
Abstract
This prospective, multi-center, observational study aimed to examine patients' early treatment decision process. Specifically, we assessed if the association between mild headache pain at treatment initiation and early treatment differed by the speed of headache escalation. Patients (n = 168) were instructed to collect information on their headache experience during the study period via an electronic diary over 30 consecutive days after enrollment. At the time of treatment, patients who treated early were 2.3 times as likely to experience mild headache pain as those who treated late. Controlling for the effect of escalation of headache, patients who treated early were three times as likely to report mild headache pain at dosing as those who treated late. The interaction between fast escalation of headache and mild pain was not statistically significant. Early treatment is associated with mild pain, regardless of the speed of headache escalation.
Keywords
Introduction
Patients' decision to initiate migraine treatment depends on a number of factors such as experiencing aura or not, headache-specific symptoms, headache pain severity, availability of medication, drug efficacy, cost concerns and potential side-effects. Early migraine treatment decision may also depend on patient's current headache profile. An early migraine treatment initiation is usually associated with mild headache pain (1). Recent studies suggest that early migraine treatment while the headache pain is mild might lead to improved treatment outcomes for migraine patients (2–5).
The co-occurrence of early migraine treatment and mild intensity of headache pain generates a hypothesis such that patients who treat-early and treat-mild are more likely to experience slow escalation of headache pain. In an editorial, Ferrari (6) discussed the twining of ‘treat-mild’ and ‘treat-early’ strategies as being more applicable to headaches that escalate the intensity slowly, and stated that ‘… in the past, “treating early” and “treating mild” have been incorrectly used as interchangeable terms. This of course may only be correct in patients with slowly progressing attacks but not in patients with rapidly progressing attacks’ (6). The concept of rapidly vs. slowly escalating migraine attacks has not been empirically defined or investigated. A new dimension of fast vs. slow escalation of headache to ‘treat early’ and ‘treat mild’ may shed additional light on a patient's treatment initiation process and thus better inform migraine management.
The overall objective of this study is to examine if the association between mild headache pain at treatment initiation and early treatment initiation differs by fast vs. slow escalation of headache. Specifically, we assess (i) an empirical definition of fast vs. slow headache escalation and its association with timing of treatment initiation and headache severity at treatment initiation; and (ii) whether the association between mild headache pain at treatment and early treatment initiation among migraine patients experiencing fast escalation of headache is different from those experiencing slow escalation of headache.
Methods
Study design
This study was a prospective, multi-center, observational study. Details of this study were published elsewhere (7). Briefly, migraine patients were recruited from 14 headache clinics in the United States during the first half of 2005. At study entry, participants were asked to sign the written consent forms and complete a baseline questionnaire. Participants were provided with a hand-held electronic diary and were asked to record their headache experiences daily over the course of a 30-day period. Physicians and patients were encouraged to treat as they normally would. The study was approved by the Schulman Associates Institutional Review Board, Inc.
Study population
Migraine patients aged 18 years or above, with a physician-diagnosed migraine with or without aura, were eligible to participate. Eligible patients experienced two to eight migraines per month, with a maximum of 15 headache days per month. Patients were either prescribed or given samples of an oral triptan medication for acute migraine. Patients with health conditions that have contraindications for the prescribed migraine medications, per the product insert, were excluded from the study. Patients who were treated with a parenteral migraine medication were also excluded.
The analysed sample included migraine patients who experienced at least one migraine episode during the study period. Migraine episode was determined by patients' responses of ‘probably a migraine’ or ‘definitely a migraine’ to the question ‘How certain were you that this headache was or was not a migraine?’ at headache peak.
Questionnaires
Enrolled patients were asked to keep an electronic diary daily over the next 30 consecutive days. Each diary day captured the occurrence of one headache episode, if applicable. Whenever a headache episode occurred, information regarding actual times of headache onset, headache peak, medication use and headache pain severity at the time of dosing were recorded. Non-response to any questions in the diary pertaining to the migraine attack was not possible because patients were not able to proceed to the next question without providing a response to the prior one. Patients were instructed to complete the diary between 17.00 and their bedtime. A daily reminder alerted patients to complete the diary. All recorded information was electronically transmitted nightly to the central data depository centre over the study period.
Measurement of study variables
For each migraine episode, the actual times at which migraine headache began, headache pain reached its peak intensity, and medication was administered, were recorded daily in an electronic diary over 30 consecutive days after enrollment. Headache pain severity at the time of treatment was also reported. The lapsed time between headache onset and first medication was computed. Consistent with the definition of ‘treat-early’ used in controlled clinical trials (8, 9), migraine episodes treated with medication within the first hour of headache onset were defined as ‘treat-early’, otherwise they were classified as ‘treat-late’.
Consistent with the pain severity assessment used in controlled trials, patients reported their headache pain using a four-point Likert scale (0 = no pain, 1 = mild, 2 = moderate, and 3 = severe). For the measurement of headache pain severity at the time of treatment, migraine episodes reporting ‘no’ or ‘mild’ pain were categorized as ‘mild’ while those reporting ‘moderate’ or ‘severe’ pain were categorized as ‘moderate/severe’.
Escalation of migraine was characterized as the speed at which headache reaches its peak from headache onset as reported by the patient. We used the median time (1.5 h) from onset to peak as the cutoff point to define a rapidly vs. slowly escalating headache. A headache that peaked within 1.5 h of headache onset was defined as a rapidly escalating headache and a slowly escalating headache was one that peaked more than 1.5 h after onset. A number of cutoff points were selected based on their relationship with timing of treatment initiation for sensitivity analysis in order to determine the feasibility and robustness of the selected cutoff point. The results of the sensitivity analysis are reported in the Results section.
Statistical analysis
Multivariate analyses were performed to assess the association between various factors using generalized estimating equations (GEE), which accounts for the correlation among repeated migraine episodes within patients. The compound symmetry covariance structure was specified for the GEE model. The impact of headache escalation on the association between mild pain at dosing and early treatment was evaluated via a multivariate model and the interaction between predictors was evaluated by its statistical significance. All analyses were performed using SAS statistical software V9 (10).
Classification and Regression Tree (CART) was performed using Classification and Regression Trees software V6.0 from Salford Systems (San Diego, CA) (11) to identify the optimal cutoff point for headache escalation. The lapsed time between headache onset and headache peak was assessed to best classify and predict the time to treatment initiation, measured on both binary and continuous scales. Sensitivity analyses were conducted to assess the pattern of associations between various cutoff points for the escalation of headache with ‘treat-early’ and ‘treat-mild’.
Results
Patient population
A total of 192 migraine patients enrolled in this study. Eighteen patients were excluded from the analysis for the following reasons: no diary (n = 7), no headache (n = 3) or no migraine episode (n = 8) during the 30-day study period. One hundred and seventy-four patients recorded 970 migraine episodes as identified at headache peak via the electronic diary over the 30-day study period. Of the 970 migraine episodes, 106 episodes were not treated with medication, and were excluded in subsequent data analysis. The analysed sample was based on 168 migraine patients who treated 864 migraine episodes.
Table 1 displays the demographic characteristics for the study participants. Enrolled patients were in their productive years (mean age = 42.6 years,
Demographic distribution of sample

∗Two patients did not provide responses regarding their education level.
†Three patients did not provide responses regarding their employment status.
The mean and median elapsed times from headache onset to first medication were 1.9 h (
Summary statistics and frequency of key study variables

∗Treat-early was defined as taking migraine treatment within the first hour of headache onset.
†Fast escalation of headache was defined as headache pain severity reaching its peak intensity within the first 1.5 h of headache onset.
Sensitivity analysis of escalation of headache
A sensitivity analysis was performed to assess the optimal cutoff point for fast vs. slow escalation of headache. Escalation of headache predicted the time of treatment initiation, measured as a binary variable and a continuous variable. In the CART analysis, using a binary-coded variable of time to treatment initiation (‘treat-early’) as the target, the cutoff point for headache escalation was identified at 1 h after the headache onset (Table 3, Column 1). Using a continuous measurement of time to treatment initiation as the target, the cutoff point for headache escalation was identified at 1.98 h after the headache onset (Table 3, Column 3). Columns 2 and 4 of Table 3 displayed the median (1.5 h) and mean (2.74 h) cutoff points of headache escalation from headache onset to headache peak.
Associations between time of treatment initiation and severity of headache pain by various cutoff points for fast escalation of headaches

Strong positive associations between treat-early and four cutoff points of escalation of headache were presented in Table 3 (Row 1) (OR = 3.1 to 12.7). The shorter the time lapsed from headache onset to headache peak was, the stronger was the association with early treatment.
Negative associations between mild pain at dosing and four cutoff points of escalation of headache were shown in Table 3 (Row 3) (OR = 0.6 to 0.7). Patients experiencing fast escalating headaches were more likely to report enduring moderate/severe pain at the time of treatment (i.e. less likely to experience mild pain at dosing).
Regardless of the choice of cutoff point for headache escalation, the associations between headache escalation with the time to treatment and headache escalation with pain severity at dosing were similar. The median cutoff point (1.5 h after the initial headache onset) for defining fast vs. slowly escalating headaches was chosen for two reasons: (i) non-overlap with the cutoff point for treat-early; and (ii) midway between cutoff points as suggested by CART analysis.
Associations of time to treatment with headache pain severity at dosing and headache escalation
The unadjusted and adjusted associations between headache pain severity at dosing and timing of treatment initiation are shown in Table 4. As presented in Model 1 of Table 4, at the time of dosing, a larger proportion of treat-early episodes experienced mild pain (22.8%) than treat-late episodes (10.0%). That is, patients who treated early were 2.3 times as likely to experience mild headache pain as those who treated late (OR = 2.3; 95% CI, 1.5–3.4; P-value < 0.0002).
Associations of time to treatment with headache pain severity at dosing and headache escalation
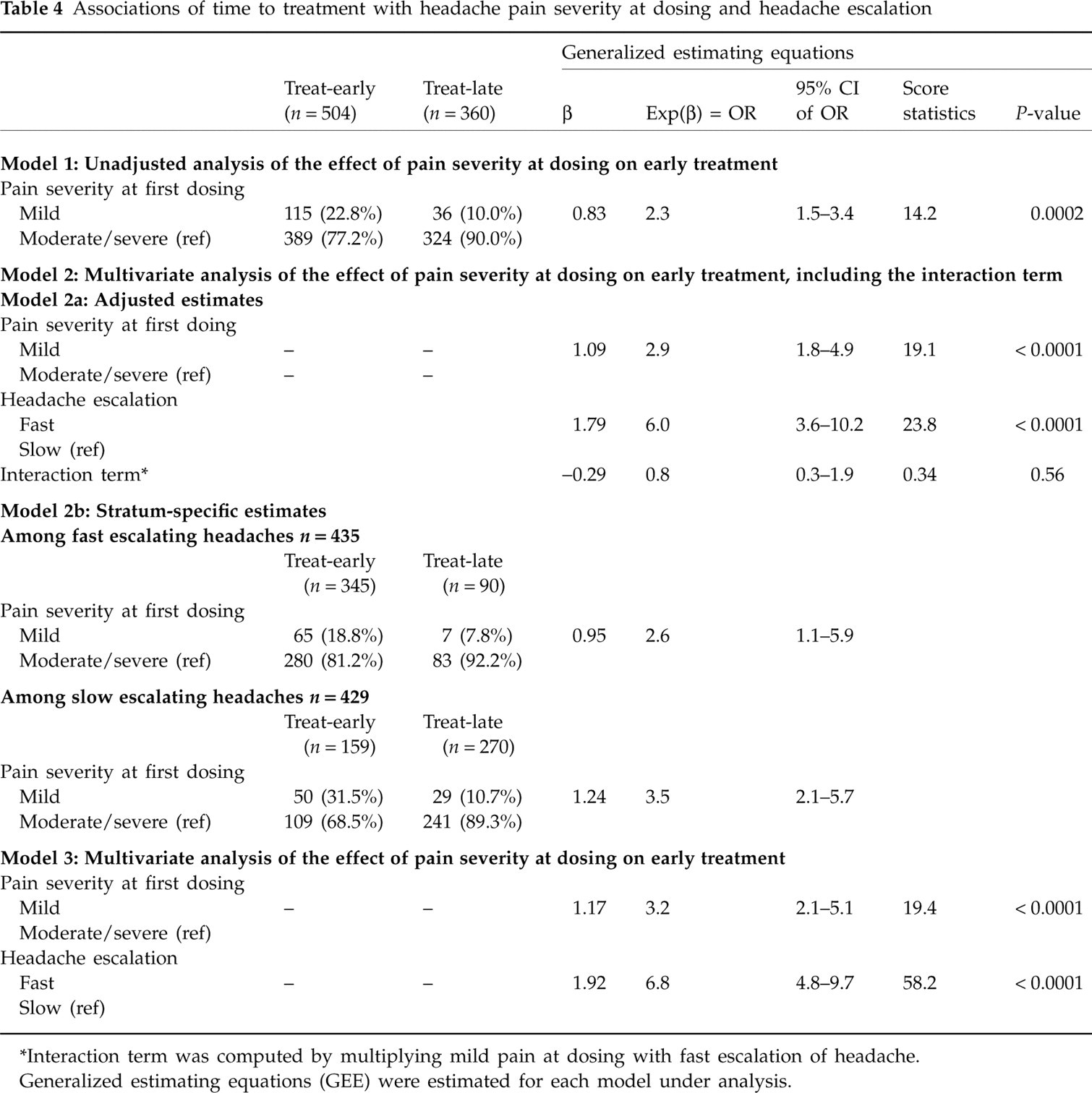
∗Interaction term was computed by multiplying mild pain at dosing with fast escalation of headache.
Generalized estimating equations (GEE) were estimated for each model under analysis.
A multivariate analysis that included headache pain severity, headache escalation, and an interaction term that was computed as a cross-product term of mild pain at dosing and fast escalation of headache, is shown in Model 2 of Table 4. As shown in Row a (Table 4, Model 2), the interaction term was not statistically significant (OR = 0.8; 95% CI, 0.3–1.9; P-value = 0.56), which suggested that the association between treat-early and treat-mild did not differ statistically between fast and slowly escalating headaches.
Stratum-specific estimates are presented in Row b (Table 4, Model 2) to show the specific effects of headache pain severity at dosing on early treatment across each stratum of headache escalation. Among fast escalating headache episodes, a significantly greater proportion of treat-early episodes experienced mild pain at dosing (18.8%) than those with treat-late episodes (7.8%). Among patients experiencing fast escalating headaches, patients who treated early were 2.6 times as likely to experience mild headache pain as those who treated late (OR = 2.6; 95% CI, 1.1–5.9).
Among slow escalating headache episodes, a significantly greater proportion of treat-early episodes experienced mild pain at dosing (31.5%) than those with treat-late episodes (10.7%). Among patients experiencing slow escalating headaches, patients who treated early were 3.5 times as likely to experience mild headache pain as those who treated late (OR = 3.5; 95% CI, 2.1–5.7).
For reasons of parsimony, a final multivariate model that included pain severity at dosing and headache escalation is presented in Model 3 of Table 4. Both mild headache pain and fast escalating headache were independently associated with early treatment initiation. Controlling for the effect of headache escalation, patients who treated early were three times as likely to report mild headache pain at dosing as those who treated late (OR = 3.2; 95% CI, 2.1–5.1; P-value < 0.0001). Fast escalation of headache, as compared with mild pain at dosing, was strongly associated with treat-early (OR = 6.8; 95% CI, 4.8–9.7; P-value < 0.0001).
Discussion
To our knowledge, this is the first study to examine the three-way associations of headache escalation, pain severity at dosing and time to treatment among adult migraine patients.
We examined Ferrari's (6) proposition that the association between ‘treat-mild’ and ‘treat-early’ may only apply to migraine patients experiencing slowly escalating headaches. In this study, however, we found similar relationships between ‘treat-mild’ and ‘treat-early’ among patients experiencing slow as well as fast escalation of headache. While fast escalating headache was a stronger predictor of an early treatment decision, in a multivariate analysis accounting for the effect of speed of headache escalation, patients remained more likely to initiate treatment early while headache pain was mild. Our results suggest that the existing migraine literature may underestimate the association between ‘treat-mild’ and ‘treat-early’.
Existing literature focuses largely on treatment efficacy as the outcome variable and assesses the relative importance of headache intensity vs. time to treatment (2, 3, 12). The current study attempted to understand the decision process of time to treatment initiation and to evaluate factors that may influence such decision making. We showed that migraine patients with fast escalating headaches tended to treat earlier than slowly escalating headaches. The decision on timing to treatment largely depends on how quickly their migraine escalates to peak level, and less so on the pain severity.
There are a number of strengths of the study. From a methodological viewpoint, we systematically addressed multiple factors that we believed to be inter-correlated. In addition, we used a data set that was based on a large sample of 168 physician-diagnosed patients who experienced multiple migraine episodes and took medication on 30 consecutive days after patient enrollment. Migraine, not headache, episodes were chosen for analysis in this study because of their relevancy to the research question. Migraine patients who did not take medication were excluded from the analysis because there was no valid data point for the variable of time to treatment.
The choice of variable type depends largely on the research hypothesis under study. The variables of interest in this study were defined on a categorical, rather than continuous, scale. The research objective was to understand the relationship between time to treatment initiation and the rate of headache escalation. Continuous measurement of these two variables was deemed less appropriate because a linear assumption of the time to treatment initiation or the rate of headache escalation does not characterize a patient's behaviour. Though it may seem subjective, the categorization of these two variables captures patients' treatment behaviour and migraine profiles. Our definition of ‘treat-early’ as the initial hour after headache onset is less controversial, as other clinical trial data have employed the same cutoff criterion (8, 9). The concept of ‘treat-early’ implies taking migraine medication before migraine escalates to its peak intensity. ‘Treat-early’, defined in this study as taking medication within the first hour of onset, was shorter than the median or mean time from headache onset to headache peak.
The definition of fast escalation of headache focuses on the speed at which migraine reaches its peak intensity. To the best of our knowledge, this is the first study to define and operationalize the concept of fast escalation of headache. To better define the categorization of headache escalation, we employed the CART methodology. CART's recommendation of cutoff for headache escalation at 1 h after headache onset yields the best prediction of time to treatment, as measured by a binary scale. To avoid a potential confounding problem with ‘treat-early’ (treatment within the first hour of headache onset), a fast escalation of headache ought to be operationalized at a time different from, and preferably after, the time to treatment initiation. Our choice of median cutoff point was deemed to be the most appropriate definition. Additional research of the definition and operationalization of fast escalation of headache is needed to better understand its role in the association between headache pain at dosing and time of treatment.
The limitations of this study must be taken into consideration. One limitation of this study is the fact that patients did not record their headache events in real time, but recorded their recollection of these events on the same day that they experienced a migraine. Despite the fact that accuracy of times to events might have been compromised, the sequence of events such as the onset of migraine pain, administration of medication and experience of the greatest migraine pain is unlikely to be confused.
We did not evaluate a full escalation of headache. It is conceivable that time of treatment initiation may affect the duration of headache. In another publication, we showed that early treatment is associated with shorter time to headache peak but not headache severity at peak (13). Other factors such as accessibility of migraine medication may also influence patients' decision on the timing of treatment for a given attack. Nevertheless, such factors potentially weaken the association between treatment decision and the underlying escalation of headache.
In conclusion, the association between ‘treat-mild’ and ‘treat-early’ is prominent among migraine patients. Our findings suggest that, in our cohort of patients, early treatment is often associated with mild headache pain whether the headache attacks are fast or slowly escalating. The frequency of mild pain at treatment remains low, however. Physicians should continue to educate and empower migraine patients to treat migraine as early as migraine symptoms are evident in order to reap clinical benefits of early migraine treatment (14).