
Abstract
Objective:
Despite the high prevalence and disabling nature of migraine, studies evaluating its economic burden in Singapore remain scant. This study aims to quantify the per capita and aggregate economic cost of episodic migraine (EM; ≤14 monthly headache days) without aura among full-time employees in Singapore.
Methods:
We administered a cross-sectional online survey to full-time employees in Singapore who met the International Classification of Headache Disorders (third edition, 2018) criteria for EM without aura. Eligible participants were classified by the frequency of monthly migraine days (MMDs): lower end episodic migraine (LEM; ≤3 MMDs) and upper end episodic migraine (UEM; 4–14 MMDs). The survey captured per capita healthcare resource utilization and lost work productivity (absenteeism and presenteeism) for each subgroup. Healthcare costs were obtained by multiplying unit costs by healthcare utilization. Finally, per capita (patient) costs of each subgroup were then imputed and multiplied by prevalence data to quantify the aggregate burden of migraine in Singapore.
Results:
Of the 606 participants who completed the survey, 81% experienced ≤3 MMDs. Total annual per capita costs were SGD4925 (USD 3620; 95% confidence interval (CI): SGD 4438–5411) and SGD14,476 (USD 10,639; 95% CI: SGD 11,908–17,045) for the LEM and UEM subgroup, respectively. Healthcare costs on average accounted for 17.6% of per capita costs, of which was driven primarily by diagnostic tests (33.6%), followed by consultations (17.1%), medications (16.7%), alternative medications (16.6%) and hospitalizations (14.8%). Lost productivity accounted for 82.4% of costs, chiefly attributable to absenteeism in the LEM group (38.2%), followed by presenteeism in the UEM group (26.0%), absenteeism in the UEM group (18.8%) and presenteeism in the LEM group (17.1%). The total cost to Singapore for EM in 2018 was approximately SGD 1 billion (USD 0.75 billion; SGD 1.00 = USD 0.74).
Conclusion:
Overall, EM imposes a substantial economic burden on society in Singapore. Total migraine cost per capita is greater in the UEM (4–14 MMDs) as compared to the LEM subgroup. Majority of the overall costs result from missed workdays and lost work productivity. Future research should determine the extent to which optimized migraine treatments could improve productivity, and by extension, mitigate the staggering costs of this disorder.
Keywords
Introduction
Migraine is a disabling neurological disorder characterized by unilateral, throbbing headaches of moderate-to-severe intensity that typically lasts between 4 h and 72 h. It is often accompanied by non-painful symptoms such as nausea, vomiting, photophobia, phonophobia and movement sensitivity. 1 Migraine patients are clinically categorized based on the frequency of headaches, as measured by monthly headache days (MHDs). Episodic migraine (EM) is defined as less than or equal to 14 headache days per month, whereas chronic migraine (CM) refers to 15 or more headache days per month for more than 3 months, and with features of migraine on at least 8 days per month. 1
Despite affecting approximately 1.04 billion people globally, migraine is often underdiagnosed and undertreated. 2,3 Acute treatment typically involves the use of over-the-counter (e.g. paracetamol) or prescription-medication (e.g. triptans or ergotamine derivatives) to alleviate migraine symptoms when they occur. On the other hand, preventive medications aim to reduce the frequency and severity of migraine attacks, especially in patients with EM who have disabling attacks or are frequently taking acute medications. 4 However, previous studies have revealed poor adherence and persistence to these routinely prescribed oral preventives. 5,6 Recently, calcitonin gene-related peptide monoclonal antibodies, a new class of preventives designed specifically for migraine, has been added to the treatment armamentarium. 4,7 –10
Migraine ranks as the second most burdensome disease worldwide in terms of years lived with disability (YLDs). 11 This burden further translates into economic losses due to increased healthcare costs and lost productivity due to absenteeism (i.e. missed workdays) and presenteeism (i.e. being less productive while working). 12 –19 In Asia, where the prevalence of migraine ranges from 11.3% to 14.4% in women and from 3.6% to 6.7% in men, studies have found that 65% of employees with migraines missed work due to the disorder and incur annual healthcare costs exceeding USD 1200 per capita per year. 20 –25
Uncovering the economic burden of migraine will raise awareness amongst healthcare providers, policymakers and employers to take timely action to mitigate the health and economic burden of the disorder through increased prioritization and resource allocation. To date, no study has attempted to quantify the per capita and aggregate economic burden of migraine among working adults in Singapore, a city-state in Asia with an advanced healthcare system. 26 The World Health Organization has expressed that the burden of headaches should be addressed as a matter of public health priority. 27
This study quantifies the economic cost of EM (≤14 monthly headache days) without aura among full-time employees in Singapore overall and separately by severity based on monthly migraine days (MMDs). We report costs for those with less than 3 MMDs (termed lower end episodic migraine (LEM)) and those with 4–14 MMDs (termed upper end episodic migraine (UEM)). We exclude CM sufferers with greater than 14 MMDS as these account for less than 1% of the total migraine population, are less likely to participate in the workforce amid due to their debilitating condition, and because they are less likely to participate in a web panel, which is the source of data for this effort. 14,25,28 –30
Methods
We administered an online survey to full-time Singaporean employees to quantify medical, absenteeism and presenteeism costs for EM sufferers. Potential participants were identified and recruited from an established web panel between June and September 2018. Invitations with a survey link were sent to an existing repository of panellists who were suffering from headaches and who have indicated their willingness to participate in online surveys. A round of reminders was sent to panellists who did not respond to the initial invitation. Upon agreeing to participate in the study through an opt-in button as a proxy for informed consent, panellists answered a short screener to determine eligibility (Online Appendix 1). Participants were eligible for inclusion in the study if they (i) were over the age of 21, (ii) were non-pregnant (iii), were Singaporean citizens or Permanent Residents, (iv) were full-time employees or self-employed workers, that is, working at least 35 h per week, (v) had at least two headaches not related to head injury or excessive alcohol consumption in the last year and (vi) fulfilled the International Classification of Headache Disorders (third edition) 3.1.1 criteria for migraine without aura. 1 Participants who failed quality checks during the survey, such as validation of internet protocol (IP) address and unique machine identifier (ID), logic checks, and identical answers to repeat questions, were dropped from the study. Twenty-five per cent of the panel sample was re-contacted to verify responses to four migraine-specific questions. Participants who completed the survey were compensated either with panel points or vouchers.
All eligible respondents reported demographic information including their ethnicity, marital status, education level, occupation and monthly employment income (Online Appendix 1). Additionally, they indicated their co-morbid conditions and their health-related quality of life as assessed by the EuroQoL-5 Dimensions (EQ-5D) questionnaire. The EQ-5D 5-L is a validated and widely used survey instrument that measures health in five dimensions, including mobility, self-care, usual activities, pain or discomfort, and anxiety or depression. 31
To collect data pertaining to the characteristics of migraine attacks experienced by respondents over the previous 3 months before the survey, they were asked about the duration of their previous attacks and responded to the 4-item Migraine Severity Questionnaire (MIGSEV). MIGSEV is an instrument that assesses the severity of migraine attacks as being mild, moderate or severe, based on the parameters of nausea, intensity of pain, tolerability and disability in daily activity. It is a validated instrument with good metrological properties and has been used in several studies to measure the intensity of migraine attacks. 19,32 –36 Participants in the study were classified into two subgroups based on the reported number of days affected by migraine in the previous month: LEM (≤3 days) and UEM (4–14 days).
To quantify direct medical costs, participants were asked about the frequency of healthcare resources consumed for the treatment of their migraines. Using checklists, we inquired about the type and frequency of physician visits, diagnostic tests, hospitalizations, visits to the emergency department (ED) and the total out-of-pocket expenditure on alternative treatments (Online Appendix Tables 2A, 2B and 3). All questions were asked with the frame ‘due to migraine’ to ensure that only costs directly associated with migraine were captured. A recall period of 3 months was chosen, modelled after the previous burden of migraine studies. 25,37 The only exception was the reporting of ED visits and hospitalization days, wherein a recall period of 12 months was selected due to the infrequency of their expected occurrence. Respondents also reported any medications taken to treat their migraine by selecting medications from a clinician-approved checklist of common migraine medicines. If the participant’s medication was not listed, they could indicate this as well.
Healthcare costs were calculated by multiplying the frequency of utilization by non-subsidized unit costs as reported in publicly available sources such as polyclinics, pharmacies and healthcare institutions (Online Appendix Tables 2A and 2B) and then averaged. This allowed for quantifying average costs across all participants based on self-reported healthcare. However, in the case of lumbar puncture tests and naratriptan, only data from the private sector were available. Since migraine medication was recorded for a checklist, it was not feasible to get full details on the dosage consumed, medication adherence or efficacy. Hence, the following assumptions were made: a 31% annual adherence rate for preventive medication and a standard initial dose on migraine days for acute medication. 38 The costs calculated for 3 months were then annualized to quantify the healthcare costs per capita due to migraine for the year. Per capita (patient) costs of each subgroup were then imputed and multiplied by prevalence data to quantify the aggregate burden of migraine in Singapore.
A modified 6-item Work Productivity and Activity Impairment Questionnaire: Specific Health Problem v2 (WPAI) was used to measure lost work productivity in terms of absenteeism and presenteeism. 39 Given the episodic nature of migraines, the investigators deemed it more suitable to have a recall period of 1 month instead of the instrument’s original recall period of 7 days despite greater potential for recall bias. Hence, all the questions in this section were asked relating to ‘the last month’. To capture absenteeism from work, respondents were asked to report the number of hours missed from work in the last month because of problems associated with their migraine. This figure was converted to days missed per year, assuming 8-h workdays and 250 workdays per year (accounting for 2 weeks of annual leave). Subsequently, migraine-related absenteeism was monetized by multiplying the number of missed workdays in a year by participants’ expected daily income, as assigned by matching age- and occupation-specific median gross income, including employer Central Provident Fund contribution (a mandatory social security savings scheme in Singapore that is funded by the contributions of employers and employees) of full-time employed residents published by the Ministry of Manpower. 40 We used self-reported income for self-employed workers (39 participants) and agricultural and fishery workers (1 participant), for whom no other data were available.
Similarly, for presenteeism, participants indicated the degree to which migraine affected their productivity while working on a scale from 0 to 10, where 0 represents ‘no migraines and/or migraines had no effect on my work’ and 10 represents ‘migraines completely prevented me from working’. As recommended in the WPAI manual, the total productive time lost was calculated as the product of participants’ presenteeism scale response and the annual number of days at work with migraine. 39 Annual days at work with migraine were calculated using the following steps: First, we divided the average number of absenteeism hours due to migraine by eight to convert to days. Then, we subtracted this from MMDs to arrive at MMDs, excluding absenteeism days. Lastly, we multiplied MMDs excluding absenteeism days by the probability that the participant was at work on that day (0.71 assuming the participant works 5 days a week) to arrive at days at work with a migraine. This figure was further multiplied by participants’ expected daily income to provide the monetized value of days of productive work lost while the individual worked below capacity due to problems associated with their migraines.
Statistical analysis
To ensure responses were in a plausible range, participant responses that exceeded the maximum values for similar questions but for any type of condition, as reported in the US Medical Expenditure Panel Survey, were set to missing (two in total). 41 Similarly, two observations for hours missed from work due to migraine were labelled as missing due to responses lying outside the plausible range (well above the 99th percentile). One additional participant was removed from the analysis due to several implausible responses (e.g. 19 magnetic resonance imaging (MRI) scans, 20 biopsies and implausible body mass index values). The remaining participants were stratified into LEM and UEM sufferers to be comparable with other studies. 9,42
Total costs for each stratum were calculated as the product of per capita costs (healthcare costs and lost work productivity) and subgroup-specific migraine prevalence rates times the number of full-time employed residents in Singapore. 43 Prior to estimation, t-tests with unequal variances were employed to test whether unit costs within each migraine subgroup were statistically different (p value ≤ 0.05) by gender (male/female) and then within gender, by age category (21–39 years/40–65 years), with a minimum of 25 individuals per stratum. We applied the unit costs at the most granular level where statistically significant differences were found. All costs were reported in 2018 Singapore dollars (SGD 1.00 = USD 0.74).
Given that the survey was only fielded to individuals who had previously reported experiencing headaches, it could not be used for estimating the prevalence of migraine. Hence, the prevalence rates were drawn from existing literature. While there had been a prior study which captured the prevalence of migraine in Singapore, its inclusion criterion required that the primary headache lasted for at least 4 h irrespective of treatment. 26 Due to this requirement, it is likely that the prevalence reported by the study is an underestimate because many migraine sufferers take medication upon the onset of an attack, resulting in a shorter headache duration and by extension, exclusion from the study. 44 For this reason, other studies consider migraine attacks to last 2–4 h with medication and at least 4 h otherwise. 45,46 These estimates tend to reveal higher prevalence rates. Therefore, instead of using the prevalence rates available for Singapore, this study employed prevalence data obtained from a study in Taipei, given that their definition of migraine is more consistent with ours and it is unlikely that the prevalence of migraine would differ greatly between the two cities. 46
However, the prevalence estimates from Taipei required certain adjustments for application in our study. The Taipei study reported age- and gender-segregated migraine prevalence (for both migraine with and without aura), whereas we required age, gender and LEM/UEM subgroups for migraine without aura only. Therefore, the following steps were taken to obtain the desired prevalence rates. First, the total age- and gender-segregated migraine prevalence from Taipei (average ∼9.6%) was divided into EM and CM prevalence rates by subtracting an estimated prevalence of CM (0.6%) from the total to result in an EM prevalence of 9.0%. 28 To further reduce the prevalence to only account for migraine without aura, the EM prevalence rate (9.0%) was multiplied by 0.88, the proportion of migraine sufferers with migraine without aura, resulting in a total prevalence of 7.9% for EM without aura. 46 Lastly, since the total prevalence for EM includes both frequency LEM and UEM subgroups the reported number of MMDs from our survey was used to stratify the prevalence rates for respective subgroups. Since the LEM group represented 80% of the panel, the total EM without aura prevalence rate (7.9%) was multiplied by 0.8 to estimate a prevalence of 6.3% for this subgroup. Likewise, for the UEM subgroup, the total EM without aura prevalence rate was multiplied by 0.2 to yield a prevalence of 1.6%.
Results
The recruitment flow and eligibility of study participants are shown in Figure 1. A total of 13,284 panellists were invited to participate in the study, of whom 10.8% (n = 1430) met the inclusion criteria. Approximately 42.3% (n = 606) of eligible respondents completed the survey and were included in the analysis set; 49% were female. Based on the number of MMDs reported for the previous month, 81% of respondents (n = 492) were LEM sufferers, while the remaining 19% (n = 114) were UEM.
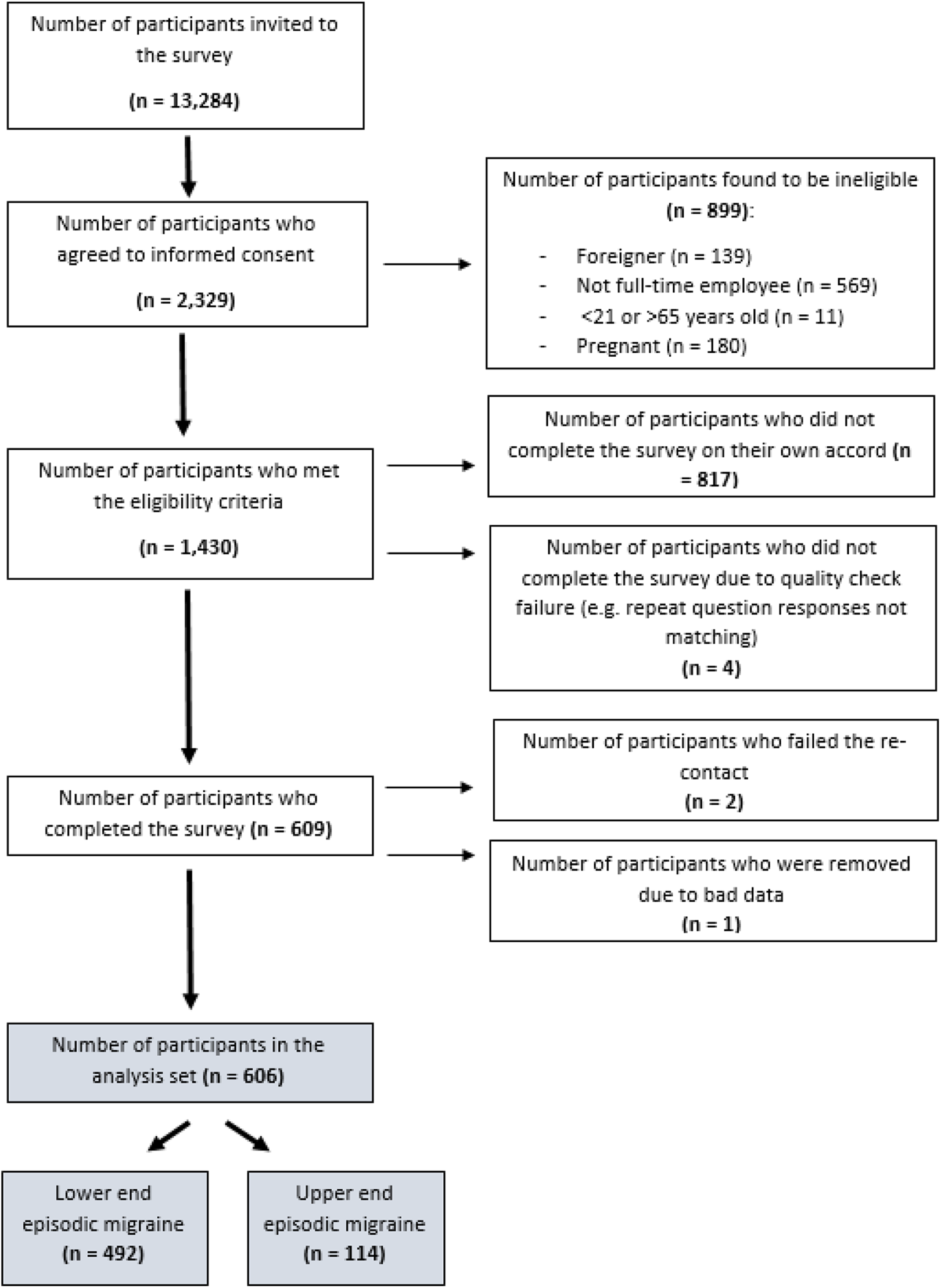
Subject enrolment, inclusion and exclusion diagram.
The demographic information and migraine characteristics of the study sample are reported in Table 1, stratified by migraine frequency. Participants were, on average, 38 years old and were primarily of Chinese descent (84.8%), married (68.3%) and had completed at least tertiary education (58.6%). With regard to migraine characteristics, the duration of the last migraine attack was similar across subgroups, whereas a higher proportion of UEM participants scored intermediate and high MIGSEV grades as compared to LEM participants.
Characteristics of subjects.

LEM: lower end episodic migraine; UEM: upper end episodic migraine; MMDs: monthly migraine days; SD: standard deviation; ITE: Institute of Technical Education; GCE: General Certificate of Education; HDB: Housing & Development Board; JTC: Jurong Town Corporation; MIGSEV: Migraine Severity Questionnaire.
a The Singapore-Cambridge GCE Ordinary Level (O level) examination is a national examination held annually in Singapore. The examination is taken by secondary school students at the end of their fourth (for Express Stream) or fifth year (for Normal Academic Stream) and is open to private candidates.
b The ITE is a public vocational education institution agency in Singapore that provides pre-employment training to secondary school graduates and continuing education and training to working adults.
c The Singapore-Cambridge GCE Advanced Level (A level) is a national examination held annually in Singapore. The examination is taken by school candidates upon the completion of pre-university education at junior colleges, centralized institutions and Integrated Programmed, and is also open to private candidates.
d The HDB is the statutory board of the Ministry of National Development responsible for public housing in Singapore.
e JTC is a Singaporean state-owned real estate company and statutory board under the Ministry of Trade and Industry.
f The MIGSEV questionnaire is a validated, reliable and widely used survey that assesses the severity of individual migraine attacks based on four parameters: intensity of pain, disability in daily activities, tolerability and nausea.
Figure 2 illustrates the healthcare expenditure, presenteeism and absenteeism costs per capita, associated with each migraine subgroup. The largest single contributor to healthcare is diagnostic tests (33.6%) with MRIs being the most expensive driver (48.8%), followed by consultations (17.1%) with the bulk of costs attributed to general practitioner visits (68.4%), medications (16.7%) with acute treatment (95.5%) making up the majority, alternative medications (16.6%) and then hospitalizations (14.8%). These percentages were obtained by averaging the LEM/UEM healthcare unit costs. The more significant source of cost was attributable to lost work productivity, which accounted for 81% of migraine costs per capita. Total per capita costs were SGD 4925 (USD 3645; 95% confidence interval (CI): SGD 4438–5411; USD 3284–4004) for LEM and SGD 14,476 (USD 10,712; 95% CI: SGD 11,908–17,045; USD 8812–12,613) for UEM. Healthcare unit costs totalled SGD 1016 (USD 752; 95% CI: SGD 757–1276; USD 560–944) and SGD 2399 (USD 1775; 95% CI: SGD 1293–3504; USD 957–2593) for LEM and UEM subgroups, respectively, which was less than 25% of the total unit costs for each group.
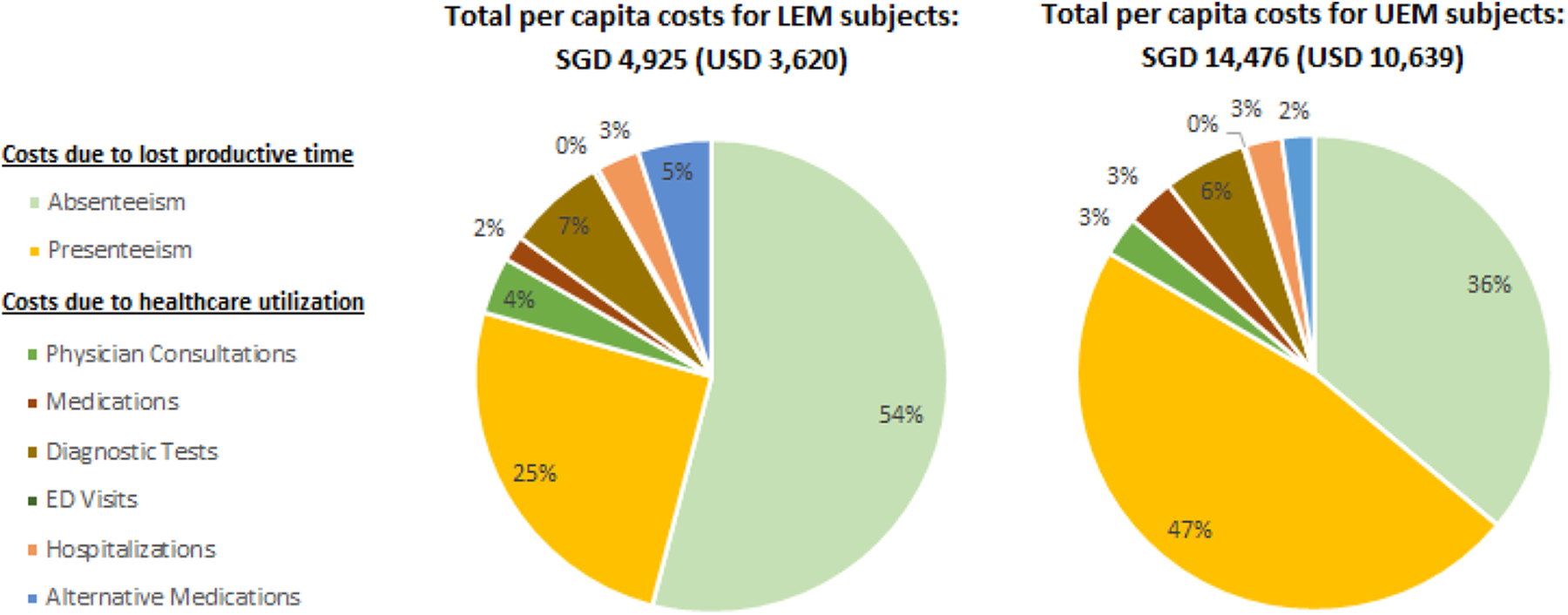
Breakdown of per capita costs for each subgroup.
Annual absenteeism costs per capita were substantially higher for UEM participants at SGD 5216 (USD 3860; 95% CI: SGD 3271–7160; USD 2421–5298) as compared to SGD 2661 (USD 1969; 95% CI: SGD 2307–3016; USD 1707–2232) for LEM participants. Similarly, annual presenteeism per capita costs were SGD 6862 (USD 5078; 95% CI: SGD 5894–7830; USD 4362–5794) for UEM and SGD 1247 (USD 923; 95% CI: SGD 1099–1395; USD 813–1032) for LEM. Absenteeism accounted for over half of total costs for the LEM subgroup and presenteeism for just under half of all costs for the UEM subgroup. The detailed breakdown of unit cost estimates for each healthcare resource utilization and lost productivity are available in Online Appendix Tables 3 and 4. Table 2 displays age- and gender-specific unit costs for healthcare utilization, which encapsulates diagnostic tests, medications, alternative medications, consultations and hospitalizations. It also displays absenteeism, presenteeism and total per capita costs. Among older UEM participants, the healthcare costs incurred by males was over four times that of females (p = 0.04) and over twice for younger LEM patients (p = 0.005). Presenteeism costs for younger female participants were two-thirds and over half that of younger males within LEM and UEM subgroups, respectively (p ≤ 0.01). Upon multiplying the total unit costs with the corresponding prevalence and population estimates, migraine costs among full-time employees in Singapore were estimated to be SGD 1 billion (USD 0.75 billion; SGD 1.00 = USD 0.74; Table 3).
Unit costs due to migraine.
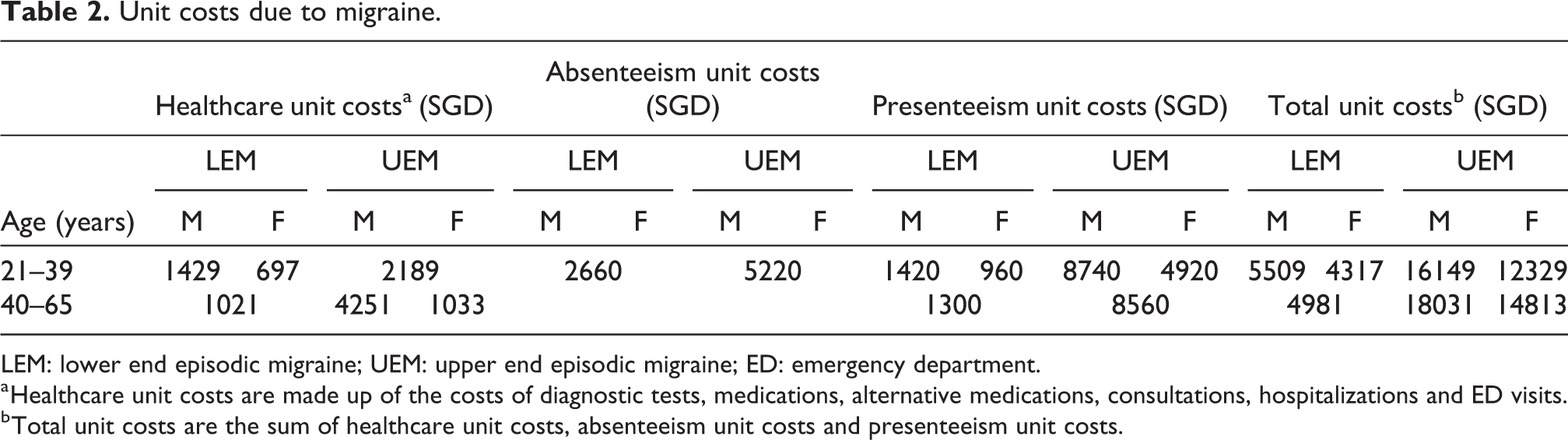
LEM: lower end episodic migraine; UEM: upper end episodic migraine; ED: emergency department.
a Healthcare unit costs are made up of the costs of diagnostic tests, medications, alternative medications, consultations, hospitalizations and ED visits.
b Total unit costs are the sum of healthcare unit costs, absenteeism unit costs and presenteeism unit costs.
Total costs due to migraine for Singapore based on number of employed residents and prevalence rates.
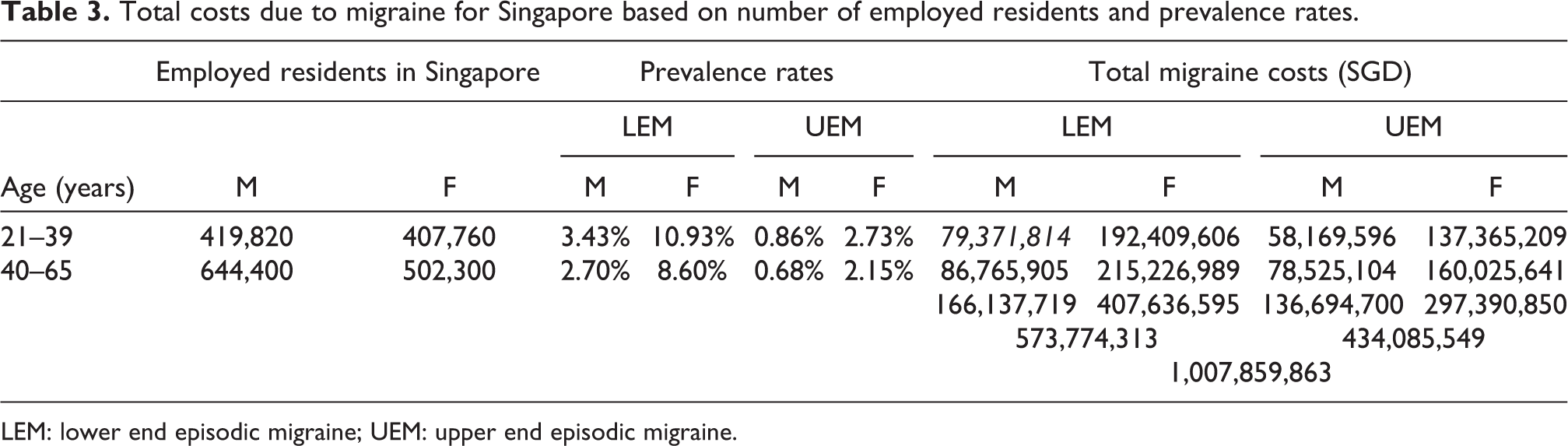
LEM: lower end episodic migraine; UEM: upper end episodic migraine.
Discussion
This cross-sectional web-based survey aimed to estimate the annual economic burden of EM without aura among full-time employees in Singapore. It focused on three measures of burden: medical expenditure, absenteeism and the value of lost productivity while working (presenteeism). Aggregating costs across the three parameters generated a total economic burden of SGD 1 billion (USD 0.75 billion; SGD 1.00 = USD 0.74) per year. Of this, annual healthcare expenditure directly associated with migraine amounted to SGD 175 million (USD 130 million; SGD 1.00 = USD 0.74), which represents approximately 2% of the total government healthcare expenditure in Singapore. 47 In contrast, YLDs attributable to migraine totalled to roughly 1% in Singapore, indicating that migraine disproportionately burdens the healthcare system relative to the YLDs it imposes. 48 Healthcare costs per capita were higher for the UEM subgroup because of the greater attack frequency and potentially more severe nature of attacks compared to those experiencing less frequent attacks. This study documents the costs of medical utilization but does not set out to determine the appropriateness of investigations for patients with migraines in Singapore as that is beyond the scope of this effort. However, there is a prevailing sentiment that many physicians over-investigate for fear of missing out a secondary aetiology despite no ‘red flags’ present. The study uncovered the significant healthcare cost attributable to investigations, highlighting the need for better education amongst physicians to ‘choose wisely’.
Consistent with data from other countries, the costs generated due to lost productivity accounted for the vast majority (roughly 83%) of the total burden of migraine for both subgroups. 15,49 A study of European countries found that indirect costs made up the majority of the costs of migraine, of which two-thirds was attributed to productivity loss (49), while another study done in the United States found up to 69.6% of costs attributable to productivity loss. 15 Both absenteeism and presenteeism costs were higher in the UEM subgroup. However, in relative terms, the magnitude of the difference in presenteeism costs between the two subgroups (SGD 5615; USD 4155 per capita) was more than double the magnitude of the difference in absenteeism costs (SGD 2555; USD 1891 per capita). A possible explanation for this discrepancy could be that the federally mandated paid medical leave in Singapore, approximately 14 days per year, falls significantly short of the minimum (48) and median (60) number of migraine days that UEM sufferers experience. 50 It is unlikely that any workplace in Singapore would offer over this minimum amount. As a result, migraine sufferers in the UEM category would unlikely be able to take paid medical leave for the majority of their migraine attacks, resulting in considerable presenteeism costs.
Several prior studies have quantified the economic burden of migraine, either for migraine sufferers on average as a whole or segregated according to chronic and EM subtypes. Although drawing any comparisons is challenging due to the variation in healthcare systems, sample sizes, data types and study methodologies, the results revealed in this study are within the range of the estimates reported in other countries. 9,13 –15,23,25,37,42,51 The number of presenteeism days for EM sufferers reported in our study (7.4 days per year) is within the range of estimates provided in several studies (6–10 days per year), and the number of absenteeism days (9.8 days per year) is within the range of estimates (6.6–12 days per year) reported in a global study which surveyed countries across Europe, Latin America, North America and Australia. 51 However, the absenteeism estimates in this study are higher than the figures reported by individual studies in the United States and Taipei (1.8–3.2 days per year). 15,16,21
This study has several limitations. All surveys, either online or in-person, are susceptible to selection bias. If the characteristics of panel participants who responded to our survey differ from those of the general migraine population, then the cost estimates would be biased. We also find from the sample that among residents, more UEM sufferers are female relative to LEM sufferers and relative to the gender split in the population. Nonetheless, it is crucial to keep in mind that we use the survey data only to quantify unit costs, not for prevalence estimation, given that the survey is not meant to be representative of the population. As long as those represented are reflective of the typical patient, our unit cost estimates are unbiased. As with all cross-sectional surveys, this study may also suffer from self-report and recall bias, which may vary across survey dimensions. For example, the recall period for the MIGSEV includes past 3 months for number of migraines, past month for number of days affected and last migraine for severity. For medical expenditures, a recall period of 3 months was used with the exceptions of admissions and ED visits, where the period was extended to 12 months. For WPAI, the recall period was modified from ‘the last 7 days’ to the ‘last 4 weeks’ to account for the episodic nature of migraine. Measuring the influence of self-report and recall bias on the estimates should be an area of future research. Moreover, we were not able to capture information on whether patients had missed work for other reasons aside from migraine, health-related or not. This exacerbates the presenteeism for both groups of EM sufferers, but particularly the UEM group. We also multiplied the units of preventive medication consumed by an adherence rate of 31%. While this is a conservative estimate, adherence rates vary across individuals and are conditional on psychological, behavioural and health-related factors, in addition to the efficacy and side effects of the treatment. Additionally, our estimate of healthcare resource utilization and associated costs is conservative due to the exclusion of participants who could not recall the name of their medications and the diagnostic tests they had undertaken. In addition, we applied the lowest standard dose for the medication list provided. We estimated the prevalence of migraine based on a 2001 Taipei study rather than a Singapore study and applied assumptions of a classification between those experiencing ≤3 MMDs and those experiencing 4–14 MMDs, based on the data collected from the online panel. However, there is no evidence for a disparity in the prevalence of migraine between Taipei and Singapore, or for any change over time. 52,53 Finally, we did not include the burden incurred by non-full time employees, despite migraine being a common condition that affects all population subsets. Due to the disability imposed, individuals may have to work part-time or become unemployed, leaving the workforce altogether. We were also unable to quantify other costs of migraine, such as lost productivity at home, foregone leisure activities and costs associated with the stigma of suffering from migraines both at work and in home. Future studies should aim to estimate these costs for a more accurate and comprehensive burden estimate.
Despite the aforementioned limitations, our study demonstrates that migraine imposes a significant annual burden of approximately SGD 1 billion (USD 0.75 billion; SGD 1.00 = USD 0.74) in Singapore, primarily driven by losses in productivity. To put this figure into perspective, our estimate of the total burden of migraine among full-time employees is approximately 85% of costs for type 2 diabetes mellitus (inflated to 2018 SGD ) among the same population subset. 54 –57 Results further show that roughly a quarter of our subjects did not medically treat their condition, and those who did, generally use acute medication that may or may not be effective. This reveals that, despite the availability of new treatments, migraine remains an undertreated condition in Singapore. Based on the guidelines set by the American Migraine Prevalence and Prevention study, preventive medication should be considered if a sufferer experiences at least four MMDs with normal functioning or two MMDs with severe impairment. 4 According to our study, 21% of our sample, including those who are likely to account for the greatest burden, could benefit from more appropriate migraine treatment. If such treatment were made more accessible, it could possibly alleviate the disability caused by migraine and by extension translate into improved productivity and better quality of life. Testing the veracity of this hypothesis should be an area of future research in Singapore.
Public health relevance
Migraine imposes a substantial economic burden on society in Singapore, especially for those experiencing higher MMDs. Majority of the costs result from missed workdays (absenteeism) and lost work productivity (presenteeism). Future research should determine the extent to which optimized migraine treatments could improve productivity, and by extension, mitigate the staggering costs of this disorder.
Supplemental material
Supplemental Material, Appendix_1_R2 - Economic burden of migraine in Singapore
Supplemental Material, Appendix_1_R2 for Economic burden of migraine in Singapore by Jonathan Jia Yuan Ong, Devanshi Patnaik, Yee Cheun Chan, Oliver Simon and Eric A Finkelstein in Cephalalgia Reports
Supplemental material
Supplemental Material, Appendix_2a_R2 - Economic burden of migraine in Singapore
Supplemental Material, Appendix_2a_R2 for Economic burden of migraine in Singapore by Jonathan Jia Yuan Ong, Devanshi Patnaik, Yee Cheun Chan, Oliver Simon and Eric A Finkelstein in Cephalalgia Reports
Supplemental material
Supplemental Material, Appendix_2b_R2 - Economic burden of migraine in Singapore
Supplemental Material, Appendix_2b_R2 for Economic burden of migraine in Singapore by Jonathan Jia Yuan Ong, Devanshi Patnaik, Yee Cheun Chan, Oliver Simon and Eric A Finkelstein in Cephalalgia Reports
Supplemental material
Supplemental Material, Appendix_3_R2 - Economic burden of migraine in Singapore
Supplemental Material, Appendix_3_R2 for Economic burden of migraine in Singapore by Jonathan Jia Yuan Ong, Devanshi Patnaik, Yee Cheun Chan, Oliver Simon and Eric A Finkelstein in Cephalalgia Reports
Supplemental material
Supplemental Material, Appendix_4_R2 - Economic burden of migraine in Singapore
Supplemental Material, Appendix_4_R2 for Economic burden of migraine in Singapore by Jonathan Jia Yuan Ong, Devanshi Patnaik, Yee Cheun Chan, Oliver Simon and Eric A Finkelstein in Cephalalgia Reports
Footnotes
Acknowledgements
The authors wish to thank Stephen Christopher (former employee of Novartis) and Immanuel Tang (current employee of Novartis) for their contribution in the early conceptualization of this study, administrative coordination of this project and constructive feedback on the manuscript. Naina Verghese (former employee of Duke-NUS) is acknowledged for her contribution to administrative coordination of this project as well as contributions to writing of the manuscript. Cecilia Ow Yuet Onn (current employee of Duke-NUS) is acknowledged for her contribution to acquisition of data.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Eric A Finkelstein has received research grants and speaker fees from Novartis and other pharmaceutical companies. Devanshi Patnaik worked as an RA for Dr Finkelstein and reports no conflicts. Jonathan Jia Yuan Ong received speaker fees from Novartis Singapore Pte Ltd outside of the submitted work. He participated in Advisory Board meetings organized by Novartis and Eli Lilly. Yee Cheun Chan attended advisory boards organized by Novartis outside of the submitted work. Oliver Simon is an employee of Novartis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Novartis Singapore Pte. Ltd.
Institutional review board approval
Since this research involved direct participation by human subjects, the study was approved by the Institutional Review Board (IRB) at the National University of Singapore (NUS), Singapore under reference code S-18-176E. The requirement for written informed consent from all participating human subjects was waived by the IRB.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.