
Abstract
Background:
Better understanding of migraine treatment in US clinical practice could be facilitated by availability of Migraine Disability Assessment (MIDAS) questionnaire results collected in routine care. We present results for migraine patients with MIDAS collected in routine clinical practice through an electronic medical record (EMR) system that presented the MIDAS questionnaire as an electronic form during the patient office encounter. The purpose of this retrospective observational study was to gain better understanding of migraine disability and migraine treatment patterns in US real-world clinical practice.
Methods:
In this EMR database study, patients were required to have 12 months baseline time for review of patient and clinical characteristics. Adult patients with documentation of migraine with subsequent MIDAS questionnaire data collected between March 2017 and September 2018 were included. Based on MIDAS responses patients were categorized into grade I—little or no disability, grade II—mild disability, grade III—moderate disability, and grade IV—severe disability.
Results:
This study included 2731 migraine patients with MIDAS results. Overall, 2309 (84.5%) were female with an average age of 46.7 years. Distribution by disability grade was 1161 (42.5%) little or no disability, 424 (15.5%) mild disability, 477 (17.5%) moderate disability, and 669 (24.5%) severe disability. Compared to overall, a larger proportion of patients with severe disability had baseline treatment with acute (71.3% vs. 67.6%) or preventive medications (70.4% vs. 62.0%) and to be on 3+ acute (9.4% vs. 7.0%) or 3+ preventive therapies (17.0% vs. 14.5%).
Conclusion:
Availability of MIDAS results in usual care provides additional insight into migraine care.
Introduction
Migraine is an underdiagnosed and undertreated primary headache disorder characterized by recurrent, painful attacks and is estimated to affect 36 million Americans. 1 The Global Burden of Disease Study provides the most current estimates of migraine prevalence, incidence, and disease burden as measured by years lived with disability (YLD). Globally, migraine had an age-standardized prevalence of 14.4% and was the second leading cause of disability in 2016, contributing an estimated 45.1 million YLD. 2 The economic burden of migraine is high as a result. In the United States (2014), total annual costs, direct and indirect, associated with migraine have been estimated at US$78 billion . 3
Migraine management is multifaceted and may include patient education, lifestyle modification, as well as use of acute and preventive therapies. 4 Identification of patients requiring preventive migraine therapy and selection of the most appropriate treatment strategy may prevent progression from episodic to chronic migraine and reduce the burden of disease associated with frequent migraine. 5 For migraine therapy, reduction in migraine headache days has been shown to be a sensitive response measure in both clinical trials and practice. 6 However, a successful therapeutic outcome in migraine headache days also depends on level of pain and associated symptoms, level of disability, and functional capacity. Because of this, there is a need for validated outcome measures that evaluate the effect of treatment on functional capacity, disability, and quality of life to help guide clinical decision-making with respect to need for and changes in therapy. 7 The recently updated American Headache Society consensus statement on integrating preventive migraine treatments into clinical practice lists eight validated instruments that may be used to measure meaningful change after a therapeutic intervention for migraine prevention, including the Migraine Disability Assessment (MIDAS) questionnaire. 7
The MIDAS was designed to quantify headache-related disability over a prior 3-month period. 8,9 This instrument consists of five items that reflect the number of days reported as either missing or with reduced productivity at work, home, and social events; higher values are indicative of more disability. This instrument is considered highly reliable and valid and is correlated with clinical judgment regarding the need for medical care. 10 The MIDAS questionnaire is regularly used as a clinical assessment instrument in clinical trial studies. In a review of available validated outcome measure instruments for evaluating outcomes of preventive treatments for migraine headaches, Mannix et al. identified the MIDAS as one of three such instruments most often used in clinical trials. 11
Use of the MIDAS in clinical practice settings is limited. Information on disability collected using the MIDAS in real-world care is mostly limited to a number of longitudinal panel studies and cross-sectional surveys. These studies generally provide descriptive information on baseline demographic characteristics, headache features, and disability as measured by use of the MIDAS. 12 –19 A small number of studies conducted in clinical practice have used the MIDAS as a measure of disability both as a baseline characteristic and as a clinical outcome. 20 –22
Evaluation of the clinical effectiveness of migraine treatments using existing databases is challenging because the measurable outcomes of medication intervention, number of migraines, and headache days experienced by a patient within a defined time interval, typically 30 days, are self-reported and are not routinely collected in clinical practice, and hence are not available in existing clinical databases. We present results for migraine patients with MIDAS collected in routine clinical practice through an electronic medical record (EMR) system that presented the MIDAS questionnaire as an electronic form during the patient office encounter. The purpose of this retrospective observational study was to gain better understanding of migraine disability and migraine treatment patterns in US real-world clinical practice.
Methods
Study design and data source
This was a retrospective observational database study of EMR data from practices entering MIDAS data as part of usual care. The MIDAS questionnaire was made available in routine clinical practice to users of the Practice Fusion EMR platform (PF EMR) starting in March 2017. The PF EMR is currently in use at over 25,000 practices, mostly single provider or small group practices, in all 50 US states representing approximately 6% of all ambulatory care among primary care and specialist practices in the United States. 23 The patient population served is comparable to the overall US population in terms of age, gender, and geographic distribution. 24 Patient consent was not required as MIDAS results were collected and entered into the EMR platform as part of usual patient care. The resulting EMR data were made available for research in the form of a certified Health Insurance Portability and Accountability Act (HIPAA)–compliant de-identified research database. As a noninterventional, retrospective database study using data from a certified HIPAA–compliant de-identified research database, approval by an institutional review board was not necessary.
Study population
This retrospective observational study included patients aged 18–65 years with documentation of migraine diagnosis in the PF EMR database. Patients with migraine were eligible for inclusion based on meeting one of the following three criteria: migraine diagnosis entered in their medical record (ICD9: 346* and ICD10: G43*), one or more prescription records for an acute migraine medication (e.g. triptans and ergotamines) that listed at least one refill, and two or more prescription records for an acute migraine medication, without refills, within 365 days of one another. The majority (approximately 90%) of patients were included because they had the migraine diagnosis codes. Patients with migraine were required to have a completed MIDAS survey including disability score and measure of headache days completed between March 1, 2017 and September 30, 2018 (index date) with their documentation of migraine occurring on or prior to this date. In addition, patients were required to have a clinic visit or encounter 12 or more months prior to their index date to establish a 12-month baseline period.
Measures
The MIDAS is scored as the sum of the first five questions, each measured as days in the last 3 months, and then categorized into four disability grades:
Grade: Disability level
Grade I: Little to no disability (0–5 days) Grade II: Mild disability (6–10 days) Grade III: Moderate disability (11–20 days) Grade IV: Severe disability (21+ days)
Two additional questions assess the number of days with headaches in the last 3 months (item A) and a scale of the painfulness of the headaches (item B).
Statistical analysis
To gain better understanding of migraine disability and treatment patterns, we described patient demographic and clinical characteristics by migraine disability grade subgroups as determined from the MIDAS instrument. To provide further detail on treatment pattern distributions between primary and specialty care, we stratified by specialty of the provider completing the MIDAS instrument. Descriptions for patients with MIDAS scores are presented as frequencies and percentages for categorical variables and means with standard deviations for continuous variables. Comparisons were made across disability grade using χ 2 statistical tests. Statistical tests were two-sided, with an α-level of 0.05 for statistical significance. No adjustments were made for multiple comparisons.
Results
Overall, 862,392 patients were identified with documentation of migraine in their medical chart. A completed MIDAS was available for 5804 patients any time after their documented migraine diagnosis date. Of these, 4758 migraine patients were aged 18–65 years at the time of MIDAS completion. Limiting to patients with a 12-month baseline period, defined as documentation of a clinic visit or encounter 12 or more months prior to their index date, resulted in a final study population of 2731 (Figure 1).
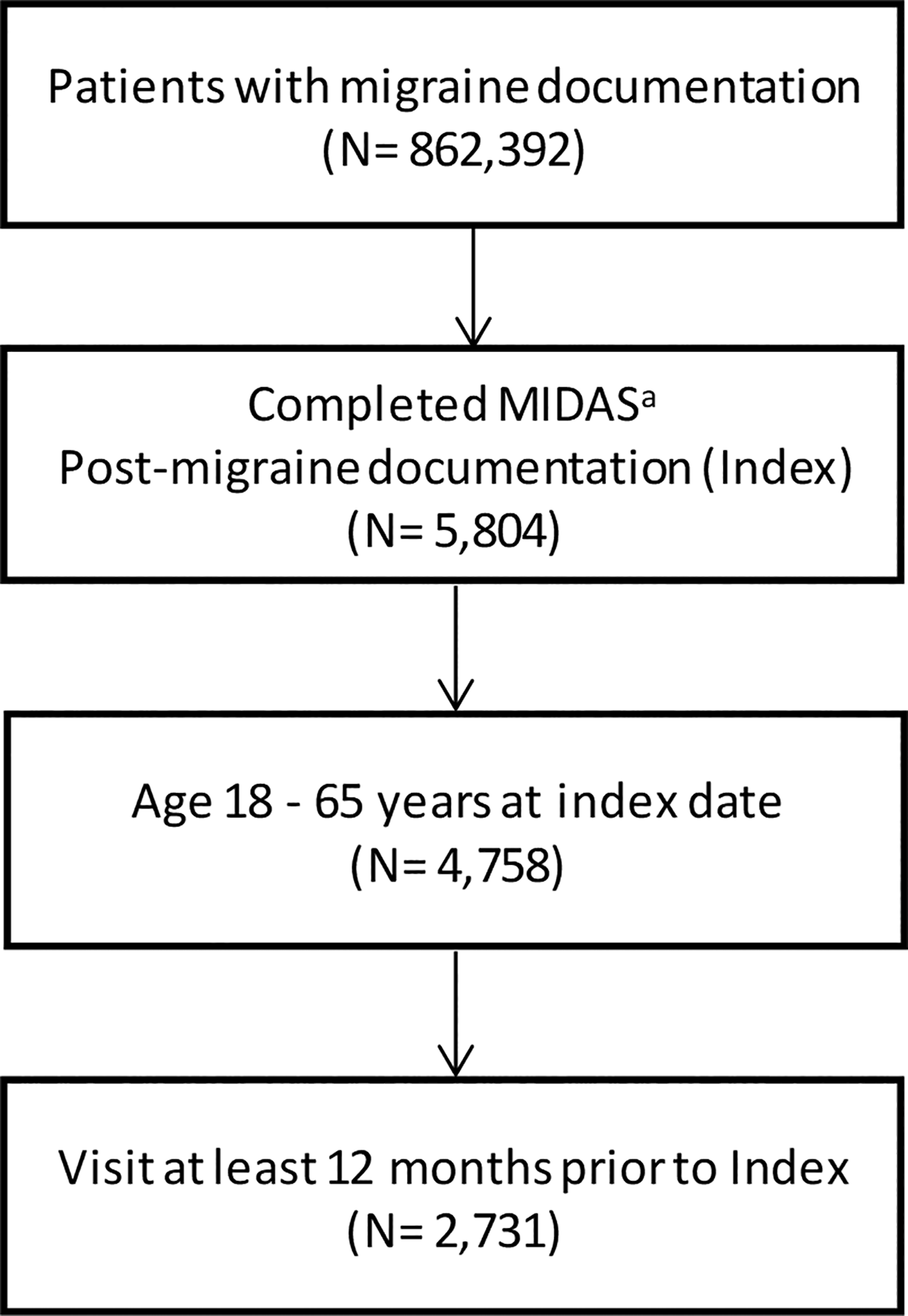
Study population identification. aMIDAS: Migraine Disability Assessment, validated questionnaire.
Patient distribution by migraine disability grade was 1161 (42.5%) little or no disability, 424 (15.5%) mild disability, 477 (17.5%) moderate disability, and 669 (24.5%) severe disability. Primary care providers (PCPs) saw a larger proportion of patients with little or no disability and specialists (neurology or pain) saw a larger proportion of patients with severe disability (p < 0.001). Overall, approximately 43% of patients were seen by neurologists or pain specialists. This proportion increased to almost 55% in patients with severe disability (Table 1). Overall, 2309 (84.5%) of patients were female with an average age of 46.7 years (Table 1). Patient age did not differ by disability grade, the proportion of female patients differed by disability grade with the highest proportion female in the severe disability grade group.
Baseline demographic characteristics.
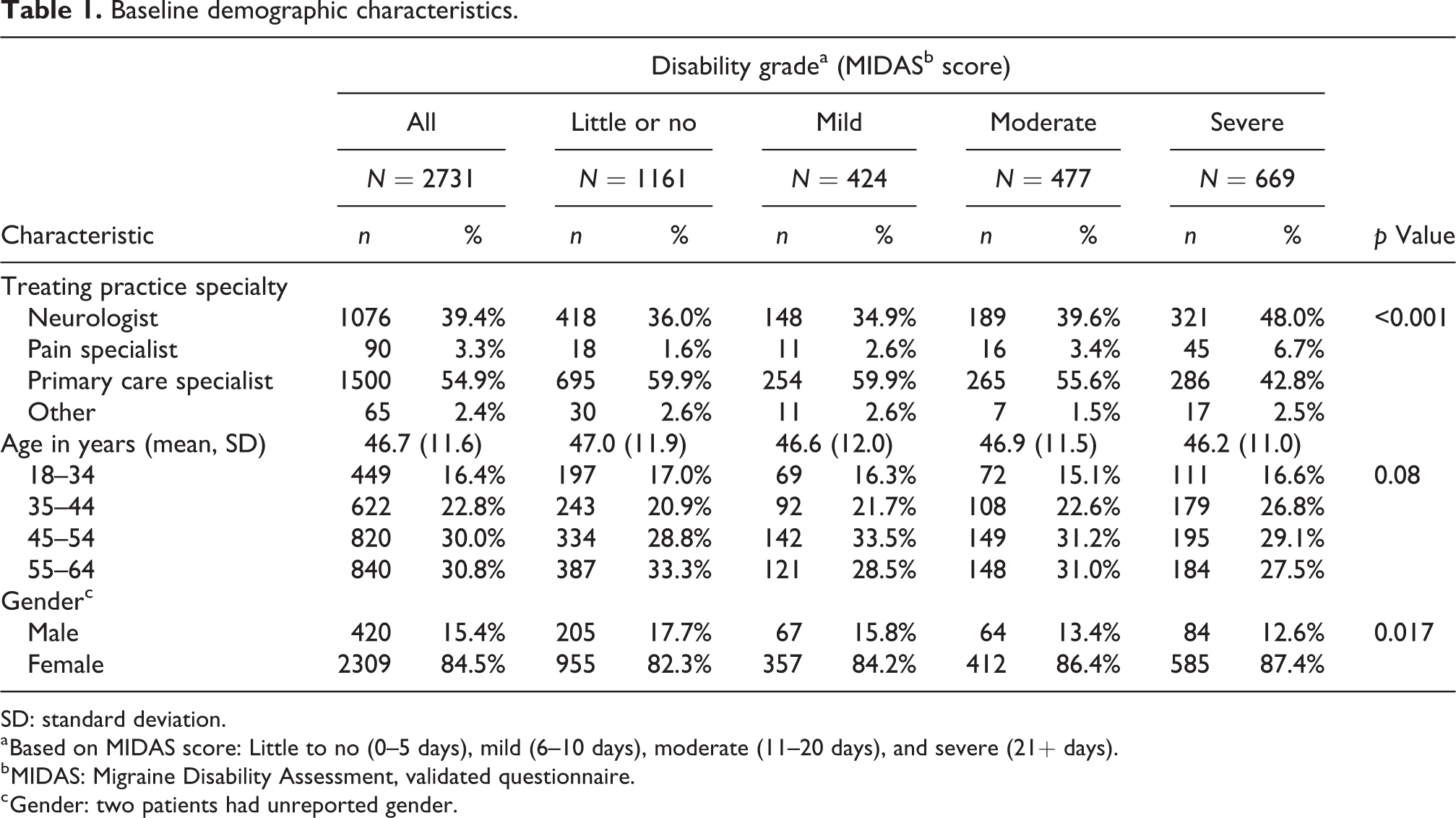
SD: standard deviation.
a Based on MIDAS score: Little to no (0–5 days), mild (6–10 days), moderate (11–20 days), and severe (21+ days).
b MIDAS: Migraine Disability Assessment, validated questionnaire.
c Gender: two patients had unreported gender.
Clinical characteristics and office visits also varied by MIDAS score. The proportion of obese patients did not significantly differ by disability grade (p = 0.07; Table 2). Both frequency of headache days and level of pain associated with headaches as ascertained through MIDAS items A and B differed by disability grade with larger proportions in the higher disability grades (p < 0.001 for both). Over half of patients with severe disability reported 21 or more headache days in the last 3 months and over 80% of patients with severe disability also reported a pain score of 6 or more indicating moderate to severe headache pain (Table 2). Patients with higher disability grade had more frequent health-care encounters as measured by office visits during the baseline year with the index practice, 5.6, 6.2, 6.6, and 7.4 for little or no, mild, moderate, and severe disability, respectively (Table 2).
Baseline clinical characteristics.

a Based on MIDAS score: Little to no (0–5 days), mild (6–10 days), moderate (11–20 days), and severe (21+ days).
b MIDAS: Migraine Disability Assessment, validated questionnaire.
Overall, over two-thirds of patients were prescribed an acute treatment during the baseline period, of which most of the prescriptions were for triptans and over 60% of patients were prescribed a preventive treatment during the baseline period, with prescriptions for topiramate, cardiovascular drugs, and antidepressants all written about equally (Figure 2). Use of any acute therapy was lowest among patients with little or no disability, 61.8% compared to 71.5, 73.0, and 71.3% in patients with mild, moderate, and severe disability, respectively (Figure 2). The proportion of patients with use of opioids increased by disability grade, 15.8, 19.3, 20.3, and 27.4%, for little or no, mild, moderate, and severe disability, respectively (Figure 2). Use of any preventive therapy increased with disability grade from 56% in patients with little or no disability to 70% in patients with severe disability. Use of both topiramate and antidepressants contributed to the higher use of preventive treatment by increasing disability grade (Figure 2).
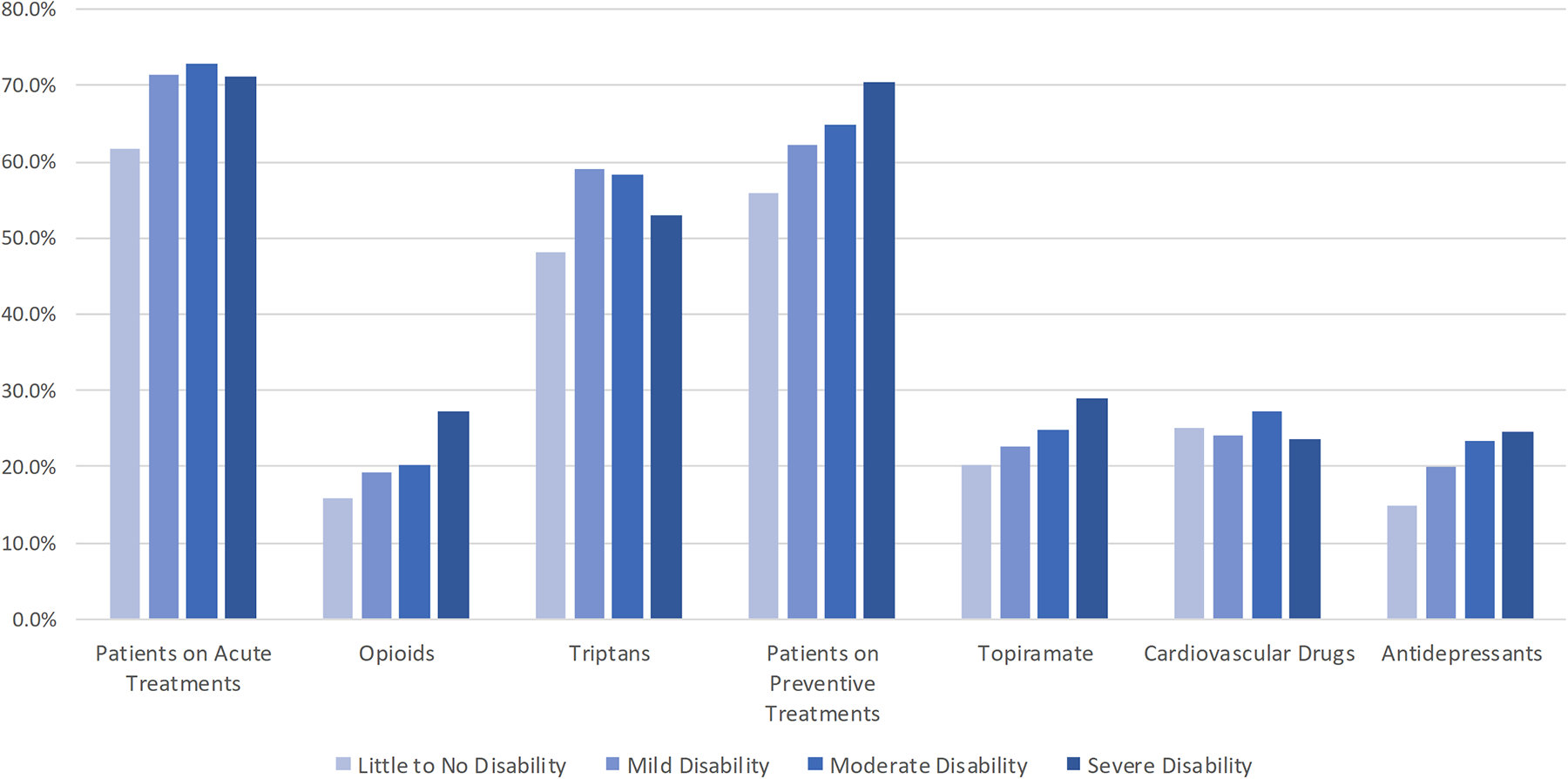
Baseline treatments by disability grade. Disability grade based on MIDAS score: Little to no disability (0–5 days), mild (6–10 days), moderate (11–20 days), severe (21+ days). MIDAS: Migraine Disability Assessment, validated questionnaire.
PCPs had a larger proportion of patients with prior acute treatment then specialists (77.0% vs. 56.1%), and a lower proportion of patients with prior preventive treatment (57.7% vs. 68.8%) (Figure 3). Use of opioids and triptans both contributed to the higher proportion in use of acute treatment by PCPs. Topiramate accounted for most of the higher use of preventive treatments by specialists (Figure 3).

Baseline treatments by provider specialty. Provider specialty: Specialty of provider completing the MIDAS questionnaire. MIDAS: Migraine Disability Assessment, validated questionnaire.
Discussion
To the best of our knowledge, this is the first published study to include patients with MIDAS assessments completed in the course of routine clinical practice. The current database study analyzed completed MIDAS assessments from a total of 2731 study-eligible patients. While the number of patients assessed using MIDAS in this study was less than that reported in three large migraine surveys, the International Burden of Migraine Survey, 15 the Chronic Migraine Epidemiology and Outcomes survey, 17 and the American Migraine Study II, 12 it was greater than the number of participants assessed in two US clinical studies. 19,22
The published study most similar to the current study is the Migraine Disease Specific Programme (DSP), 19 a survey of 1487 migraine patients identified from 150 enrolled clinical practices. Similar to the DSP, most patients in the current study had documentation of physician diagnosed migraine. In addition, the distribution between primary care and neurologists in the current study and the DSP was also similar, approximately 60% and 67%, respectively. Patients in the current study were somewhat older than in the DSP (46.7 vs. 39.8) and a larger proportion had severe migraine disability (24.5% vs. 11.3%). The DSP took a sequential sample of patients from each enrolled site and only 43% of patients had MIDAS data available, where the current study was based on a set of patients where 100% of patients had a MIDAS instrument completed. Also, with respect to the DSP, prior treatment use in the current study shows a lower proportion of patients with prior acute treatment (67.6% vs. 93.2%) and a higher proportion of patients with prior preventive treatment (62.0% vs. 56.0%). Considering that we found a lower proportion of patients with prior acute treatment than the DSP, patients who were identified solely on the use of migraine medications for study inclusion did not have a material impact on this comparison.
Effective clinical management of migraine frequently entails the use of both acute and preventive therapies to mitigate symptoms and disability. In the patients studied, just over half or 55% of patients with severe disability were treated with both acute and preventive medications, indicating that migraine remains inadequately treated in a large number of patients in real-world practice.
A strength of the current study is the size and coverage of the EMR data source provider network. However, the source network is made up of primarily small, independent practices, and results may not be generalizable to other care settings. We required patients to have 12 months of time in the EMR database for review of therapies prior to completion of a MIDAS questionnaire. This removed 2027 patients from our analysis that had a completed MIDAS questionnaire. The patients that we removed from the analysis tended to have a higher grade of migraine disability than those that were included. As this was a descriptive study, the main effect of excluding these patients was a reduction in sample size that otherwise did not impact our findings.
Our study findings should also be considered within the context of study design and limitations inherent in EMR data collection. As this was a retrospective observational study, potential confounding effects due to unknown variables, such as diet, lifestyle, and medication adherence, which were not assessed in this study cannot be ruled out. Data captured in an EMR system reflects routine clinical practice rather than mandatory assessments at pre-specified time points, which may have an impact on the quality and timing of available data. Available data may still be subject to incompleteness (lack of documentation of patient care) and to potentially inaccurate data entry into the EMR system. Our drug use definitions are based on written prescription orders with no confirmation of whether the prescription was filled at the pharmacy or taken by the patient. As a result, measures of drug use related to timing are based on order dates and may be imprecise with respect to actual medication start and stop dates.
Conclusions
In this study of EMR data from practices entering MIDAS data as part of usual care, patients with severe disability comprised almost a quarter of the patients studied and had more complex treatment profiles. Among patients with migraine, differences were observed in use of acute and preventive treatments by both disability grade and provider specialty. Migraine disability grade information collected through use of the MIDAS instrument provides additional information for treatment decision-making as well as insight into migraine care that is not generally available in routine clinical practice.
Clinical implications
Availability of the MIDAS score in real-world clinical practice can provide additional insight into patient care. Among patients with migraine, differences were observed in use of acute and preventative treatments by both disability grade and provider specialty.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Amgen. Victoria Chia and Akeem Yusuf are employees and shareholders of Amgen Inc. Lee Kallenbach and Alina Bogdanov are employees of Veradigm Health, under contract with Amgen Inc. for the conduct of this study.