
Abstract
Background:
Treating migraine attacks early may improve outcome. The aim of this analysis was to investigate whether certain premonitory symptoms could be indicators for taking acute medication.
Methods:
We analyzed 3-month diary data recorded by 271 patients with episodic migraine and looked at all migraine-free intervals. For investigating the interaction between acute medication and neck discomfort associated with sensitivity to lights, noises, or odors, we used a marginal structural model and a Cox regression analysis adjusted for moderate or severe headache.
Results:
The patients (mean age 43 ± 15.4 years, 88% women) recorded a total of 20,219 diary days without migraine. In the marginal structural model analysis, the risk for occurrence of a migraine attack on the subsequent day was reduced when acute medication was used in the presence of neck discomfort associated with sensitivity to lights (hazard ratio 0.4; 95% confidence interval 0.2–0.7), noises (0.4; 0.3–0.7), or odors (0.2; 0.1–0.4). The marginal structural model showed lower risk of migraine attacks than the Cox regression analysis adjusted for moderate or severe headache in the majority of the cases.
Conclusion:
Migraine attacks may be prevented when acute medication is used in the presence of neck discomfort associated with sensitivity to lights, noises, or odors. The results of this study may stimulate further prospective trials.
Keywords
Introduction
Migraine is a chronic recurrent neurological disorder which has a great impact on the lives of affected people and their quality of life. 1 It represents an economic problem for the society due to the loss of work time and reduced productivity. 2 In traditional trials for establishing the efficacy of triptans, patients were usually advised to take acute medication when the intensity of headache was at least moderate. 3 The same advice was given in a recent study on lasmiditan. 4 With this advice, patients are more likely to treat a true migraine attack rather than a non-migrainous headache and the risk of medication overuse may be diminished. On the other hand, taking acute medication with a moderate or severe headache may not be the optimal strategy for the majority of patients. Indeed, some studies indicate that taking acute medication earlier may improve the efficacy of acute medication. 5 –8
An important issue is to detect alternative indicators for the timing of acute medication to improve the current practice of treating migraine attacks. A general approach to address this question could be to identify premonitory symptoms which could be indicators for the use of acute medication early in an attack. 9
We used this strategy and reanalyzed the data of a large prospective diary study. 10 For our analyses, we chose neck discomfort and sensitivity to lights, noises, or odors recorded in the patient’s diaries. We chose neck discomfort because it was most frequently associated with migraine attacks both on a population level and in individual n = 1 analyses in our own data set, 10,11 and it was one of the most common premonitory symptoms in other studies. 12,13 We chose sensitivity to lights, noises, or odors because such sensitivity is specifically related to migraine attacks. 14 –16
The aim of this study was to assess the prevalence of neck discomfort and sensitivity to sensory stimuli as well as the use of acute medication on migraine-free days in patients with episodic migraine, to analyze the impact of these symptoms on the risk of a forthcoming migraine attack, and to investigate whether neck discomfort and sensitivity to lights, noises, or odors could be indicators for taking acute medication early during the premonitory phase of a migraine attack.
Patients and methods
This study was approved by the Ethics Committee (1777/2019), and data transfer to the University of Bremen was approved by the Data Protection Committee at the Medical University of Vienna. Formal co-operation was approved by the Legal Departments at the Medical University of Vienna and the University of Bremen.
The pseudonymized data analyzed in this article were collected in a prospective cohort in Austria. The details of the methodology have been published previously. 10 Briefly, patients with migraine without or with aura were recruited via articles in newspapers and filled in a comprehensive paper–pencil diary regardless of the absence or presence of headache every evening over a period of 3 months. Inclusion criteria comprised a diagnosis of migraine without aura or migraine with aura according to the second edition of the International Classification of Headache Disorders (ICHD-2) 17 and a minimum of one migraine attack per month in the preceding 6 months. Exclusion criteria were clinically relevant other diseases and headaches except for tension-type headache.
The diary covered hormonal, psychological, and environmental factors, daily activities, sleep and tiredness, nutrition, consumption of alcohol, and smoking. In addition, the participants recorded all headache characteristics required for classifying each single headache as migraine or non-migrainous headache. The diagnostic algorithm was based on ICHD-2 criteria B (headache duration), C (headache characteristics), and D (associated symptoms) of migraine without aura. We classified headaches fulfilling all three criteria as migraine without aura, headaches fulfilling two criteria as probable migraine, and headaches fulfilling one or no criterion as non-migrainous. 17
In the initial study, a total of 327 patients enrolled and stepwise multivariate Cox regression analyses revealed that menstruation, neck discomfort, physical tension, tiredness, and sensitivity to noises and odors increase the hazard of getting a migraine attack. For the current analyses, we excluded 56 of the initial 327 patients, 46 because they had 15 or more headache days per month and 10 because they did not record any day with definite or probable migraine without aura. Accordingly, the final data set was composed of 271 patients.
The analysis was based on the time intervals between two successive migraine attacks starting with the day after a migraine attack and ending with the day before the onset of the next attack. For each patient, data analysis started with the first completely observed migraine-free interval. This provided a total of 20,219 observation days. Acute medication comprised non-opioid analgesics, combination-analgesics, opioids, ergotamines, triptans, and antiemetics. Definite or probable migraine was the main outcome variable.
For a complete understanding of the findings, we additionally analyzed the headache-free periods, that is, the time intervals between any headaches. This analysis included 281 patients with at least one headache day and comprised 18,237 observation days. The outcome parameters corresponded to those for the migraine-free intervals and covered prevalence of neck discomfort and sensitivity to sensory stimuli, use of acute medication, impact of these symptoms on the risk of headache on the subsequent day, and the association between the use of acute medication and the risk of forthcoming headache of any type.
Statistical analysis
Descriptive statistics comprised the number and proportion of migraine-free days with moderate or severe headache, neck discomfort, sensitivity to lights, noises, or odors and specific combinations of these symptoms as well as the number and proportion of patients for whom these symptoms were present on at least one day. The different types of acute medications were summarized by absolute and relative frequencies (%). In addition, we prepared cross-tables for premonitory symptoms with moderate or severe headache and for acute medication with the symptoms of interest. To characterize the association of specific symptoms with the risk of developing a migraine attack we performed univariate Cox regression analyses and provided hazard ratios and 95% confidence intervals.
The effect of using acute medication in the presence of neck discomfort and sensitivity to lights, noises, or odors was analyzed by means of a marginal structural model allowing for the interaction between acute medication and the premonitory symptom under consideration. The marginal structural model is a weighted Cox regression analysis that accounts for baseline and time-varying confounders. 18 With the marginal structural model, one builds a pseudo-population where treatment is un-confounded with the covariates accounted for in the model for the inverse probability weights. The marginal structural model allows for avoiding or at least substantially reducing a bias due to time-dependent confounding. 18 We refrained from applying only the Cox proportional hazard model with the mentioned confounders as time-dependent covariates because it may not have provided sufficient power and may be biased. 19
The weights were estimated with the R-package ipw (inverse probability weighting). 20 The results were compared with a classical Cox regression analysis with the same interaction treatment factor and including moderate or severe headache as covariate.
To account for the repeated time intervals within a patient, we used robust standard errors and p-values. For computing the stabilized weights in the marginal structural model, we accounted for a total of 21 baseline and time-dependent confounders, that is, age, gender, private stress, stress at work, tiredness, sleeping too long, restless sleep, sleep deprivation, hunger, skipping meals, smoking, consumption of alcohol, sensitivity to lights, noises, or odors, neck discomfort, menstruation (days −2 and −1, days 1–3 and days 4+), moderate or severe headache, and nausea. In our causal model, we deliberately avoided to control for too many confounders, as it may have led to the violation of the positivity assumption and the variance in the final estimates might increase. The positivity assumption requires that all treatment or covariate combinations are possible so that no patient can have probability zero or one for being treated. 21 To avoid estimation of reversed causal effects, we shifted the state variable (migraine yes/no) to the day before, that is, the state variable of each day had the value of the subsequent day and acute medication, premonitory symptoms and time-varying confounders were taken from the day on whom they had been observed. For the complementary analysis of the headache-free intervals, we performed corresponding statistical analyses.
Results
Our analyses were based on 271 patients with migraine (mean age 43 ± 15.4 years, 88% women) and 20,219 observation days, that is, days with non-migrainous headache or without headache. The use of acute medication was recorded on 2938 days (15%). Most of the patients, namely 93%, took acute medication on at least one day. Eight patients (3%) used acute medication on more than 10 days per month on average. As expected, moderate or severe headache was the dominating reason for using acute medication.
Table 1 presents that neck discomfort was present on more than half of the days without migraine and that almost all patients recorded at least one day with neck discomfort. Sensitivity to lights, noises, or odors was present on 6–16% of the days and the proportion of patients who recorded at least one day with such sensitivity ranged between 62% and 87%. Neck discomfort was associated with sensitivity to lights, noises, or odors on 14% of the days and this association was found in more than 80% of the participants on at least one day.
Prevalence of headache and other predefined symptoms on migraine-free days in 271 patients with migraine.a

a The proportion of days and the proportion of patients for whom a specific symptom was present on at least one day is listed.
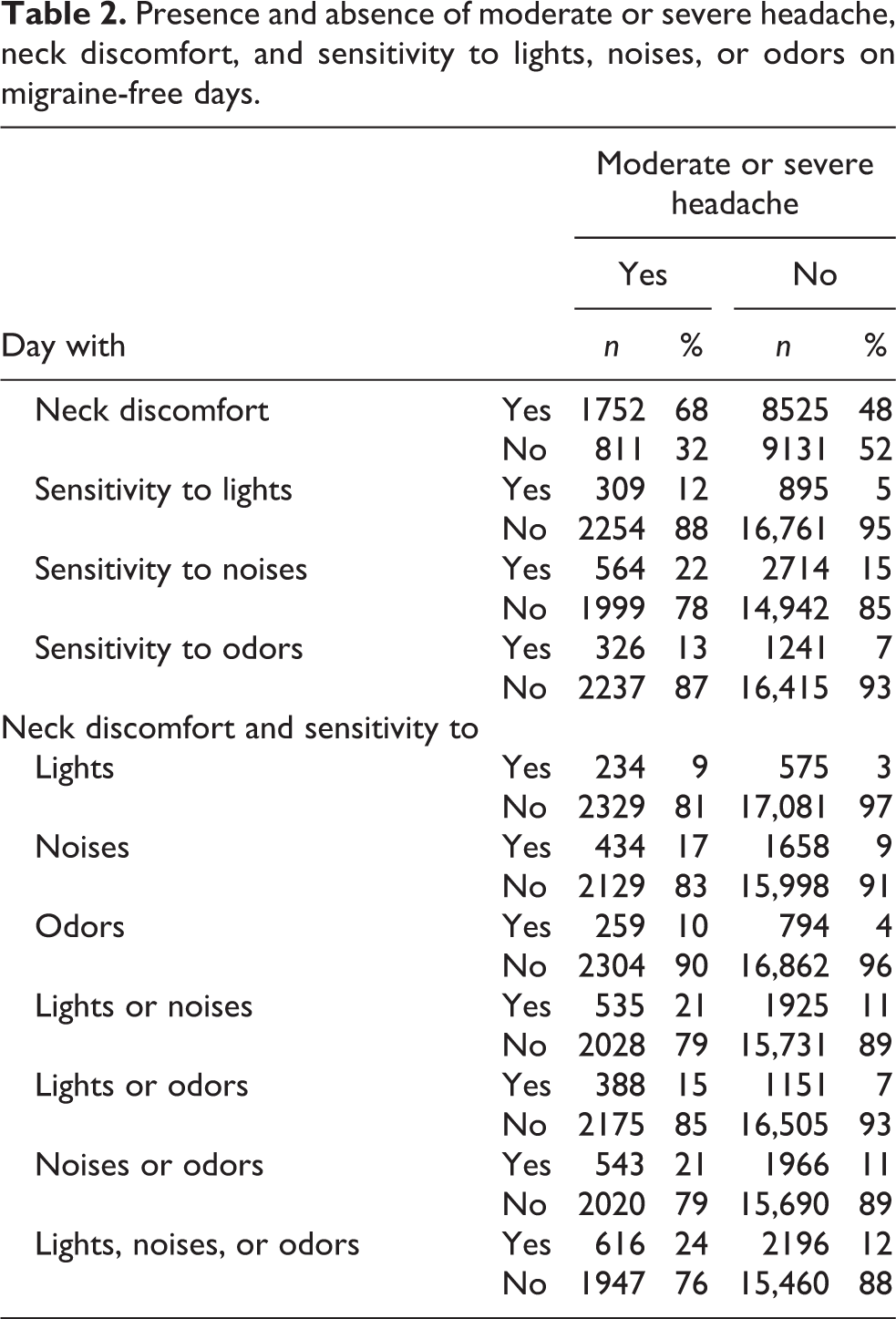
The relation of headache and premonitory symptoms is given in Table 2. Neck discomfort was found on 68% of the days with moderate or severe headaches and on 48% of the days with mild or no headaches. The prevalence of sensitivity to lights, noises, or odors alone or associated with neck discomfort ranged from 9% to 24% when the headache was moderate or severe and from 3% to 15% when the headache was mild or absent.
Presence and absence of moderate or severe headache, neck discomfort, and sensitivity to lights, noises, or odors on migraine-free days.
Regarding acute medication, non-opioid analgesics, combination analgesics, and triptans were used most frequently, and expectedly, use was much more common on days with moderate or severe headache than on days with mild or no headache (Table 3). Table 4 presents the intake of acute medication on days with the presence and absence of headache and certain premonitory symptoms. The proportion of days with acute medication was 67% with moderate or severe headache, 34% with mild headache, 19% with neck discomfort, and 18–24% with sensitivity to lights, noises, or odors. In the case of neck discomfort associated with sensitivity to lights, noises, or odors, acute medication was used on 21–26% of the days.
Use of acute medication on migraine-free days in 271 patients with migraine.a

a The proportion of days with use of acute medication and the proportion of patients who used a specific medication on at least one day of the observation period is listed.
Use and nonuse of acute medication in the presence and absence of headache, neck discomfort, and sensitivity to lights, noises, or odors on migraine-free days.

As given in Table 5, the presence of neck discomfort and sensitivity to lights, noises, and odors increased the risk for migraine statistically significant by 20–40%. In contrast, this risk was statistically significantly decreased by moderate to severe headache. This finding can be explained by the fact that moderate or severe headache was frequently associated with the use of acute medication (see Table 4).
Risk for developing migraine on the subsequent day in the presence of moderate or severe headache, neck discomfort, and sensitivity to lights, noises, or odors on migraine-free days.a
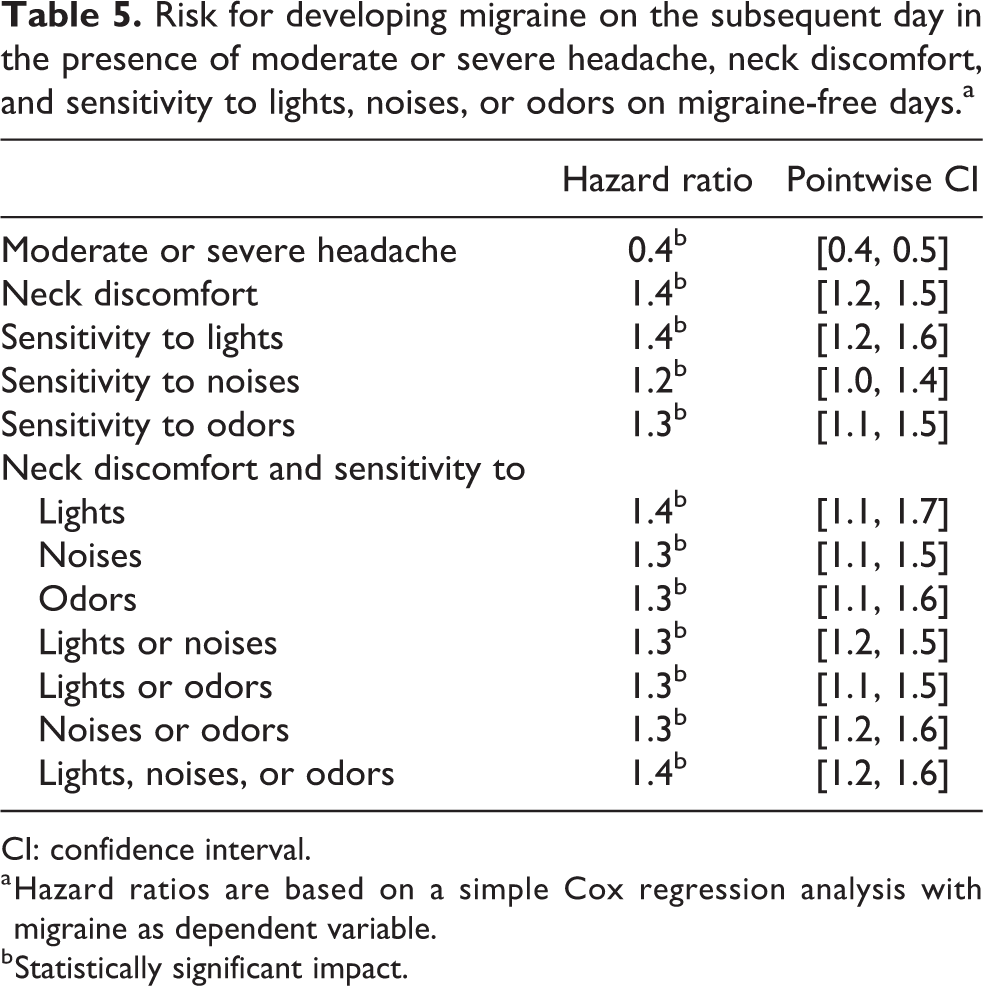
CI: confidence interval.
a Hazard ratios are based on a simple Cox regression analysis with migraine as dependent variable.
b Statistically significant impact.
Our final analysis, summarized in Table 6, provides adjusted treatment effects from a Cox regression analysis with moderate or severe headache (which was the dominating confounder) and a weighted Cox regression analysis, the marginal structural model which accounts for more potentially confounding variables as described in the section ‘Statistical analysis’. The use of acute medication on a day with neck discomfort or on a day with sensitivity to lights, noises, or odors reduced the risk of a migraine attack on the subsequent day by 30–70% in the marginal structural model and by 10–60% in the Cox regression analysis adjusted for moderate or severe headache (Table 6). Using acute medication in the presence of neck discomfort associated with sensitivity to sensory stimuli reduced the risk by 60–80% and by 40–80%, respectively. Analyzing single symptoms, only sensitivity to odors showed a statistically significant reduction in both models. Analyzing neck discomfort associated with sensory sensitivity, the risk was reduced statistically significantly for all constellations in both models, however.
Use of acute medication in the presence of neck discomfort and sensitivity to lights, noises, or odors on migraine-free days.a
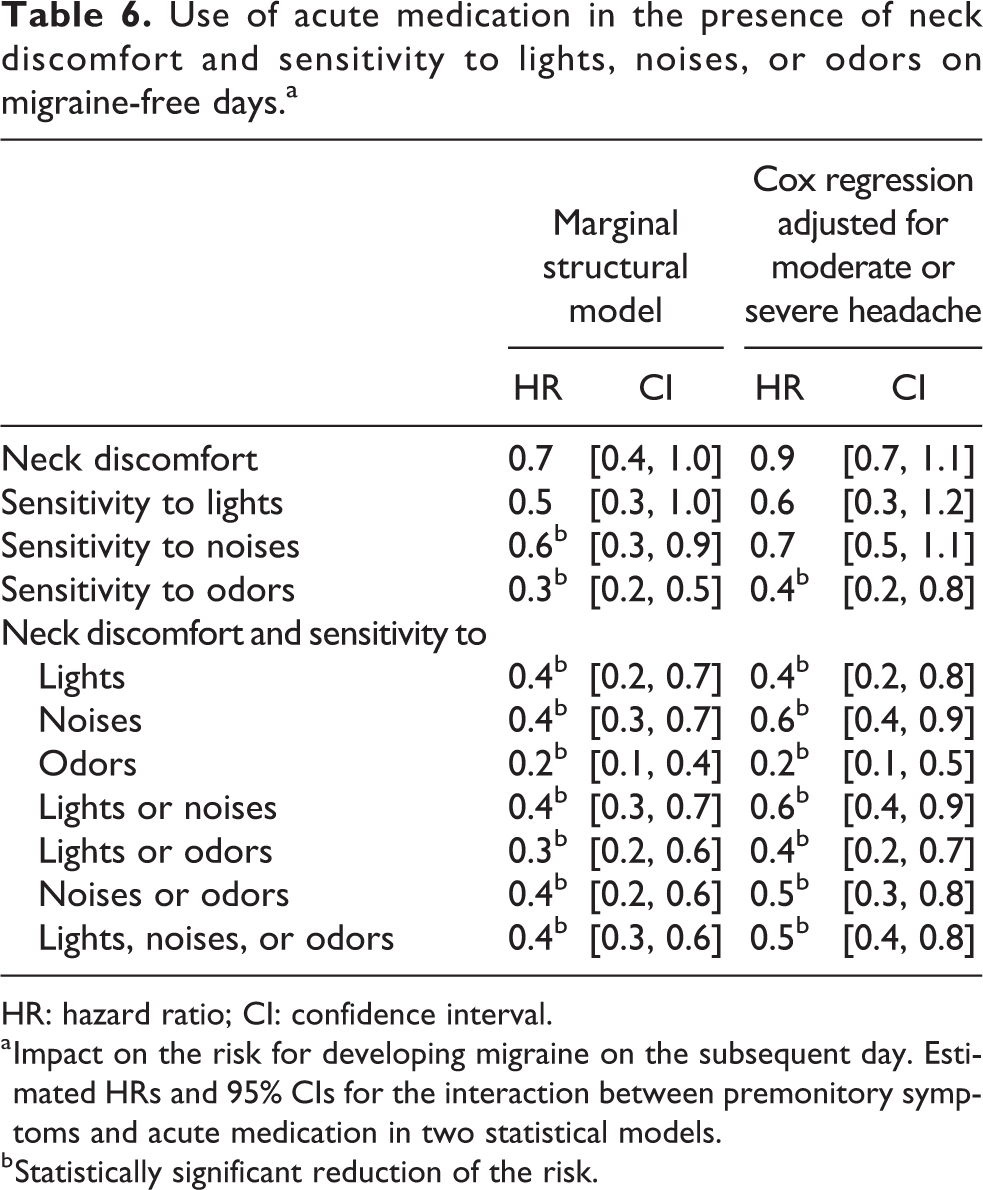
HR: hazard ratio; CI: confidence interval.
a Impact on the risk for developing migraine on the subsequent day. Estimated HRs and 95% CIs for the interaction between premonitory symptoms and acute medication in two statistical models.
b Statistically significant reduction of the risk.
The complementary analysis of headache-free days (results in supplementary material) revealed the following findings. Neck discomfort was present on 49% of the days in 97% of patients. The corresponding figures for sensitivity to lights, noises, or odors ranged between 6–16% and 59–84%, and neck discomfort associated with sensitivity to sensory stimuli occurred on 4–13% of the days and in 49–79% of the patients. Any acute medication was used on 2374 (13%) of the days by 90% of the patients on at least one day of the observation period. Non-opioid analgesics (7% of the days, 74% of the patients), combination analgesics (3% and 39%), and triptans (2% and 26%) were most popular. Use of acute medication on days with at least one of the premonitory symptoms ranged between 16% (days with sensitivity to noises) and 25% (days with neck discomfort associated with sensitivity to lights). Neck discomfort and sensitivity to sensory stimuli increased the risk for headache on the subsequent day by only 10–20% and the increase was statistically significant only for neck discomfort and constellations including neck discomfort and sensitivity to noises (p-value 0.03). Using acute medication on a day with neck discomfort and/or sensory sensitivity reduced the risk of a forthcoming headache for all constellations statistically significantly by 70–80% in the marginal structural model and by 70–90% in the Cox regression analysis.
Discussion
This analysis was based on data from a large prospective cohort of patients with episodic migraine. The analysis included exclusively days without migraine and aimed at assessing neck discomfort, sensitivity to lights, noises, or odors, and use of acute medication. The prevalence of neck discomfort was 51% that of sensitivity to lights, noises, or odors that ranged between 6% and 16% and co-occurrence of neck discomfort and sensitivity to sensory stimuli was found on 4–14% of the diary days. The majority of patients recorded at least one day with one of these symptoms alone or jointly. As expected, neck discomfort and sensitivity to sensory stimuli were more common on days with moderate or severe headache but still present on days with mild or no headache. Similarly, acute medication was used as expected, both with respect to the type of medication (non-opioid analgesics, combination analgesics, triptans) and with respect to the circumstances (moderate or severe headache).
The risk of a migraine attack, that is, occurrence of a headache fulfilling ICHD-2 criteria of definite or probable migraine without aura on the subsequent day, increased in the presence of neck discomfort and sensitivity to lights, noises, or odors, whereas the risk decreased when acute medication was taken on a day with such symptoms. In the model adjusted for moderate or severe headache, the benefit of medication was larger in the presence of both neck discomfort and sensitivity to sensory stimuli than in the presence of only one of these symptoms suggesting that the co-occurrence of neck discomfort and sensitivity to lights, noises, or odors is a more reliable indicator of using acute medication.
We want to point out, however, that there might be other premonitory symptoms which are more reliable indicators for using acute medication. In addition, our analysis was population-based and did not consider that premonitory symptoms are highly individual. 11
Accordingly, further research is necessary for elucidating key symptoms indicating the successful use of acute medication during the premonitory phase of a migraine.
The analyses of the headache-free intervals showed that neck discomfort and sensitivity to sensory stimuli as well as the use of acute medication are not uncommon on days without headache in patients with migraine. As expected, the presence of any of the premonitory symptoms increased the risk of headache on the subsequent day much less than the risk of migraine. In contrast, the reduction of the risk of a forthcoming headache was more pronounced when acute medication was used in the presence of neck discomfort or sensitivity to sensory stimuli on a headache-free day compared to the findings for migraine-free days.
In the patients’ assessment as well as in daily medical practice, premonitory symptoms such as neck discomfort and sensitivity to lights, noises, or odors may be mistaken as triggers. 9,11,22 Karsan and Goadsby 9 pointed out that neck discomfort is experienced early in the premonitory phase of a migraine attack. Neck pain preceding the onset of migraine headache may be explained by early activation of the trigemino-cervical complex (TCC). The authors explain that the TCC is modulated by descending input from regions pivotal to the pathophysiology of migraine, that is, the periaqueductal gray, locus coeruleus, and hypothalamus involving neurotransmitters such as 5-HT1B/1D, calcitonin gene-related or others targeted by compounds used for treating acute migraine attacks. 9 The findings of the present analysis support this hypothesis, as neck discomfort was highly prevalent on migraine-free days and increased the risk for a migraine attack on the subsequent day. However, our findings also suggest that neck discomfort alone may not be a reliable indicator for using acute medication in the premonitory phase. Functional neuroimaging and neurophysiological studies showed that processing of sensory stimuli differs in the pre-ictal and inter-ictal periods of migraine attacks. 6,23,24
In a functional magnetic resonance imaging (fMRI) study, trigeminal nociceptive stimulation induced higher activity within the trigeminal nucleus caudalis in the pre-ictal than in the inter-ictal period and the height of the response allowed to predict the next attack. 23 Schulte and May reported a patient with migraine who underwent daily fMRI and daily assessment of sensory stimuli over a period of 30 days. The unpleasantness of ammonia rose odor and a rotating checkerboard rated on a visual numeric rating started to increase and hypothalamic activity as a response to trigeminal nociceptive stimulation was altered on the day before the onset of migraine headache. 24
Recommending acute interventions in the premonitory phase requires a reliable prediction of a forthcoming migraine attack. Analyses of the same data set (n = 1) as used in this study suggest that both premonitory symptoms and trigger factors are highly individual. 11 A 3-month prospective electronic diary study in 76 patients revealed correct prediction of a migraine attack in 72% of the occasions rated by the patients as premonitory symptoms. 13 In another study including 34 patients who recorded 229 migraine attacks, 69% of the attacks were preceded by premonitory symptoms. Two-thirds of the patients were able to predict at least one attack, one-third correctly predicted more than 50% of the attacks, and one-third of the patients erroneously reported premonitory symptoms. 25 Different presentation of the data prohibits a comparison of the two studies.
The use of acute medication in the premonitory phases was examined in two small studies, suggesting that this approach might be useful. 26,27 A study on naratriptan was completed by 20 patients who recorded details of premonitory symptoms as well as headache onset at baseline and thereafter were instructed to use naratriptan at the time when they knew that headache was inevitable. During baseline, all of 59 premonitory periods were followed by headache, whereas in the treatment period headache remained absent after 38 of 63 premonitory periods, that is, in 60%. 26 Another study included 76 patients with migraine to compare the use of frovatriptan in the premonitory period with daily use of topiramate. At baseline, the patients had to demonstrate that they were able to predict at least 50% of the migraine attacks during the premonitory phase. Fifty-five patients were randomized and 44 patients completed the study. The treatment period lasted 2 months. Both groups showed a decline in headache days. In terms of efficacy, topiramate was superior to frovatriptan, whereas in terms of tolerability, frovatriptan was superior to topiramate. 27 Even though the two studies do not allow reliable conclusions, they were a first – symptom-based – step toward early therapeutic intervention in migraine attacks. The present analyses provide additional information supporting this approach.
Another approach was chosen by Martins and co-workers performing a proof-of-concept study for detecting neurophysiological changes preceding a migraine attack by means of a portable device. 28
Although the findings of this study support early use of acute medication during the premonitory phase of a migraine attack, specifically in the presence of both neck discomfort and sensitivity to lights, noises, or odors, we refrain from any treatment recommendation at this stage. Further studies should be carried out to provide more insights in the use of acute medication in the early phase of a migraine attack.
Strengths and limitations
In this study, statistical analysis was based on a large data set from a prospective diary study including a population-based convenient sample of 271 patients with episodic migraine who kept a comprehensive daily diary covering a wide spectrum of factors possibly associated with migraine attacks. In this article, we used the data to investigate the use of acute medication in the premonitory phase of a migraine attack focusing on the co-occurrence of neck discomfort and sensitivity to sensory stimuli.
Whenever a treatment is not assigned randomly as in the case of observational studies, confounding needs to be accounted in order to achieve an unbiased estimation of treatment effect. Marginal structural models are powerful statistical methods, which allow for controlling for the effect of time-dependent confounding, while being affected by the previous treatment. Dealing with such longitudinal data patterns, appropriate estimation of the relationship between treatment and outcome is not possible via standard regression methods. 18
The main strength of marginal structural models is that they do not suffer from collider stratification bias, as the statistical method is based on weighting for controlling time-varying confounders and not on conditioning. 29
However, marginal structural models, as all causal models, can only achieve balance on known factors in contrast with an ideal situation with randomized clinical trials where variation and unknown confounders are balanced. This study is also limited by the fact that the results are based on re-analysis of historic data that the study initially was not designed to assess therapeutic strategies and the all types of acute medication were summarized in one single variable.
Furthermore, a bias arising from the patients’ decision when to use acute medication cannot be excluded. Indeed some patients carefully observing the evolution of a migraine attack may take acute medication as soon as they experience certain non-headache symptoms. However, our procedure based on modeling acute medication use was chosen to minimize the impact of such bias.
Even though we used a sophisticated and powerful statistical method like the causal marginal structural model, some concerns about the bias, involved in the estimation of the treatment effect, still remain, as the complex relationship between the outcome and the treatment might be distorted due to unmeasured confounding within the design of the data. This is hard to completely avoid, while dealing with longitudinal observational data, but we are also conscious of the fact that, within such patterns, the marginal structural model represents an optimal strategy in dealing with time-dependent confounding, enhancing treatment comparability, and estimate causal effects. Such innovative causal methods should be preferred to conventional statistical methods such as Cox regression, random-effects model, and generalized equation estimation, as the standard approaches may be impaired by selection bias and over-adjustment bias. The former occurs by adjusting for a time-varying confounder that may share a common cause with the outcome; the latter occurs by blocking the effect of past treatment on outcome, by adjusting for an intermediate variable affected by past exposure.
In marginal structural models, weighting plays a crucial role in dealing with confounding. Indeed, each patient receives a weight inversely proportional to the estimated probability of having her or his own observed treatment history. This approach corrects for the non-random assignment of acute medication by up-weighting patients whose treatment and covariates histories are underrepresented compared to what would have been observed if the treatment had been randomized. It turns out that this analytical causal tool, provided that all their assumptions are met, replicates results of randomized controlled trials. For instance in HIV, the findings of studies applying a marginal structural model were close to the ones of randomized controlled trials. 30,31 Nevertheless, randomized controlled trials are the gold standard for proving the efficacy and the safety of an experimental drug, as randomization renders the treatment groups comparable by balancing both observed and unobserved confounding factors. Accounting for all of that, we still believe that the marginal structural model represents a fundamental tool in longitudinal observational data and provides an acceptable approximation of the ideal design. Such analyses have at least the potential to provide strong hypotheses that are worth being followed-up in more expensive controlled clinical trials.
Conclusion
Migraine attacks may be prevented when acute medication is used in co-occurrence of neck discomfort, that is, a very common premonitory symptom, and sensitivity to lights, noises, or odors, that is, premonitory symptoms which are very specific to migraine. The results of this study may stimulate further prospective trials.
Clinical implications
This re-analysis of data from a large prospective diary, by means of the marginal structural model, supports the usefulness of treating migraine during the premonitory period.
The marginal structural model stands out, due to its controlling for the effect of confounding variables that change over time and ensuring unbiased treatment effect estimators.
Ingestion of acute medication in the presence of neck discomfort associated with sensitivity to lights, noises, or odors during migraine-free days showed a statistically significant and clinically relevant decrease in the risk of a migraine attack on the forthcoming day.
Further studies aiming to identify reliable premonitory symptoms which enable early therapeutic intervention and controlled studies of such interventions (non-pharmacological or pharmacological) appear to be a promising approach for improving the management of migraine attacks.
Supplemental Material
Supplemental Material, Di_Termini_Tables_all_Headaches - Early use of acute medication for preventing migraine attacks: Results from a diary-based cohort study
Supplemental Material, Di_Termini_Tables_all_Headaches for Early use of acute medication for preventing migraine attacks: Results from a diary-based cohort study by Susanna Di Termini, Christian Wöber and Werner Brannath in Cephalalgia Reports
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Grant TE 1181/1-1 of the German Research Foundation (DFG) to SDT.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.