
Abstract
It is generally accepted that ongoing medication overuse nullifies the effect of prophylactic treatment, although few data support this contention. We set out to describe the treatment outcome in patients withdrawn from medication overuse and relate any improvement to a renewed effect of prophylaxis. For patients with probable medication-overuse headache (pMOH), treated and dismissed from the Danish Headache Centre in 2002 and 2003, we assed, from prospective headache diaries, the headache frequency before and after withdrawal of offending drugs and compared these frequencies with the headache frequency at dismissal. Among 1326 patients, 337 had pMOH. Eligible were 175, mean age 49 years, male/female ratio 1: 2.7. Overall, there was a 46% decrease in headache frequency from the first visit to dismissal (P < 0.0001). Patients with no improvement 2 months after complete drug withdrawal (N = 88) subsequently responded to pharmacological and/or non-pharmacological prophylaxis with a 26% decrease in headache frequency as measured from the end of withdrawal to dismissal (P < 0.0001). At dismissal, 47% were on prophylaxis. Former non-responders to medical prophylaxis had a 49% decrease in headache frequency from first visit to dismissal (P < 0.0001), whereas those who had never received prophylaxis had a 56% reduction (P < 0.0001). This difference was not statistically significant (P = 0.22). Almost all MOH patients benefit from drug withdrawal, either just from the withdrawal or by transformation from therapeutic non-responsiveness to responsiveness. According to the International Classification of Headache Disorders, 2nd edn, the MOH diagnosis requires improvement after drug withdrawal. Our data suggest that these diagnostic criteria are too strict.
Keywords
Introduction
Overuse of acute migraine medication and plain analgesics is a well-known problem which has been described repeatedly over the last several decades (1–4). In a recent study, we confirmed that patients with overuse improve simply by being kept medication free for 2 months (5). While this was the overall result, patients segregated clearly into three groups: one with improvement (45%), one that stayed unchanged (48%) and a small group of 7% which deteriorated. This was perhaps a smaller percentage of improvement than had been expected from the previous literature (6–8) and the issue therefore was whether or not there are other benefits to the patients who did not improve merely by discontinuation of the overused drug. In the absence of data, it is generally accepted that patients are refractory to prophylactic treatment while having medication overuse and that they become responsive after medication withdrawal. The primary aim of the present study was therefore to describe the treatment outcome of patients withdrawn from medication overuse after initiation of pharmacological and/or non-pharmacological prophylactic treatment. The secondary aim was to relate improvement to a renewed effect of prophylactic medication. We followed up at dismissal a previously published study of patients from the Danish Headache Centre (DHC) (5) who were kept medication free for 2 months and analysed the response of these patients to prophylactic treatment. Our hypothesis was that this group of severely affected patients, previously totally refractory to treatment at other clinics, would become responsive to therapy after withdrawal.
Materials and methods
DHC is a tertiary out-patient referral Headache Centre. It functions as the only national referral centre for severely affected headache patients in Denmark (5.4 million inhabitants). At the time of this study, only referrals made by neurologists were accepted.
All patients dismissed from DHC in 2002 and 2003 had been mailed a diagnostic headache diary 1–2 months before the first visit. For the present study diaries were available for 83% of the patients. Questionnaires recorded by the doctor at the final visit describing headache frequency and medication use at dismissal were also available. Diagnoses, headache frequency and medication use were determined from these prospective recordings and loaded into a Microsoft Access 2002 database together with information on socio-economic status and previous pharmacological and non-pharmacological treatment. The patients were primarily diagnosed according to International Classification of Headache Disorders (ICHD)-I, but data allowed a subsequent reclassification according to ICHD-II.
After establishment of a diagnosis of probable medication-overuse headache (pMOH) (9), all acute headache medication was discontinued abruptly and patients were kept medication free for 2 months as part of the general treatment programme in DHC (10). In the case of severe opioid overuse, phenobarbital substitution was used for a short period to avoid abstinence syndromes. Overuse of barbiturates or benzodiazepines must be tapered slowly, but marked overuse of these substances was not documented among our patients. Levomepromazine or promethazin was allowed as the only rescue medication during withdrawal, primarily to be used for the first week. After withdrawal, headache frequency was reassessed and diagnoses were revised. At this time medical and/or non-medical prophylactic treatment was initiated if needed and symptomatic medication was resumed, but with a strict upper limit of maximally 6 days per month as agreed by the patient. As part of the non-pharmacological treatment strategy, patients with significant pericranial muscle tenderness were referred to physiotherapy and referral to a psychologist was initiated if comorbid psychiatric disorder was suspected, if pharmacological treatment was insufficient or if the patient expressed specific interest in psychological treatment.
Statistics
Based on their primary headache diagnoses, the eligible patients were divided into four groups: migraine, tension-type headache (TTH), mixed migraine and TTH (MT) and other diagnoses (OD). Wilcoxon’s signed rank test was used for paired comparisons of headache frequencies within groups.
All comparisons between groups have been adjusted for variations in the initial headache frequency using a stratum-adjusted Kruskal–Wallis test. Post hoc tests were performed using a stratum-adjusted Kruskal–Wallis test with the step-down Bonferroni method of Holm adjustment for multiple testing. P-levels < 0.05 (two-tailed) were chosen as the level of significance. Statistical analysis was performed using SAS version 8.2 (SAS Inc., Cary, NC, USA). Mean values are presented with median values in parentheses and range in square brackets.
Results
Among 1326 patients treated and dismissed from DHC in 2002 and 2003, we identified 337 (25%) with an initial diagnosis of pMOH. We excluded 121 who did not stay medication free for 2 months, leaving 216 patients of whom 45% had a reduction in headache frequency by mere discontinuation of the offending drug, 48% were unchanged following withdrawal and 7% had an aggravation (5). Among these 216 patients, 39 were later administratively dismissed because of failure to appear and for two patients information regarding headache frequency at dismissal was missing, leaving 175 patients eligible for the present study. The excluded patients were slightly younger (mean age 44 years vs. 49 years) and a smaller proportion overused ergots/triptans (14% vs. 26%). There were no significant differences between excluded and enrolled patients with regard to sex, primary headache diagnoses or initial headache frequency.
Among the 175 enrolled patients there were 47 men (27%) and 128 women (73%) with a mean age of 49 years (range 17–86 years). Seventeen patients (10%) had migraine, 58 (33%) had TTH, 79 (45%) had mixed migraine and TTH and 21 patients (12%) had other headache diagnoses, where post-traumatic headaches, which had markedly worsened during overuse, accounted for the majority (N = 12). All diagnostic groups had a significant decrease in headache frequency from first visit to dismissal. Overall, the mean headache frequency at first visit was 27 days/month (range 15–30 days/month) and at dismissal 15 days/month (range 0–30 days/month). This corresponds to an overall decrease in headache frequency from first visit to dismissal of 46% (P < 0.0001) (Table 1). The average time from the end of withdrawal to dismissal was 228 days (range 0–1422 days) for all patients. Figure 1 illustrates the development in headache frequency from the first visit through the end of medication withdrawal to dismissal for all patients.
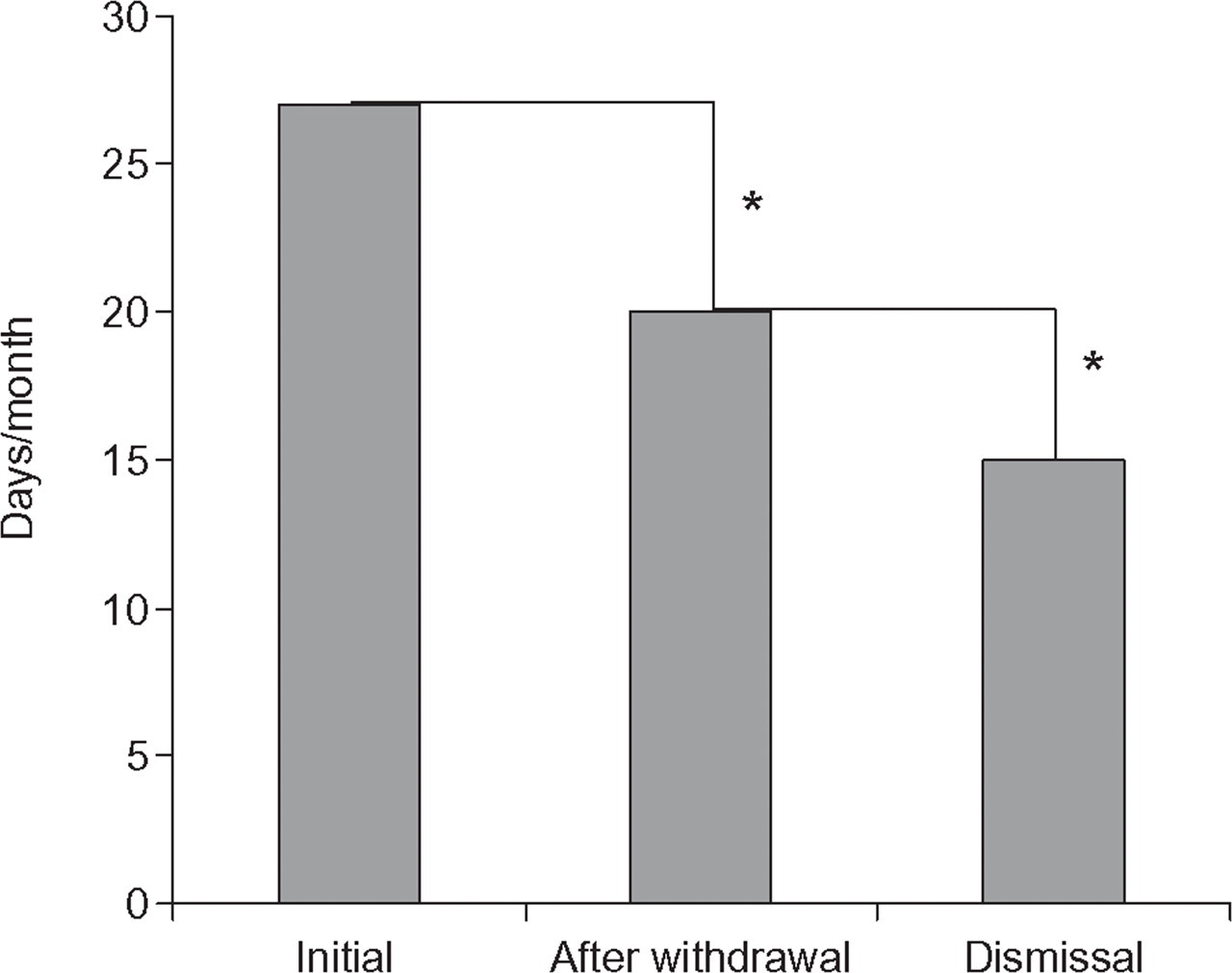
Development in headache frequency for patients withdrawn from medication overuse (N = 175). ▪, Headache frequency. ∗P < 0.0001.
Clinical characteristics and treatment results for all patients withdrawn from medication overuse

Mean values, median values in parentheses and range in square brackets.
P < 0.001;
P < 0.0001.
TTH, Tension-type headache.
Eighty-eight patients (50%) had no initial decrease in headache frequency following medication withdrawal. Four patients (5%) had migraine, 37 (42%) had TTH, 29 (33%) had mixed migraine and TTH and 18 patients (20%) had other headache diagnoses. All diagnostic groups had a significant decrease in headache frequency from the end of withdrawal to dismissal, except for pure migraine where the trend was the same but not significant, probably due to the small number. Overall, the mean headache frequency after withdrawal was 29 days/month (range 19–30 days/month) and at dismissal 22 days/month (range 0–30 days/month). This corresponds to an overall decrease in headache frequency from the end of withdrawal to dismissal of 26% (P < 0.0001) (Table 2). Comparing migraine, TTH, MT and OD, the reduction in frequency differed significantly between the diagnostic groups (P = 0.022). Post hoc analysis showed a significantly smaller reduction in TTH than in migraine and TTH (P = 0.041) and other diagnoses (P = 0.047). All other comparisons were insignificant. The average time from the end of withdrawal to dismissal was 249 days (range 0–690 days) for the non-improving group. Figure 2 illustrates the development in headache frequency from the first visit through the end of withdrawal to dismissal for the patients who experienced no initial effect of medication withdrawal.
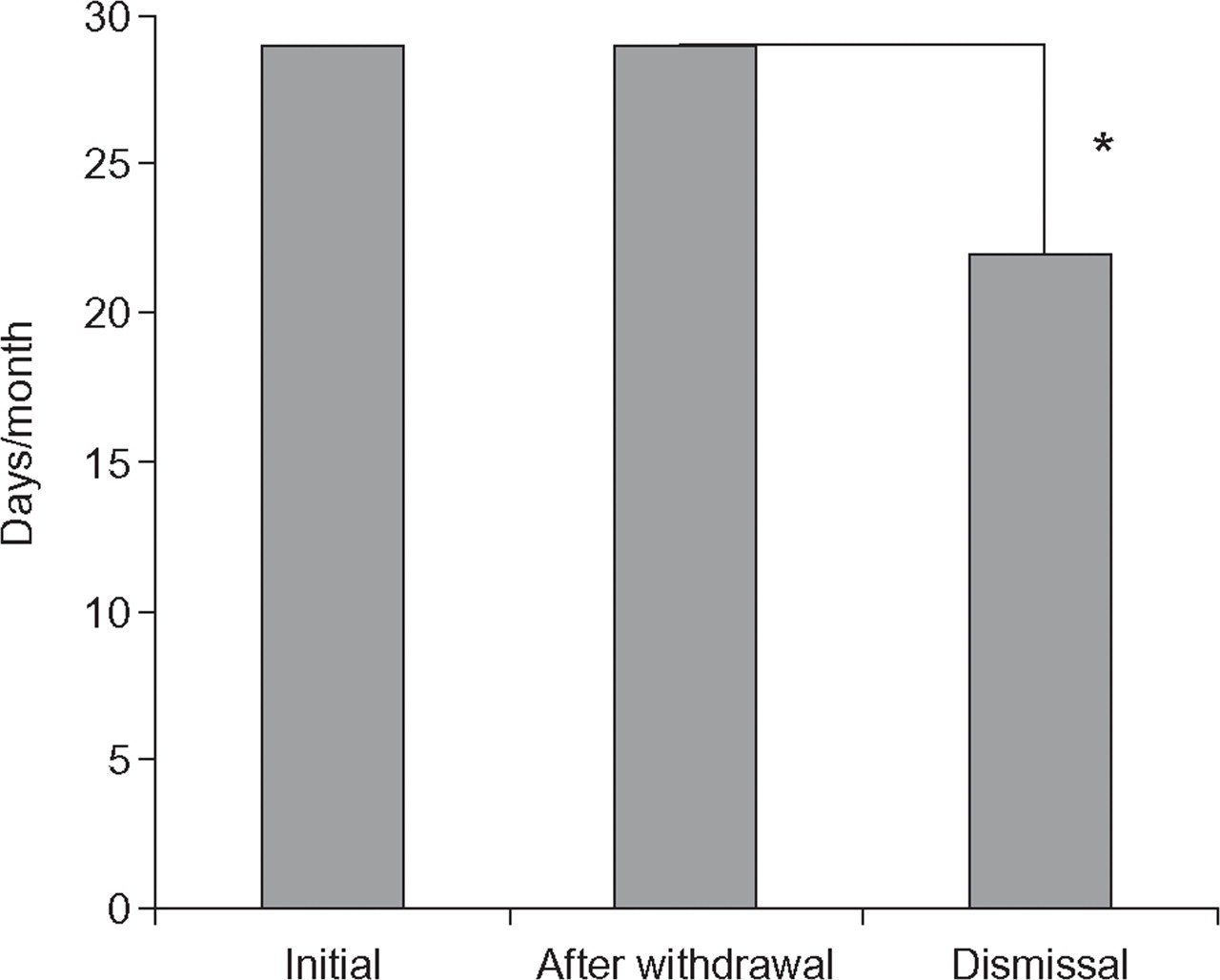
Patients with medication overuse and no improvement in headache frequency following a 2-month drug-free period (N = 88). ▪, Headache frequency. ∗P < 0.0001.
Treatment results for patients with medication overuse and no improvement in headache frequency following a 2-month drug-free period
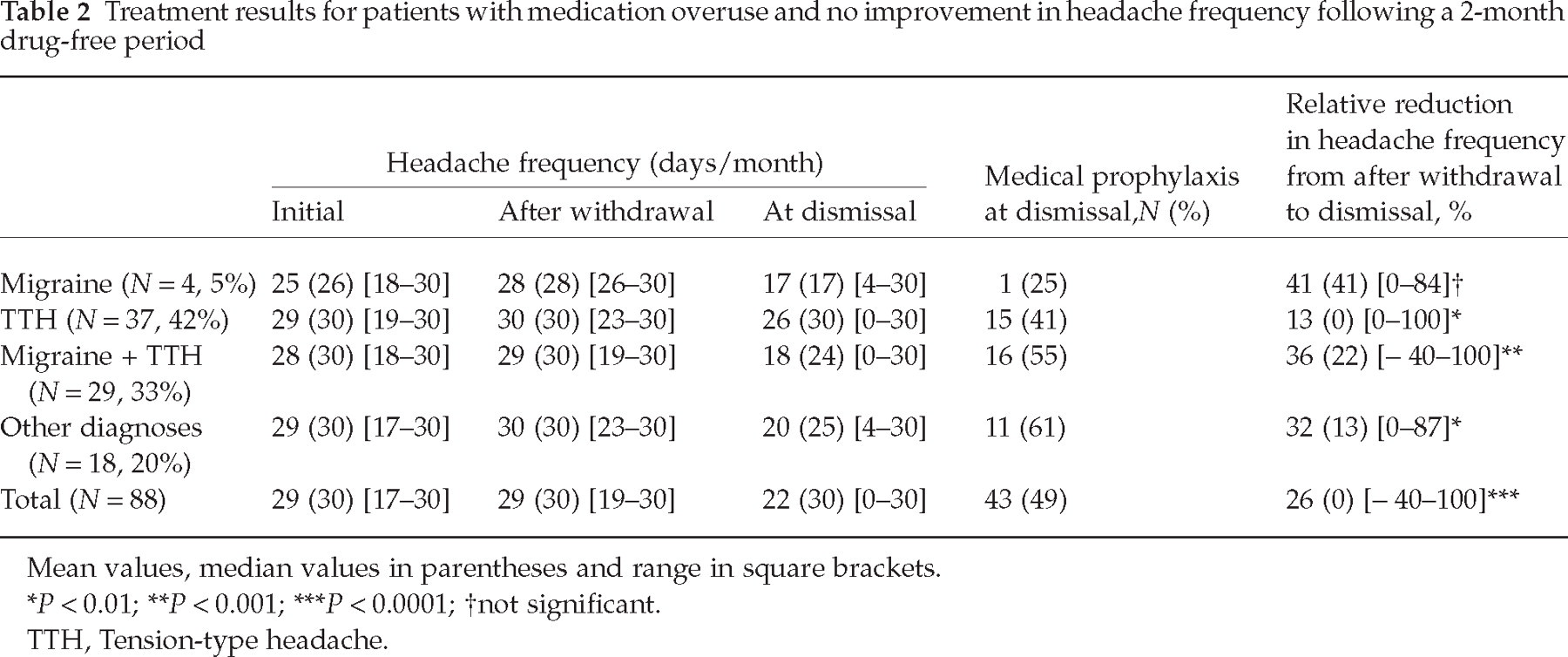
Mean values, median values in parentheses and range in square brackets.
P < 0.01;
P < 0.001;
P < 0.0001;
not significant.
TTH, Tension-type headache.
Those 87 patients (50%) who did improve following the initial 2 months’ medication withdrawal had a slight further improvement from the end of withdrawal to dismissal with an overall additional mean reduction of 2 days/month (P < 0.01). For the specific diagnostic groups the reduction was significant only for mixed migraine and TTH (P = 0.003). The average time from the end of withdrawal to dismissal for these patients was 207 days (range 0–1427 days).
Overall, 69% of the patients received preventive medication following withdrawal. Due to either intolerance or lack of effect the treatment was abolished for some of the patients. At time of dismissal, 47% of our patients were on medical prophylactic treatment (Table 1) and 44% had a history, before admission to DHC, of prior medical prophylaxis without effect, with an average of 1.6 (1–5) drugs with different medical profiles (antiepileptics, β-blockers, non-steroidal anti-inflammatory drugs, Ca-antagonists, antidepressants, others). In order to elucidate a possible renewed effect of medical prophylaxis after medication withdrawal, we divided the patients on prophylactic treatment at dismissal into two groups based on whether or not they had received prior medical prophylaxis without effect. The mean relative reduction in headache frequency from first visit to dismissal was 49% (P < 0.0001) for the known non-responders to medical prophylaxis and 56% (P < 0.0001) for those who had never received prophylaxis. This difference was not statistically significant (P = 0.22) (Table 3).
Patients withdrawn from medication overuse and on medical prophylactic treatment at dismissal

Mean values, median values in parentheses and range in square brackets.
N is 80 and not 82 due to missing values for two patients regarding prior medical prophylaxis.
P < 0.0001.
Discussion
This study shows that patients with medication overuse, who have no improvement in headache frequency, by mere discontinuation of the offending drug subsequently become responsive to therapeutic intervention in the time period after drug withdrawal.
Excluding patients who did not stay medication free during withdrawal and subsequently excluding patients who were administratively dismissed due to failure to appear, resulted in a 50% exclusion rate. Even then, our sample size is fairly large. As in all open studies, bias is a possibility. The prospective headache data, however, minimize the risk of bias and comparisons between diagnostic groups are unbiased. In addition, there is no social bias because medical treatment is free for all residents in Denmark. All our patients had a long history of refractory headaches and had consulted one or several neurologists before admission. The latter was due to the referral criteria of DHC. It is therefore unlikely that the observed improvement from the end of withdrawal to dismissal is a simple placebo or time effect. It is important to emphasize that generalization of the results must be made with caution. Yet there were no difference between enrolled and excluded patients with regard to sex, primary headache diagnoses or headache frequency, the excluded were slightly younger and fewer overused specific migraine drugs. Furthermore, few if any headache clinics keep their patients completely drug free for 2 months and most allow prophylactic treatment before 2 months.
The age was slightly older and with less female preponderance compared with other studies (1, 4, 11–13). In a meta-analysis by Diener and Dahlöf of 29 studies, 65% had migraine as primary headache, 27% TTH and 8% mixed migraine and TTH or other headache diagnoses (8). The present study had a much smaller proportion of pure migraine (10%), a larger proportion of TTH (33%) and a much larger proportion of mixed migraine and TTH (45%) and OD (12%). This is probably due to our systematic prospective use of diagnostic diaries where all headaches are recorded. As shown by Russell et al., episodic TTH is usually underdiagnosed and migraine overdiagnosed in a diagnostic interview compared with a diagnostic diary (14).
For all patients together the relative reduction in headache frequency from the first visit to dismissal was 46%. The variation between the diagnostic groups ranged between 30% for TTH and 64% for pure migraine. Patients with mixed migraine and TTH had a 55% reduction. These results are somewhat smaller than the 74% decrease in headache frequency found by Bigal et al. 1 year after a successful and maintained detoxification in patients with so-called transformed migraine (1).
The most remarkable result in the present study was the long-term treatment benefit for the subgroup of patients who had absolutely no initial improvement in headache frequency following a 2-month drug-free period. Our data show that one can expect a significant positive therapeutic response after withdrawal for these patients, with a relative reduction of 26% over a period averaging 249 days. TTH patients had a significantly poorer outcome with a mean relative reduction of 13% compared with 36% for mixed migraine and TTH and 32% for OD. The largest improvement was observed in the group with pure migraine (41%), yet this was not significant due to the small number of patients. These findings are in aggreement with other studies which have reported a worse long-term prognosis for TTH compared with migraine following drug withdrawal (15, 16). We have previously shown that, using headache frequency as the sole efficacy measure, the improvement following medication withdrawal is less pronounced in TTH compared with migraine (5) and have suggested that both intensity and duration of the individual headache episode should be included in the evaluation of treatment outcome in TTH. The poorer long-term treatment outcome in TTH is likely also to reflect the lesser efficacy and the small number of available prophylactic drugs compared with migraine.
It is generally assumed that medication overuse nullifies the effect of prophylactic agents. The evidence in the literature is, however, sparse (4). We therefore wanted to relate the long-term treatment outcome to a possible renewed effect of medical prophylaxis. For this aim it is a problem that DHC is a multidisciplinary headache clinic with standardized procedures for the treatment of MOH involving doctors, nurses, physiotherapists and psychologists (10). As most of the patients receive combined therapy, it was not possible to ascribe the overall outcome with certainty to prophylactic drug treatment. We therefore looked at the 80 patients on medical prophylactic treatment at dismissal. Of these, 43 patients had a history of prior medical prophylaxis with no effect on their headaches, while 37 had never tried prophylactic agents. Comparing the treatment outcome for these two groups, one would expect a poorer outcome among the patients with a known non-response to medical prophylaxis. However, we found a highly significant relative reduction in headache frequency from first visit to dismissal for both groups and no significant difference between groups. The former non-responders had a 49% reduction and the patients with no prior history of prophylaxis reduced their frequency by 56%. This strongly suggests a renewed effect of prophylaxis after medication withdrawal and that medication overuse nullifies the effect of prophylactic agents.
Our data are important in relation to the diagnostic criteria for MOH according to the International Classification of Headache Disorders, 2nd edn. In order to receive the MOH diagnosis, it is required that patients must improve after drug withdrawal. This was the case in only half of our patients. However, the other half who did not improve became responsive to pharmacological and non-pharmacological therapeutic intervention. Thus, the vast majority of patients had a positive result of drug withdrawal, suggesting that the criteria for MOH in ICHD-II are too strict.
In summary, this study shows that almost all MOH patients benefit from drug withdrawal, either directly or by transformation from therapeutic non-responsiveness to responsiveness.
Conflict of interest
None declared.
Footnotes
Acknowledgements
The authors thank Mrs Hanne Andresen for technical assistance during data collection. The study was supported by grants from ‘IMK Almene Fond’. The funding source was not involved in any stage of the study.