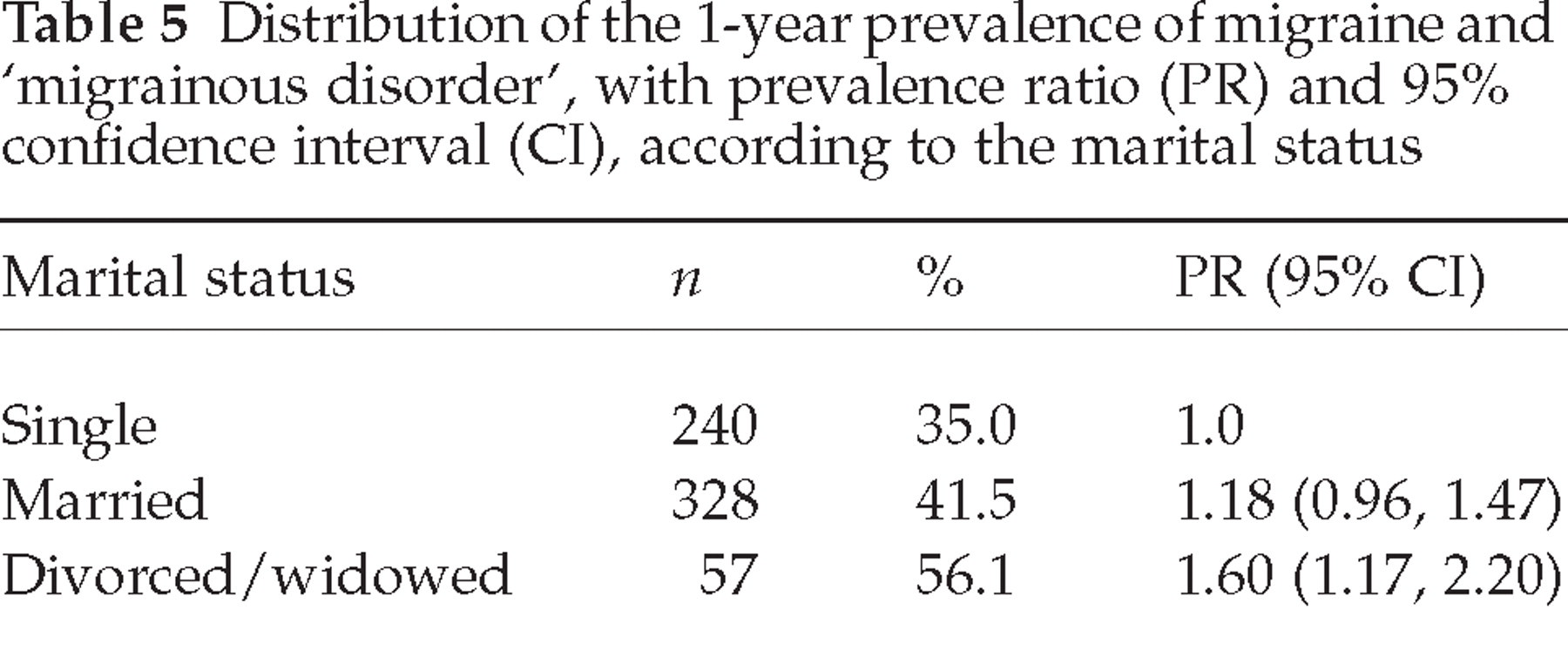
There was no statistically significant relationship between migraine prevalence and educational level. Table 5 shows that divorced or widowed subjects reported 1.6 times more migrainous headache than single persons.
Distribution of the 1-year prevalence of migraine and ‘migrainous disorder’, with prevalence ratio (PR) and 95% confidence interval (CI), according to the marital status
Discussion
This is the first population-based study of headache in Brazilian adults, applying the operational diagnostic criteria of the IHS. We had a high participation rate (87%) and a good random selection of the sample, at different socioeconomic levels.
Carefully trained medical students obtained the data through direct, door-to door interviews. This type of interview is considered an excellent research tool for epidemiological studies (45). To minimize recall bias, we completed the headache questionnaires only with subjects who had experienced head pain within the last year. Although the coexistence of migraine and TTH is frequently reported in the literature (6, 10, 17, 25, 27, 28), in this study we gave only one diagnosis for each subject, based on their most frequent type of headache. This might overestimate the prevalence of migraine and underestimate the prevalence of TTH, because people tend to remember their more severe headaches, which are usually migraines. There was a higher proportion of males in the non-responders. As males have a lower prevalence of headache, we may have overestimated a little the reported prevalence rates.
The 1-year prevalence of headache was 80.8%. This was similar to the 85.7% reported by Pereira Monteiro (10), in Oporto, Portugal.
The estimated 1-year prevalence of migraine is usually higher in European and North American studies than in Latin American, African and Asian studies. Pryse-Phillips et al. (17), in Canada, reported a migraine prevalence of 28%, but 14% had only migraine and an additional 14% had migraine and TTH. Merikangas et al. (9), analysing a cohort from Zurich, Switzerland, estimated a prevalence of migraine of 24.5%, but it was probably overestimated, because the population sample was 29 and 30 years old, in whom the migraine prevalence is usually higher. However, even in Asia, in South Korea, Roh et al. (27) described a migraine prevalence of 21.4%. We found a migraine prevalence of 22.1%, which is close to the higher estimated prevalence rates reported in the literature. This may be partly explained by the fact that the genetic background of the population of Florianopolis is European. The prevalence of migraine was higher in the age group 35–44 years. This was found also in some other studies, such as by Launer et al. (11) in the Netherlands, by O'Brien et al. (18) in Canada, by Alders et al. (24) in Malaysia, and by Wong et al. (22) in Hong Kong.
There is a wide range in the estimated 1-year prevalence of TTH, from 2 to 74%. This may reflect methodological differences between studies; also, this disorder may be influenced by sociodemographic and psychological aspects of different populations. In this study we found a 22.9% prevalence of TTH, which is close to the 22.3% reported by Igarashi and Sakai (34) in Japan, to the 26.5% noted by Alders et al. (24) in Malaysia, and to the 26.9% described by Lavados and Tenhamm (33) in Chile. In our survey, the prevalence of TTH was higher in the age group 15–24 years. We noted decreasing prevalence rates with increasing age, in concordance with some other studies (23, 24, 28, 39).
We found a 6.4% 1-year prevalence of CDH, which is slightly higher than the rates previously described in the literature (35–38); but if we consider the low figure of the 95% CI (4.7%), it is equal to the 4.7% reported by Castillo et al. (35) in Spain, and similar to the 4.1% noted by Scher et al. (37) in the USA. Because we did not use diaries to confirm the reported frequency of the headaches, there might be some recall bias, which may account for this high prevalence rate. Most (80%) subjects with CDH were diagnosed as ‘chronic migraine’, including individuals who fulfilled the criteria for migraine or ‘migrainous disorder’. Scher et al. (37) reported a higher proportion of chronic TTH, but some authors (35, 36, 38) described higher rates of ‘chronic migraine’. The disproportion between ‘chronic migraine’ and ‘chronic tension-type headache’ in our study may be due to the possibly overestimated high prevalence rates of migraine and ‘migrainous disorder’.
There are a few studies (4, 15, 16, 30), all in the USA, which noted a higher prevalence of migraine in subjects with a lower household income. We also noted an inverse relationship between migraine prevalence and household income. This finding was corroborated by a higher proportion of subjects with migraine in households with lower electricity consumption per capita per month. This variable seems to be a fair and objective marker of the socioeconomic level of the population, at least in underdeveloped countries.
Stang and Osterhaus (4) reported a higher prevalence of migraine in subjects of higher education level. We did not find this relationship, nor did most other studies on this topic (6, 8–10, 12, 16).
The association between migraine and marital status is not well established. In three studies (6, 9, 16) that looked at this subject, no relationship was detected. In this study, we noted 60% more migraine in single persons than in those divorced or widowed. Rozen et al. (46), justifying a higher incidence of migraine in women, many of then divorced, in Olmsted County, MN, USA, attributed this to a stressor factor.
In conclusion, we have shown high prevalences of migraine and CDH in Florianopolis, Brazil, close to the higher rates of previous studies. There is a preponderance of migraine in females, divorced or widowed, with a low socioeconomic level.
Footnotes
Acknowledgements
The authors thank Dr Alan M. Rapoport for reviewing the manuscript.