
Abstract
The Act when Mild (AwM) Study has illustrated the benefits to migraineurs of taking triptan medication when their migraine pain is still mild and within 1 h of the onset of symptoms. Yet many patients wait until the attack has fully developed before taking their medication, with potentially inferior outcomes. In order to reproduce the benefits of early intervention using the AwM paradigm in daily practice, a number of key barriers need to be addressed at both the physician and patient level. Notable physician-related barriers to be overcome, particularly at the primary care level, include accuracy of an early diagnosis of migraine in newly presenting patients, communication skills that generate a therapeutic engagement with migraine patients and enhance patient confidence, the application of knowledge about up-to-date strategies to optimize treatment outcomes, and the setting of achievable goals to avoid unrealistic expectations. Patient-related obstacles that need to be identified and overcome encompass patient attitude, expectations, and behaviour. Migraine patients may be reluctant to consult their physician, and, of those who do, many stop consulting because they perceive that physicians can do little to improve their situation. For this reason, migraine patients need to be counselled about the most appropriate medication for their level of symptoms. Moreover, patients need to be confident before they will adhere routinely to the advice they receive, and high in the priority of advice is the use of medication, particularly triptans, at the first sign of a migraine attack, rather than waiting until their attack has progressed to moderate or severe intensity. Patients who adhere to this advice are likely to experience a notable reduction in the pain, disability and time lost that they would otherwise suffer. The beneficial effects of early triptan intervention illustrated in the AwM Study can therefore be best reproduced in the clinic if the correct advice given to patients is not only accepted and applied by them, but also followed up by their physician.
Introduction
Understanding the needs of migraine patients is crucial to tailoring treatment that not only achieves the best possible outcome based on their presenting pattern of symptoms, but also meets their expectations and, thus, results in patient satisfaction. Historical goals of treatment—to relieve moderate to severe migraine pain—have evolved to a higher level of sophistication, based on treatment attributes that are known to be most sought by patients. These encompass speed of onset of pain relief, rapid freedom from pain, rapid restoration of normal daily functioning, reduced risk of recurrence and absence of side-effects (1). These goals form the current benchmark against which the efficacy and effectiveness of migraine treatments are measured, most notably in clinical trials. The ‘Act when Mild’ (AwM) Study has provided robust evidence and supports a large body of emerging evidence suggesting that the early administration of acute migraine therapy, while pain is still mild, increases the likelihood of achieving these goals (1, 2). This evidence base provided the basis for the American Academy of Neurology's recent Acute Migraine Treatment Practice Parameter recommendation that treatment early in the course of an attack is a strategy that improves outcomes, is cost effective and reduces the use of rescue medication, side-effects and the potential for medication overuse headache (3). The challenge is to apply the AwM approach outside the confines of a clinical trial so that patients can benefit from improved outcomes in a naturalistic setting. This review considers how this challenge may be met.
Identifying and overcoming challenges to early treatment with triptans
A matrix of issues influence the goal of enabling migraine patients to gain the most from triptan therapy through optimal timing of medication intake in relation to the start of a migraine attack. This matrix encompasses the behaviour, knowledge and communication skills of the physician, the patient and the healthcare payer. Each component of this matrix is a possible independent obstacle to achieving this goal. Collectively they can pose potentially formidable challenges that need to be addressed to reach the goal of achieving early triptan treatment benefits in individual migraine patients in a routine day-to-day environment. These challenges and their potential solutions will be considered here, from both the physician's and patient's viewpoint.
Physician-related challenges
Most migraine patients first seek assistance for headache from their primary care physician (PCP). This first contact by migraine patients is crucial to their future outcome, and PCPs as well as tertiary care physicians (e.g. office- and hospital-based specialists) need to remain vigilant about the importance of an expedient diagnosis, tailoring treatment options to patients' needs and setting realistic treatment goals relative to patient expectations.
Diagnosis
The initial diagnosis of migraine, usually made by the PCP, is often constrained by the high prevalence of tension-type headache in the population and the overlap in clinical features and triggers of these two primary headache disorders. About half of migraineurs in the USA have not been diagnosed with migraine, and the most common misdiagnoses are sinus and tension-type headache, often resulting in suboptimal treatment (4). The use of quick and simple screening tools (5, 6) (Fig. 1) can improve the accuracy of diagnosis and increase the probability of a more expedient diagnosis of migraine and initiation of appropriate treatment.

Treatment approach
Following diagnosis, medication options for migraine include migraine non-specific treatments, such as simple analgesics, non-steroidal anti-inflammatory drugs (NSAIDs) and medications more specific to migraine, including ergot derivatives and triptans. All are proven effective interventions for migraine, but their relative clinical utility in a given patient is influenced not only by the severity of migraine pain at the time of medication intake, but also their hierarchical use throughout the course of the illness. The traditional step-care approach is based on an empirically sound rationale, i.e. to start with simple non-specific analgesic monotherapy and progress through hierarchical layers of options sequentially, using a trial-and-error approach, until an optimal solution is found. However, as the step-care approach is essentially a ‘one-size-fits-all’ paradigm, it does have some important limitations. Although some migraine patients may be well controlled on non-specific monotherapy, a proportion will not, requiring them to progress to the next step in the treatment hierarchy. An inadequate response at any stage may urge patients to disengage from consulting their physician in favour of seeking their own solution, so that a proportion of triptan candidates never reach the triptan stage in the step-care paradigm. Indeed, in spite of high patient satisfaction with triptans relative to other interventions (7, 8), triptans remain underused (9, 10). Moreover, in those who do reach the triptan stage through step care, their journey to this point potentially prolongs the time to achieving this as their best solution.
An alternative approach, the stratified-care approach, considers the needs of each patient individually, based on their presenting symptoms at the time of consultation. Using the severity and frequency of migraine attacks together with the level of disability caused, the presence of associated symptoms, and the time to the peak of the attack, each elicited at consultation, the most appropriate treatment option can be selected on a ‘menu’ basis predicated on a match between the illness profile and therapeutic profile of the medication. In this way, a prolonged sequential trial-and-error period can be avoided and triptan candidates can be identified and treated more expediently than with the step-care approach. Moreover, this approach is not only more likely to enhance patient confidence, but also allows patients to select from a menu of options according to their own perceived needs, encouraging their compliance with treatment instructions. The potential limitation of this approach arises from the risk of medication overuse, when more than one option is prescribed at the same time. This emphasizes the need for an effective therapeutic alliance between the physician and the patient, including regular follow-up, based on a mutually high level of communication. In these circumstances, influencing patient behaviour, ultimately in relation to the timing of intake of their medication following the AwM paradigm (i.e. when pain is still mild and within 1 h of migraine onset), is likely to be less challenging.
Addressing patient expectations
Optimal treatment of migraine is a function of patient expectations based on several target outcomes. Although most patients seek pain relief, this is an imprecise end-point in terms of measuring treatment outcome. A commonly used end-point in clinical trials is freedom from pain at 2 h after dosing (2 h PF), a robust definitive end-point that is also amenable for use in a routine clinical practice setting. Outcome measures have evolved further to overcome the main limitation of the 2 h PF end-point; that is, to measure how long 2 h PF can be sustained. Sustained freedom from pain (SPF) requires achievement of 2 h PF without recurrence or use of additional migraine-related medication for a defined time period, often 24 h post dose. In deciding on a target end-point for an individual patient, realistic expectations need to be considered in line with the increasing challenges to achieve the more discerning outcomes; achievement of pain relief at 2 h is less challenging than 2 h PF and both are less challenging than SPF. The end-point that presents the greatest challenge is a composite of SPF plus the absence of adverse events (AEs) [sustained pain free and no AEs (SNAE)], an outcome that appears to discriminate between triptans (11).
Targeting end-points in a real-life setting is likely to enable both the physician and patient to achieve an outcome that is tailored realistically to individual patient expectations (Fig. 2). Put another way, targeting end-points that encompass realistically unachievable outcomes, at least in the first instance, can raise patient expectations beyond reality. However, patients who achieve a realistic target outcome are more likely to engage with, and accept advice from their physician to enable further improvement, including the potential need to use acute treatment sooner in the course of the attack than they are otherwise accustomed.
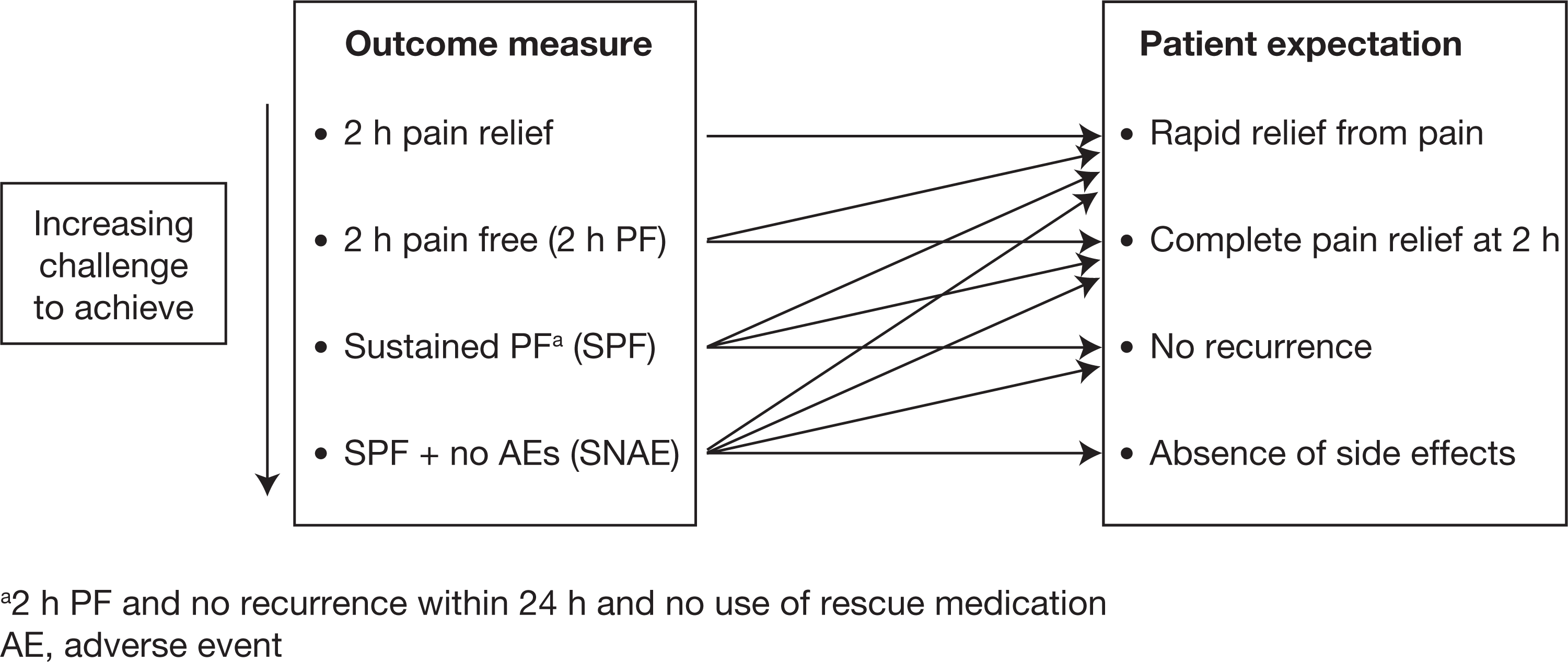
Ability of different outcome measures in migraine to meet patient expectations.
Overcoming patient-related barriers to early treatment with triptans
Patients and not physicians are, of course, the best judges of what works best for them when treating a migraine episode. However, fixed views by patients based on real or perceived expectations can lead, understandably, to a reluctance and even intransigence to accept further advice from their physicians. Such views are apparent from surveys about consultation rates with, and patient confidence in, their physician, patient attitudes to migraine and their perceptions about treatment. Moreover, in establishing the AwM paradigm, the presence of an appropriate window of opportunity needs to be established based on the variable pattern of migraine attacks within and across individual patients.
Consultation rates as a measure of patient confidence?
Up to one-third of migraine patients have never consulted a physician about their migraine (1), indicating that a substantial minority appear to manage their illness without physician intervention. The reasons for this are open to speculation and are beyond the scope of this overview. Of more concern, perhaps, is that of those who have sought physician consultation, a high proportion do not follow up for further consultation (Table 1a) (1). The reasons that drive these patients to disengage with their physician are varied, but are likely to include a proportion who, by virtue of treatment failure during their step-care management have chosen to seek their own solutions. This is reflected in surveys conducted in different countries that canvassed the level of confidence migraine patients have in the ability of physicians to manage their migraine (Table 1b) (1). Clearly, ways to increase consultation rates and enhance patient confidence are a target for improvement (12), as both have implications in the context of a physician's opportunity to modify patient behaviour consistent with the AwM paradigm.
Patient consultation rates with, and their confidence in, physicians. Targets for improvement?

Data from UK, USA and France.
Data from patient surveys in UK, USA and Sweden.
Patient attitude to migraine and perceptions about treatment
Barriers to early treatment in migraine can be exacerbated by a number of other patient-related factors. One of these revolves around the ability of patients to distinguish between migraine and non-migraine headaches. Indeed, the most frequent reason why patients delay medication intake, notably with triptans, is their perceived need to wait to see if the headache develops into a migraine attack (13, 14). However, recent evidence indicates that experienced migraineurs can usually self-identify a migraine attack at onset. In a study to measure the accuracy of migraineurs' ability to identify their headaches as migraine at the time of onset of head pain, 182 migraineurs at 14 headache clinics in the USA were asked to record their headache episodes over a 30-day period and to classify them into migraine and non-migraine attacks at the first sign of onset (15). Of 1197 attacks reported, 309 (26%) were classified as non-migraine headaches and 888 (74%) as migraine attacks at onset. At the time of headache peak, 92% of headaches classified as migraine at onset were indeed migraine headache.
A related patient barrier to early treatment with triptans is their perceived need to delay treatment intake until they are sure that the migraine will progress beyond a mild intensity (13, 14). In fact, most migraine headaches progress to at least moderate–severe intensity (16). In order to examine whether this perception is consistent with reality in individual patients, the physician should seek the patient's history by consultation, to illustrate this point with a view to overcoming this perceived barrier.
Fear of side-effects, risk of medication overuse and availability of sufficient medication supplies—notably of triptans centred on cost—are issues that need to be addressed through effective physician–patient communication. Choice of medication with the most favourable tolerability profile will address the former. Risk of medication overuse, discussed earlier, can be minimized by effectively aborting the attack as early as possible using the AwM paradigm, which can potentially minimize cost in terms of fewer pills consumed, less time lost and reduced medical resource utilization (17).
Identifying a window of opportunity
The AwM paradigm is predicated on a window of opportunity for patients to take medication within 1 h of migraine onset and before pain has progressed to moderate–severe intensity. However, the ‘window of opportunity’ is not a constant across and within all migraine patients. For example, in a cohort of 253 migraine patients, moderate–severe pain was present at the time of onset of the attack in 11% of patients with aura and 19% without aura, whereas pain progressed to moderate–severe intensity within 1 h of migraine onset (range 11–60 min) in 48% and 60% of patients with and without aura, respectively. Pain reached moderate–severe intensity after 1 h (range 61 to > 120 min) in 21% and 42% of patients with and without aura, respectively (18), indicating that in a substantial proportion of patients whose migraine occurs during waking hours, a window of opportunity exists although in some it may be quire short. However, in patients who experience attacks upon awakening, the percentage of attacks that may be treatable while pain is mild may be less than half. This was demonstrated in a recent study in which patients were asked to treat their migraine when pain was mild and within 1 h of onset. In that study, in approximately 30% of 14,000 attacks, moderate–severe pain was already present on waking, and in 20% the attack progressed with sufficient rapidity that moderate–severe pain was established before medication could be taken (19). These findings reinforce the need not only to establish the existence of a window of opportunity, but also to determine the presence and percentage of attacks that occur upon awakening or awaken the patient from sleep, and develop strategies to effectively manage these particular attacks.
Illustrative real-life case profiles
To illustrate the barriers to early treatment presented above and other potential barriers that are consistent with the AwM paradigm, two distinct real-life case profiles are presented here, together with their potential solutions.
Case profile 1
A 48-year-old woman with a 25-year history of migraine suffered frequent migraine attacks both during waking (daytime) and sleeping (night-time) hours. Approximately 15–20% of migraine attacks occurred during the day and would start with neck discomfort. This, the patient had learned, was the signal to take her prescribed triptan medication, after which the patient would be pain free in approximately 30 min. If this patient did not take medication within 1 h of the start of neck discomfort, the triptan ameliorated some of the pain, but residual pain would remain for the following 12 h. Moreover, the patient clearly identified that beyond this time it was too late for medication to prevent nausea and vomiting and, in this scenario, she sought bed rest as the only feasible treatment option. Furthermore, most of this patient's migraine attacks occurred during normal sleep. These attacks were of sufficient severity to cause waking in the early hours of the morning, when she would take a triptan dose immediately, return to bed and wake up several hours later usually pain free.
Clinical commentary on case profile 1
For this patient, early intake of triptan medication at the first sign of a migraine episode meant the difference between avoiding severe pain plus achieving complete relief within 30 min, and the presence of moderate or severe pain lasting several hours. In waking episodes, the window of opportunity to abort migraine attacks effectively with triptan therapy was around 1 h. This patient was able to identify premonitory symptoms that reliably predicted the impending onset of a migraine episode, so that if a triptan was taken during the premonitory time, complete and rapid relief was achieved. The major challenge in this patient was that most of her migraine attacks started during sleep, when premonitory symptoms were unable to signal the patient to take medication. The consequence was that the attack evolved into a severe headache that awoke the patient. The solution for this patient was prophylactic therapy that not only reduced the severity of nocturnal headache, but also lengthened the window of opportunity to allow rapid relief with a triptan.
Case profile 2
A 58-year-old man with a > 40-year history of frequent migraine attacks was able to reduce the frequency of acute attacks by approximately 30% using prophylactic medication. However, he still experienced 7–12 migraine headaches per month. Apart from the headaches present on waking, most started with mild pain that would progress relentlessly to moderate–severe intensity without treatment. When pain was still mild, massage was effective in ameliorating about one in five attacks, although it was not possible to predict which headaches would go away and which would progress to greater intensity with this approach. The patient had been prescribed oral triptan therapy for acute attacks, which was effective provided that it was taken early after onset when pain was still mild. In this scenario, he would be aware of therapeutic benefits within 30–60 min, whereas if medication intake was delayed the therapeutic benefit was substantially lower. When asked why he did not take triptan medication early for all his attacks, the patient revealed that this was because he had an insufficient quantity of tablets to treat all his migraine attacks because of healthcare provider restrictions on the reimbursement of this type of medication. To conserve triptan supplies, the patient used massage as described above and/or non-specific over-the-counter medication with little benefit. In this triptan-experienced patient, fear of side-effects was not a driver of delayed triptan intake; the major obstacle to early treatment was the limited supply of triptan medication.
Clinical commentary on case profile 2
This patient had a long history of debilitating migraine attacks, and preventative therapy was now optimized. In spite of a remaining attack frequency of 7–12 migraines per month, this was, in fact, the best the patient had been in > 20 years. Clearly, early treatment with triptan medication makes a significant difference for this patient when the window of opportunity presents to take medication early and while migraine pain is still mild. This patient, however, receives only six triptan tablets per month and two triptan injections every 3 months, necessitating him to conserve supplies. This is a common dilemma faced by migraineurs: in a survey of 233 migraine sufferers, 80% of respondents considered triptans to be the most effective acute treatment for migraine, although only 47% of patients with insurance limitations took triptans at the first sign of pain, compared with 79% who had no insurance restrictions (20). Moreover, 42% reported an inadequate supply of triptans due to such insurance limitations. This scenario is representative of the present case profile, because the inadequate supply, as opposed to an unrestricted supply, resulted in meaningful reductions in quality of life. This consequence is illustrated in another survey in which 249 migraineurs were asked if a triptan was the first medication they take for a migraine attack (21). Responses to the survey were categorized into ‘always’ (41% of patients), ‘sometimes’ (45%) or ‘never’ (14%). Patients in each category were asked a further series of questions, the responses to which not only revealed some important behavioural and attitudinal differences, but also showed quality-of-life benefits in patients who took triptans earlier in the hierarchy of available treatments (Table 2) (21).
How the order of use of triptans reflects migraineurs' quality of life. Reproduced with kind permission (21)

Available at http://www.headachetest.com/HIT6/PDFS/English/pdf
The solution for this present patient's dilemma encompasses the use of prescribed non-triptan therapy (NSAIDs or dihydroergotamine) early in the course of attack, together with massage, after the triptan supply is exhausted, or the prescription of an additional triptan—while ensuring that one triptan is never taken within 24 h of another triptan or dihydroergotamine—on the basis that some insurance carriers will cover the use of more than one triptan.
Summary and conclusions
The AwM Study adds to an emerging body of evidence that early treatment with triptans, while pain is still mild and within 1 h of the onset of migraine symptoms, provides significantly better outcomes than waiting until the migraine attack has fully developed. Achieving these benefits in the clinic, outside the highly controlled environment of a clinical trial, is contingent upon several patient and physician variables that encompass the knowledge, attitude, communication skills and behaviour of both parties. The next challenge is to identify patients in whom the AwM strategy is necessary, as up to 30% of patients may still achieve a pain-free response within 2 h even when the pretreatment pain intensity is moderate or severe. In those for whom treatment while pain is still mild is important for achieving the best outcomes, there are several factors that may still confound this approach: lack of a window of opportunity (including development of a migraine attack during sleep and rapid progression before the triptan can be taken); failure to recognize premonitory symptoms; and reserving the ‘most potent’ drug for the most severe attacks (driven by fear of side-effects and/or limited availability of supply). It is, however, crucial that such factors are identified in order to apply tailor-made solutions that can minimize the lower quality of life and higher disability that occur as a result of late or delayed triptan intake. To achieve this, physicians and patients need to identify the individual need for treating early while pain is still mild, the patient's ability to distinguish between migraine and non-migraine headaches and between migraine attacks that are likely to respond to non-triptan therapy or to progress, the diurnal distribution of attacks, and the duration of the window of opportunity to treat using the AwM paradigm. By exploring these parameters and developing approaches based on the AwM paradigm that accommodate the variability between migraine sufferers in the clinic, patients are more likely to gain optimal benefit from triptan therapy, resulting in reduction of their level and duration of suffering.
Footnotes
Competing interests
D.W.D. has received consultancy fees from Allergan, GlaxoSmithKline, Merck, OrthoMcNeil, Neuralieve, Pfizer, Addex, Endo, St Jude, Coherex and HS Lundberg and has received research grants from ANS and Medtronic.
Acknowledgements
The author would like to thank Stuart Donovan PhD, from Complete Medical Communications, who provided medical writing support funded by Almirall.