
Abstract
Introduction
According to the IHCD-3β classification, chronic migraine (CM) is headache occurring on 15 or more days/month. Episodic migraine (EM) can be divided into low frequency (LFEM) and high frequency (HFEM) depending on the headache days suffered per month.
Methods
We performed a clinical comparison of migraine characteristics according to monthly headache days suffered. Patients were divided into three groups: LFEM (1–9 headache days/month), HFEM (10–14 headache days/month) and CM (≥15 headache days/month).
Results
The analysis included 1109 patients. Previously reported differences between EM and CM were replicated. However, there were three times more clinical differences between LFEM and HFEM than between HFEM and CM (15 vs. 6). A new model that takes 10 headache days as a cut-off value for CM would have a minimally higher predictive capacity (72.8%) and no statistical differences (71.8%) when comparing it to the current classification.
Conclusions
HFEM patients have few clinical differences compared with CM patients. This includes the poor outcomes regarding headache-related disability and impact on daily life. According to these findings, neurologists and headache specialists should consider that the emotional and functional impact in HFEM patients could be as disabling as in those with CM.
Introduction
Migraine is a brain disorder with episodic attacks consisting of head pain and other neurological symptoms. It has a variable clinical course over the patient’s lifetime. In some patients migraine can improve to having few or no attacks, others have a stable evolution and, in a subset, attacks increase in frequency over a period of time and may become chronic.
During the 17th century’s scientific revolution, Thomas Willis was the first to suggest the basis of how a headache could become daily (1). But the modern discussion about the nature of frequent headache started in 1982, when Mathew et al. suggested the possibility that migraine could transform into chronic daily headache over time (2). Since then, the debate on the concept of chronic headache has been controversial. Silberstein et al. (3) divided chronic daily headache into different groups which included tension-type headache, new daily persistent headache, hemicrania continua and transformed migraine. Transformed migraine emphasises the concept of the nature of disorder: Headaches starts being episodic and later transforms into a pattern of daily or near-daily frequency. Chronic migraine (CM) as we know it today was first introduced in the second edition of the International Classification of Headache Disorders (ICHD-2) in 2004 as a complication of migraine (4). In the latest classification (ICHD-third edition beta version) CM is considered to be a type of migraine in itself and is defined as headache occurring on 15 or more days per month for more than three months which has the features of migraine headache on at least eight of these days (5).
On the basis that migraine can be considered as a progressive disease that may transform to CM, Bigal and Lipton (6) proposed a transition model: Individuals who do not have migraine may develop episodic migraine (EM) that can increase in frequency progressively depending on the existence of certain risk factors such as medication or caffeine overuse, obesity or concurrence of other chronic pain syndromes. Accordingly, EM can be divided into low frequency (LFEM) and high frequency (HFEM) depending on the headache days suffered per month. This model creates the dynamic concept of the possibility of migraine transformation towards progression or remission.
The prevalence of CM is estimated to range from 1% to 5% depending on the definition of CM (7). Over the course of one year, 3% of individuals with EM transform to CM (8). Modifiable risk factors for transformation are attack frequency, obesity, medication overuse, stressful life events, caffeine overuse and snoring (9). Compared to EM, CM has been associated with worse outcomes including headache-related disability and health-related quality of life (10) and it is consistently associated with greater productivity loss, more consultations, more or longer hospitalisations and higher direct and indirect costs than episodic headaches (11).
The aim of this study is to perform a clinical comparison of patients suffering from migraine according to the headache days per month in order to see whether if 15 days of headache per month or more reflect the clinical characteristic of disability and impact from migraine.
Methods
We performed a prospective observational study. We included consecutive patients from the headache outpatient clinic. A headache neurologist took a clinical history with the following information: (I) demographics (age, sex, race, marital status, level of education and working status); (II) personal background (allergies, physical activity, menses, sleep disorders and tobacco, alcohol or xanthenes intake); (III) comorbidities; (IV) pain characteristics (location, quality, intensity (visual analogue scale, numeric scale (1–10) and verbal assessment))), pain frequency and duration; (V) presence of aura; (VI) associated symptoms (nausea, vomiting, photophobia, phonophobia, osmophobia, dizziness, worsening with movement, allodynia—12-item Allodynia Symptom Checklist (ASC12)); (VII) migraine triggers; (VIII) premonitory features; (IX) preventive treatment (present, past, type, duration, effectiveness, secondary effects); (X) acute treatment and presence or history of medication overuse as well as (XI) impact on quality of life (Migraine Disability Assessment Test (MIDAS), Headache Impact Test (HIT-6), Short Form Health Survey (SF-36v2)), (XI) anxiety and depression (State/Trait Anxiety Inventory (STAI), Beck Depression Inventory (BDI-II)). A total of 57 variables were analysed. The study was approved by the Vall d’Hebron Clinical Research Ethics Committee (PR(AG)15/2008) and all participants gave written informed consent.
Patients were classified following the ICHD-2 as migraine without aura (MO) and migraine with aura (MA). Patients were also classified according to headache frequency as EM (less than <15 days/month of headache) or CM (≥15 days of headache/month). Furthermore, patients with EM were divided between LFEM (0–9 days of headache/month) or HFEM (10–14 days of headache/month) (6).
We performed a comparative analysis between EM and CM based on ICHD classification. After that, the same analysis was made between LFEM, HFEM and CM. We performed a receiver operating characteristic (ROC) curve analysis in order to explore best cut-off points to define difference for every condition. Finally, we used a new cut-off point (≥10 headache days/month) to classify patients according to headache frequency and compared it with the classical cut-off point for CM (≥15 headache days/month). In order to assess if this new classification would be better than the classical, regression models were created based on disability and impact on life variables (MIDAS, HIT-6, STAI and BDI-II scales). Predictive capabilities of both models were compared.
Our hypothesis was that patients who suffered from more than 10 days of headache per month presented a similar emotional and functional impact as chronic migraineurs.
Statistical analysis
Descriptive and frequency statistical analysis were obtained and comparisons were made by use of the SPSS statistical package, version 15.0 for Windows. Variables not normally distributed (P-P plot) were expressed as median (interquartile range). Statistical significance for intergroup differences was assessed by Pearson’s chi-square or Fisher’s exact text for categorical variables, Student’s t test for continuous variables and Mann-Whitney U test for quantitative variables without an approximately normal distribution (non-parametric data). Ordinal variables were compared using the linear trend chi-square test. Multivariate logistic regression analyses with the different classifications of migraine frequency (≥10 and ≥15 headache days per month) were performed and predicted probabilities were calculated in order to measure the predictive ability of the models. We created the models based on emotional and functional impact variables (MIDAS, HIT-6, STAI, BDI-II). We assessed model discrimination by ROC curves. The area under the ROC curve showed the discriminating ability of the model; an area of 0.5 indicates no discrimination, and an area of 1.0 indicates perfect discrimination.
Comparison between areas was performed with MedCalc Statistical software. ROC curves were also used to obtain sensitivities (Se) and specificities (Sp) for each cut-off point of migraine frequency depending on the patient condition and other factors. The optimal cut-off point was obtained by using the maximum value of the Youden (J) index (Se + Sp−1) (12). A p value <0.05 was considered statistically significant.
Results
Demographics and personal background.

EM: episodic migraine; CM: chronic migraine; BMI: body mass index; OSAS: obstructive sleep apnoea syndrome; SD: standard deviation. *p<0.05; **p<0.001.
Comorbid conditions and migraine.

EM: episodic migraine; CM: chronic migraine. *p<0.05; **p<0.001.
Regarding features previously described as risk factors for migraine chronification, though there were a higher proportion of females and lower educational level in the CM group, those differences were not significant. However, significant differences were found in the presence of sleep disorders (68.6% EM vs. 80.7% CM p < 0.001) and allodynia (35.3% EM vs. 45.7% CM p < 0.001), which is considered a clinical marker of central sensitisation and medication overuse (3% EM vs. 20.9% CM p < 0.001). A total of 79 individuals fulfilled International Headache Society (IHS) criteria for medication overuse. The majority of patients who overused analgesia (70.9%) were taking nonsteroidal anti-inflammatory drugs (NSAIDs), 36.7% were taking triptans, 15.2% analgesics in combination with ergotamine and 48.1% overused other analgesics including paracetamol, metamizole or opioids. EM and CM patients in our sample did not show differences in mean body mass index (BMI), but they did in prevalence of obesity, which was lower in the CM group (14.3% EM vs. 8.7% CM p = 0.020).
Disability and quality of life assessment.

BDI: Beck Depression Inventory; EM: episodic migraine; CM: chronic migraine; MIDAS: Migraine Disability Assessment Test; HIT-6: Headache Impact Test; STAI: State/Trait Anxiety Inventory. *p<0.05; **p<0.001.
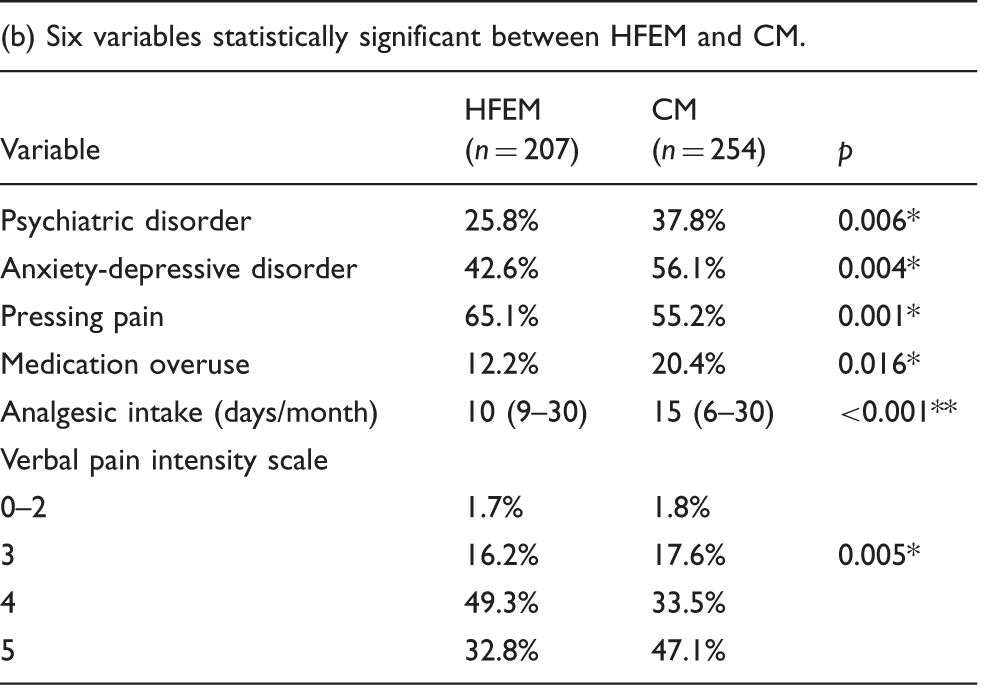
In order to study differences in groups depending on the number of headache days per month, we also performed a comparison between LFEM, HFEM and CM. The univariate analysis showed 15 significant differences, from 57 variables assessed, when LFEM and HFEM were compared against each other. In contrast, only six variables were statistically significant when HFEM and CM were compared (see Table 4a and Table 4b). When disability and impact of life variables were assessed, a positive relationship was found between headache frequency and a worsening of MIDAS, HIT-6, STAI and BDI scales. Strikingly HFEM and CM showed similar distribution in the categories of the MIDAS and STAI scales (p < 0.001) (see Figure 1).
Disability (a), impact on quality of life (b), anxiety (c) and depression (d) assessment when comparing LFEM, HFEM and CM. Clinically significant differences between LFEM and HFEM. LFEM: low-frequency episodic migraine; HFEM: high-frequency episodic migraine; MIDAS: Migraine Disability Assessment Test; BDI: Beck Depression Inventory; STAI: State/Trait Anxiety Inventory. *p<0.05; **p<0.001. Clinically significant differences between HFEM and CM. LFEM: low-frequency episodic migraine; HFEM: high-frequency episodic migraine; MIDAS: Migraine Disability Assessment Test; BDI: Beck Depression Inventory; STAI: State/Trait Anxiety Inventory. *p<0.05; **p<0.001.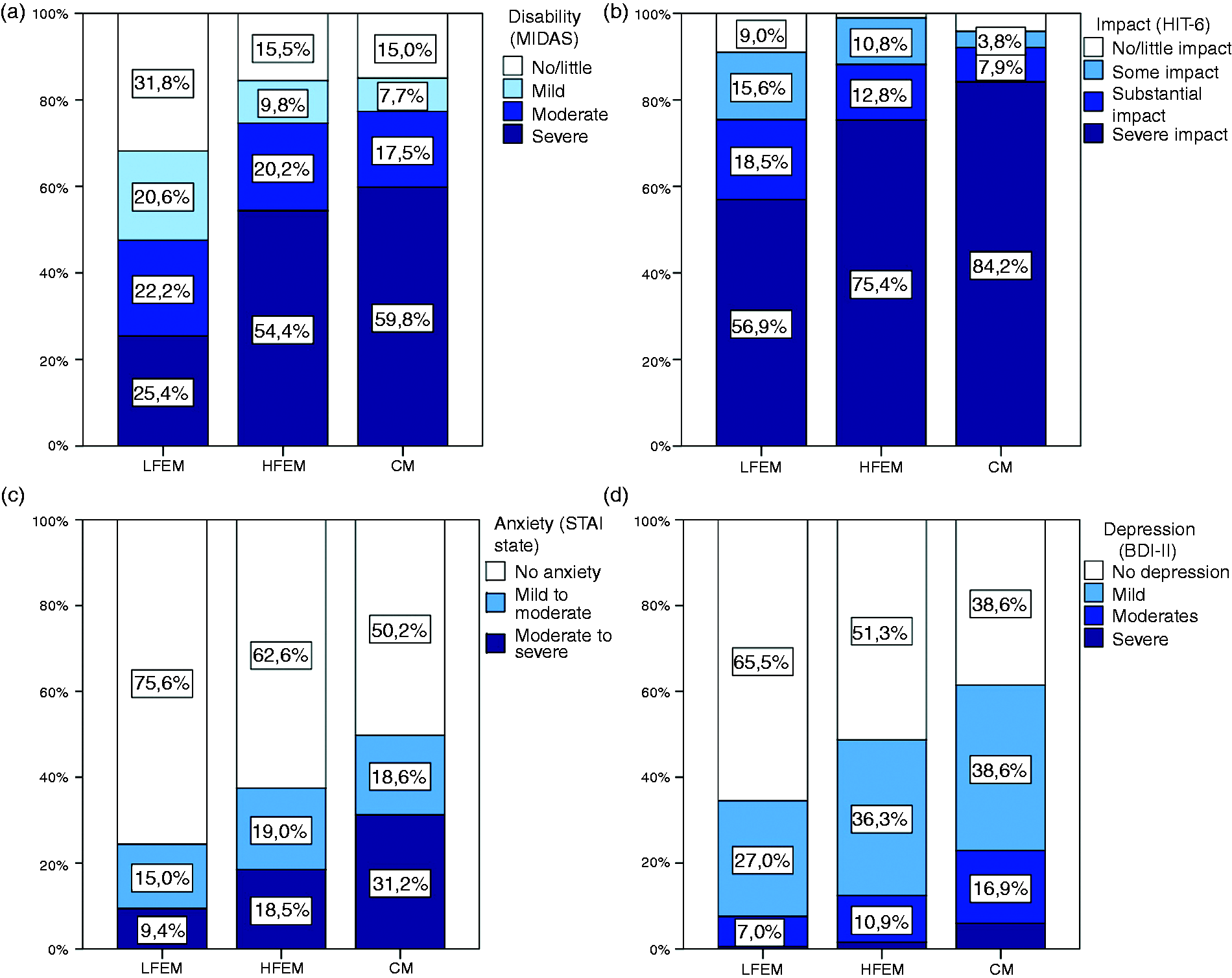

Based on the understanding that there are few statistically significant differences regarding clinical characteristics between HFEM and CM, we intended to construct a new model to better classify patients according to disability. We explored which was the best number of headache days cut-off point for different variables analysed and found that for disability and quality-of-life variables these cut-off points were quite variable. For instance, five or more headache days/month better differentiates patients with severe involvement in MIDAS (Se 86.5%, Sp 50.0%; J = 0.356), HIT-6 scale (Se 75.9%, Sp 59.1%; J = 0.350); and seven headache days/month for STAI trait (Se 70.9%, Sp 51.9%, J = 0.228). On the other hand, higher numbers of headache days are needed to differentiate moderate to severe involvement in anxiety and depression scales: 13 or more days for the STAI state scale (Se 57.6%, Sp 73.0%; J = 0.306) or 15 or more headache days for the BDI-II scale (Se 41.0%, Sp 80.8%; J = 0.218).
Cut-off points of headache days/month.

MIDAS: Migraine Disability Assessment Test; BDI: Beck Depression Inventory; HIT-6: Headache Impact Test; STAI: State/Trait Anxiety Inventory; J: Youden index.
Discussion
Migraine is considered to be a brain disorder which clinically presents with episodic attacks and potential for progression. Headache attacks can increase in frequency, transforming into daily or nearly daily headache over time (6). The definition of CM has evolved over the years but it has always appeared rather ambiguous. Since the first diagnostic criteria for CM were introduced in ICHD-2 (4), 15 headache days per month has been taken as the limit between episodic and chronic migraine. Based on 15 days as the cut-off value, EM and CM have been characterised in many population studies, and significant clinical differences were noticed between both groups (10,13,14).
This study about clinical profiles in patients with migraine based on headache frequency had the following main findings. First, our study replicates previous described clinical differences between CM and EM. Second, patients suffering from 10 or more headache days per month (HFEM) are closer to CM than to those who suffer from fewer than 10 headache days per month (LFEM). Third, the relationship between headache frequency and headache-related disability and impact on daily life is not linear, so participants suffering from 10 or more headache days per month showed similar emotional and functional disabilities as those with CM.
Our results confirm clinical differences between CM and EM. CM patients show a higher prevalence of anxiety-depressive disorder (15,16), sleep disorders (17), used more acute medication (18) and suffer from allodynia more frequently (19). When we compare CM and EM patients, those suffering from CM also presented poorer outcomes regarding the headache-related disability and impact on daily life (10,11,20).
However, contrary to previous findings, CM patients of our sample did not show higher rates of obesity. CM and EM patients have similar mean BMI and, when we sorted individuals by BMI categories, both groups showed similar prevalence of being normoweight. But surprisingly, obesity prevalence (BMI > 30) was lower in CM patients. Only 8.4% of CM patients had obesity. This prevalence is lower than other studies which tend to explore the relationship between obesity and migraine (21) and is also lower than the one found in Spain (22).
Another interesting finding is related to acute medication use. In our sample, medication overuse rates were found to be significantly different between three migraine groups. On one hand, it is reasonable to think that acute medication intake increases when headache is more frequent. Accordingly, the vast majority of patients with CM who take analgesics fulfil criteria for medication-overuse headache (MOH). But in our sample only 20.4% of patients with CM fulfil criteria for MOH with 15 mean monthly days of exposure to analgesics. These ratios are similar to previous studies (19,23). But, on the other hand, it is also known that overusing certain medications such as opioids or barbiturates can be independently associated with, or can help to perpetuate headache chronification (18). In our study, the use of these types of medications was uncommon, and the majority of patients took NSAIDs, triptans or ergotamine-containing medications. These data made us think that medication overuse could be one of the many risk factors for chronification. However, given that the main goal of our study was not to evaluate analgesic overuse, we are not able to establish the cause and effect of this relationship.
The main aim of this study was to assess differences in 57 variables depending on headache frequency. Based on the proposal by Bigal and Lipton (6), we performed a univariant analysis comparing participants with LFEM, HFEM and CM. CM and HFEM showed differences in only six categories which included more intense attacks and pressing pain, psychiatric comorbidities and a higher use of analgesics. We found it important to highlight that there were no significant differences on variables that evaluate emotional and functional disability between CM and HFEM.
Many epidemiological studies focusing on clinical differences between CM and EM had already been published; however, only a few studies have explored the influence of headache frequency (determined by headache days per month) on previously mentioned items. Although there is a tendency for patients with the very lowest frequencies to show less disability, this tendency is not linear. This means that having reached a certain level, those with higher frequencies show similar emotional and functional disabilities, affective distress and depression scores (24). For instance, there is a study that explores the relationship between the frequency and headache intensity with MIDAS and HIT-6 scales and it shows a non-monotonic relationship, that is, similar MIDAS scores from more than 37 headache days/3 months while HIT-6 was similarly affected by more than 8 headache days/3 months (25). Regarding association between depression and anxiety disorders, a significant strong linear trend of higher-prevalence odds ratios with increasing headache frequency (15) has also been shown.
Based on these findings, we performed a multivariant logistic regression with variables related with functional and emotional disability as MIDAS, HIT-6, STAI and BDI-II questionnaires. Despite the fact that the best cut-off points of frequency for each variable could be quite different, it seemed that the cut-off point for HFEM (≥10 headache days) could be a good option to better classify patients according to emotional and functional disabilities.
Further research is needed to classify more accurately migraine patients in order to unify diagnostic and therapeutic strategies. In addition to clinical features, molecular biomarkers have also been investigated to differentiate CM from EM. Data from human studies have begun to identify genetic mutations/polymorphisms and altered levels of specific proinflammatory and neuromodulatory molecules that may correlate with CM. For instance, increased levels of calcitonin gene-related peptide (CGRP) have been found in CM compared with EM or healthy controls (26). Epigenetic mechanisms may also be involved in the development of migraine so future studies in this field would provide further potential biomarkers for CM. All of these studies will help us differentiate biologic and genetic differences between the disorders in the future.
This study has several limitations. First, in contrast to the majority of previous studies that are based on surveys, our data collection was made in person by a headache specialist as it was conducted at a specialised headache unit. Because of this fact, our cohort includes a higher proportion (22.9%) of CM patients compared with survey-based studies. This makes our CM cohort larger and more detailed than other single-centred studies. Our cohort has the limitation of not reflecting what is encountered in primary care settings or general neurology outpatient clinics. Second, unmeasured or unknown confounders may have influenced the results. We have expressed migraine using frequency categories instead of expressing it in linear headache days, even if the initial analysis was performed considering it a continuum. Finally, this is not a longitudinal study, and we did not assess the same individual over different periods of time confirming the diagnosis using a calendar. A couple of strengths of our study are the large sample size and the analysis which has been made considering the number of headache days, not only by differentiating between EM and CM patients.
This study supports previous evidence that clinical characteristics of CM patients differ from EM patients. It seems that there is a clear difference that is easily recognised by headache specialists, but the cut-off point that better defines these clinical differences has never been explored. In our study, HFEM patients are as disabled as those diagnosed with CM. Consequently, we encourage neurologists and headache specialists to consider the emotional and functional impact of HFEM patients, as it could be as important as in CM patients, and to take 10 or more headache days per month as the threshold for substantial impact on daily life. A mind shift may allow us not only to define CM and its subsequent disability, but also to recognise those patients who are already disabled and prevent them from evolving to CM, offering them perhaps other therapeutic options. Remission to episodic migraine has been negatively associated with baseline headache frequency (8), so it is likely that the sooner we intensify the migraine treatment, the better remission rates we will obtain and future costs may be avoided.
Conclusions
EM and CM patients show significant differences regarding clinical presentation but especially when disability and quality of life are assessed. When a group differentiation is made following headache frequency, patients who suffer from 10 to 15 headache days per month have practically no differences compared with CM patients but, in contrast, both groups have many differences compared with LFEM patients. That led us to rethink the concept of when to consider a migraineur to be chronic as we might not be offering HFEM patients some interesting therapeutic options or considerations that might benefit and/or help them to improve.
Article highlights
Patients with 10 or more headache days per month have practically no clinical differences compared with chronic migraine (CM) patients. Similar to CM patients, high-frequency episodic migraine (HFEM) patients show poor outcomes in functional and emotional disability. HFEM patients are highly disabled, thus all therapeutic options should be considered.
Footnotes
Acknowledgments
PPR and JFM made substantial contributions to the conception, design and acquisition of the data. MQL contributed to the analysis and interpretation of the data. MTF wrote the first draft. PPR and JAS critically revised and finally approved the version to be published. All authors fully agree with and approved the version to be published.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Institute of Health Carlos III, Spanish Ministry of Economy and Competitiveness (PI10/00876), and the Fundació La Marato TV3 (072310).