
Abstract
Background:
Headaches represent a significant proportion of referrals to any neurology consult service, of which many are migrainous. Regular use of opioids can lead to medication overuse headache in these patients and in some cases, dependence. The epidemic of opioid abuse represents a serious public health concern, with long term use of opioids associated with risk of misuse, abuse, addiction and even overdose.
Methods:
We audited headache referrals to the neurology consult service in an acute tertiary hospital over three 6-month periods between 2012 and 2019. Appropriateness of referrals with respect to NICE guidelines and initial treatments strategies were assessed.
Results:
The majority of headache disorders seen were migrainous and we found an alarming and repeated trend of early opioid prescribing in the initial acute setting (up to 56%).
Conclusions:
Further education of healthcare professionals and patients is urgently required to prevent this group becoming victims of the growing global opioid epidemic.
Keywords
Introduction
We have noted over the last few years that the World Health Organisation ‘pain ladder’, 1 designed for cancer pain relief, is often employed by primary care physicians and even in some emergency departments for the management of headache disorders. However, the prolonged use of these agents can lead to medication overuse headache. 2 In addition, the epidemic of opioid abuse represents a serious public health concern among physician prescribers and emergency departments, 3,4 with long term use of opioids associated with risk of misuse, abuse, addiction and even overdose. 5 Headache specific treatment guidelines (e.g. NICE) have been published but compliance with such guidelines is unclear. 6
Methods
We undertook a chart review to audit headache referrals from general medical teams to the neurology consult service in the author’s institution, an acute tertiary hospital, over three 6-month periods between 2012 and 2019. Approval from our institution’s audit committee was obtained. The first study period was prior to the publication of the NICE guidelines and the subsequent study periods were thereafter. Appropriateness of referrals with respect to NICE guidelines and initial treatment strategies were assessed. Interventions to highlight appropriate treatment of acute headache with emergency department staff and general physicians were instituted after each audit cycle. Unpaired t-tests and Pearson chi-square tests were employed to examine demographic differences between migraine, non-migraine and medication overuse subgroups and trends in prescribing pattern over time. Trends in prescribing between migraine and non-migraine subtypes were examined using two-way ANOVA.
Results
A total of 167 headache referrals were received over the three audit periods. The breakdown of headache diagnoses by year is shown in Table 1. The predominant headache diagnosis was migraine (67–73%). The mean age of the total cohort was 41 years (range 17–86), 65% of whom were female. Those who were diagnosed with migraine were of a similar age to the non-migraine group but the predominance of females within the migraine group was greater (83% vs 52%, p = 0.01). Those diagnosed with medication overuse were non-significantly older (45 years, range 19–61, p = 0.27) with a gender distribution matching the total cohort. Demographics are summarized Table 2.
Breakdown of headache diagnoses for entire study period.

Demographics of migraine, non-migraine and medication overuse cohorts.

The majority of patients (88%) were investigated in accordance with NICE guidelines. The remaining 12% were investigated in spite of not meeting NICE guideline red flag recommendations for investigation. We observed a significant increase in the use of paracetamol (2012: 68%; 2015: 77%; 2019: 93%, p = 0.004) but no reduction in the use of opioid analgesics (2012: 47%; 2015: 45%; 2019: 56%, p = 0.404) in the acute setting across all headache types. This was in spite of interventions to highlight the importance of avoiding this practice. Similarly, prescription of non-steroidal anti-inflammatories (2012: 44%; 2015: 48%; 2019: 47%, p = 0.752) and triptans (2012: 7%; 2015: 3%; 2019: 7%, p = 0.319) remained stable over time. There was no significant difference in these trends when divided into migraine and non-migraine subtypes (p = 0.35). 88% of all patients prescribed opioids were also prescribed paracetamol +/− NSAID suggesting escalation along the WHO pain ladder. These trends and a breakdown of opiate medications prescribed are shown (Figure 1).
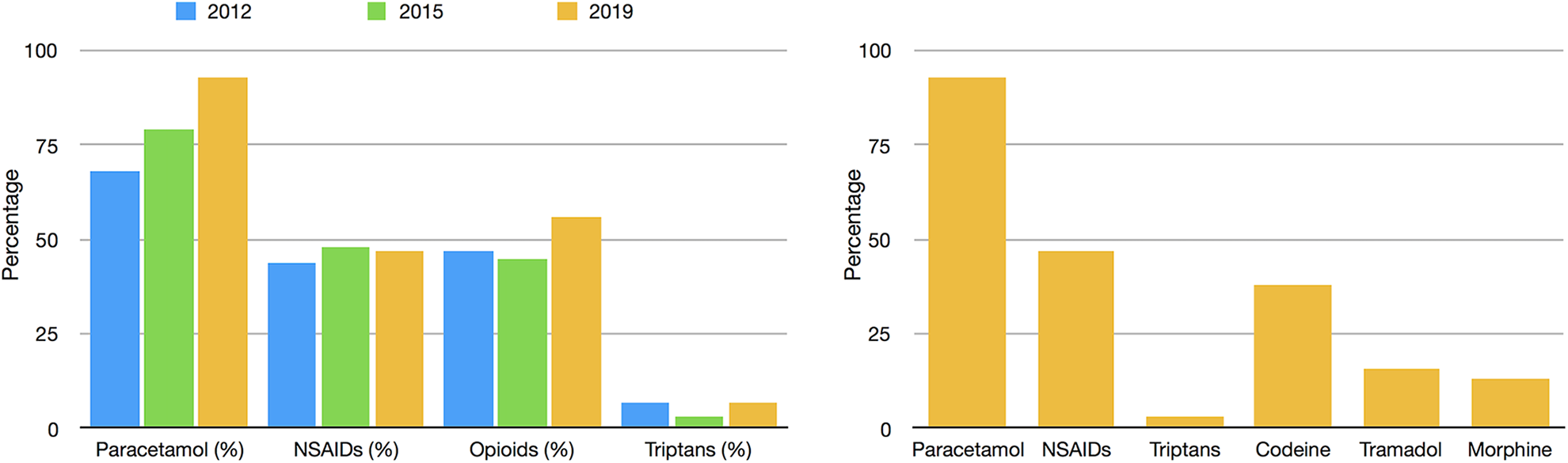
Percentage of patients prescribed analgesia types by year (left) and percentage of specific medication classes prescribed in 2019 (right).
Discussion
Our results suggest that, despite the fact that the predominant headache diagnosis referred is migraine, the reliance on acute analgesia (in particular opioids) has not changed in spite of interventions to highlight these concerning patterns. The second striking finding is the very low use of triptans in the acute setting. This is in spite of repeated interventions to curb this trend, suggesting an ingrained mentality towards prescribing opiates for headache in the acute setting. Although acute use of analgesia in the setting of migraine is not necessarily in itself a problematic issue, the pattern of prescribing, with escalation from simple analgesia to opioids if pain control is ineffective, rather than use of migraine specific treatments such as triptans, is similar to that of the WHO ‘pain ladder’ (although statistical comparison was not undertaken). This approach was validated for pain relief in cancer but not for other types of chronic pain. Although subgroups of patients with chronic pain may obtain sustained relief with stable doses of opioids, the negative effect of medication overuse on chronic daily headache is well documented. 7 In addition, those with episodic migraine who overuse opioids are more likely to progress to chronic migraine than with other analgesics. 7 The reasons for the low use of triptans acutely is unclear but also clearly needs to be addressed.
This study has a number of limitations. The primary reason for admission to hospital was not recorded. As a result, possible contraindications to use of NSAIDs or triptans may have been missed. For this reason there may have been alternative reasons for the high use of opioids. However, one would expect the prescribing of opioids to fall following interventions to address these trends. Furthermore, given that this was a chart review, it was not possible to classify the majority of these patients using the International Classification of Headache Disorders, 3rd edition.
The worldwide opiate problem highlights the significant risk of misuse, addiction and suicide with chronic use of these agents. 5 Opioid overdoses kill over 130 Americans every day and the pattern of prescribing among U.S. physicians has received scrutiny in recent years. 3,4 Although the data presented here is from a single institution, we suspect similar patterns may exist in other jurisdictions. Indeed, Woolley et al. showed an excess of opioid prescribing in comparison to triptans in commercially insured patients with migraine in the United States. 8 Efforts have been made to curb the use of opioids in the in-patient and emergency department settings with some effect but larger structured programmes are required. 9,10 Initial prescription of opioids can be innocuous but can quickly lead to dependence, particularly in patients who experience chronic pain. Individuals with chronic daily headache require multidisciplinary approaches to symptom management rather than early introduction of acute analgesia which may worsen their condition. Further education of healthcare professionals is urgently required to prevent this group becoming victims of the growing opioid epidemic.
Clinical implications
Early opiate prescribing and use of the WHO pain ladder should be avoided in the management of headache
Initial prescription of opioid can be innocuous but can quickly lead to medication overuse headache and dependence
Further education of healthcare professionals is urgently required to prevent this group becoming victims of the growing global opioid epidemic
Footnotes
Author contributions
CF, KM contributed equally to this work. All authors have made substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data, drafting the work or revising it critically for important intellectual content. All have given final approval of the version published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.