
Abstract
Introduction
Migraine is associated with comorbidities and greater healthcare resource utilization (HCRU). We investigated comorbidity rates and HCRU among Leumit Health Services (LHS) members diagnosed with migraine versus matched controls.
Methods
This electronic health record (EHR)-based retrospective study included adult LHS members with a migraine diagnosis between 2017 and 2022 (migraine cohort), and matched-controls drawn from the LHS EHR. HCRU was evaluated for 2022.
Results
The cohorts included 18,527 subjects each (both 78.7% female; mean age, 45.8 ± 14.8 years). Transient ischemic attacks (TIAs), cerebrovascular accidents (CVAs), and valvular disorders were more prevalent in the migraine cohort (TIA, 0.55% vs. 0.30%; CVA, 1.8% vs. 1.3%; valvular disorders, 2.8% vs. 1.8%; all P < 0.001), whereas myocardial infarction was less frequent (1.0% vs. 1.2%; P = 0.015). Hypertension was more prevalent (23.5% vs. 19.9%, P < 0.001), whereas diabetes (10.0% vs. 12.1%, P < 0.001) and chronic kidney disease (0.92% vs. 1.2%, P = 0.028) were less common. All evaluated inflammatory/autoimmune and pain-related/neurological disorders were significantly more prevalent among migraine patients; cancer rates were similar. HCRU was significantly greater among migraine patients, with higher proportions having ≥1 visit to a general practitioner (93.7% vs. 85.4%), neurologist (57.4% vs. 22.1%), pain specialist (12.0% vs. 3.4%), and the emergency department (17.3% vs. 11.2%) (all P < 0.001). Migraine patients were also more likely to request approval for sick days (28.0% vs. 15.7%, P < 0.001).
Conclusions
Compared to matched controls, migraine was associated with significantly higher rates of multiple comorbidities and substantially increased HCRU, reflecting both clinical and societal burden.
Background
Migraine, a very prevalent and potentially debilitating neurological disease, is often associated with comorbidities.1–3 These comorbidities include cardiovascular, inflammatory, neurological diseases, and pain syndromes. The presence of these comorbidities may adversely affect the overall treatment outcomes. 3 Understanding the association between migraine and their accompanying comorbidities could help elucidate their mechanistic links, which is important for developing effective treatment strategies for both migraine and the associated conditions. These mechanistic links have been proposed and investigated for numerous comorbidities. For example, the neuroinflammation implicated in migraine pathophysiology involves alterations of cytokine profiles (e.g. tumor necrosis factor-α and interleukin-1β). These alterations have been suggested to contribute to the increased predisposition of migraine patients to immunological diseases. 4
Across the world, studies have consistently demonstrated the heavy burden of migraine with respect to healthcare resource utilization (HCRU). Health economic analysis also showed the economic burden resulting from the disease, both directly (e.g. due to visits to medical professionals, treatments, and hospitalizations) and indirectly with productivity losses due to taking time off work, accounting for most of the indirect cost. 5 The cost-effectiveness of abortive and preventative migraine treatments was evaluated in a recent systematic review, which included studies in the USA as well as countries in Europe, Asia, and Africa. The study showed that these treatments were cost-effective in many health systems, particularly in high-income countries. 6
The current study investigated the comorbidity rates among members of Leumit Health Services (LHS) a national health maintenance organization in Israel serving approximately 730,000 members (roughly 7.5% of the country population). The LHS electronic health record (EHR) system was used to characterize LHS members with a clinically significant migraine between 2017 and 2022. That study found that in 2022, among adult LHS members, approximately 24,300 had a clinically significant migraine diagnosis, representing 5.2% of the adult members of LHS. 9 It compared individuals diagnosed with a clinically significant migraine (migraine cohort) compared to a matched control cohort without such a diagnosis (control cohort) and assessed the extent of HCRU in both cohorts.
Methods
Study design, data source, and patients
The study was approved by the institutional review board (IRB) of LHS (approval number: LEU 0008-23) and was granted a waiver for obtaining informed consent due to its retrospective design. The study was conducted in accordance with the Declaration of Helsinki.
LHS has been maintaining a centrally managed EHR system for over two decades, with person-level data including sociodemographic data, medical diagnoses, visits/consultations with LHS and LHS-affiliated medical professionals, hospital and emergency department (ED) admissions, medication prescription/purchases, and laboratory results. The demographic composition of the LHS reflects that of Israel, with slight overrepresentations of medium-to-low socioeconomic (SES) status groups and certain minority populations, including Arabs and Ultra-Orthodox Jews.
This retrospective observational cohort study included all current/former LHS members who had a diagnosis of migraine between 2017 and 2022, were ≥18 years, and had an active LHS membership during the year under consideration, alongside a matched control. LHS members were included in the migraine cohort of the study if at least one of the following four criteria were met: having ≥2 documented instances of migraine as a diagnosis in an outpatient setting; having a record of the International Classification of Disease, 9th Edition Clinical (ICD-9) code for migraine in a hospital or ED discharge; a migraine diagnosis by a board-certified neurologist; or a purchase of migraine-specific therapeutics (i.e. triptans, calcitonin gene-related peptide (CGRP) inhibitors). The matched control cohort (1:1) consisted of LHS members without a migraine diagnosis, drawn from the EHR system of LHS. The matching was based on age, sex, demographic group, and SES. No exclusion criteria were applied.
The EHR of LHS constituted the source of all data analyzed in the current study, including sociodemographic, comorbidities, and HCRU. Data extraction for the migraine and control cohorts was performed automatically using structured query language and Python scripts. All data were anonymized before the analysis.
Data for body mass index (BMI) and physical activity were documented by treating physicians or nurses during routine medical appointments. SES was determined according to the residential address of the LHS members. It is a scale from 1 (lowest SES) to 20 (highest SES), based on the Points Location Intelligence® database, which is highly correlated with SES measures provided by the Israeli Central Bureau of Statistics. The residential address was also used to classify the population into three demographic groups: the general population, Ultra-Orthodox Jews, and Arabs, using established methodologies. Comorbidities were assessed using the EHR-documented ICD-9 codes corresponding to each of the evaluated conditions up to the data extraction date.
HCRU was evaluated for the 2022 calendar year, measuring all encounters captured in the EHR for the migraine and control cohorts. For migraine patients who were diagnosed in 2022, the encounters captured for that patient and the matched control were from the diagnosis date through the end of 2022.
Statistical considerations
This retrospective observational study followed the STROBE reporting guidelines for cohort studies. Descriptive statistics were used to summarize demographic and clinical characteristics. The main variables were summarized as means and standard deviations (SD). Characteristics of the migraine and control cohorts were compared using Fisher's exact tests and two-sample t-tests for categorical and continuous variables, respectively. In addition, odds ratios (OR) and 95% confidence intervals (CI) were calculated. R version 4.4.1 was used for the analysis. 10 All tests were two-sided. The value P ≤ 0.05 was considered statistically significant.
Results
Study patients
Of the 24,311 subjects with a clinically significant migraine diagnosis in 2022, a total of 18,527 (76.2%) were successfully matched based on age, sex, demographic group, and SES. Thus, the migraine and control cohorts included 18,527 subjects each. The baseline demographic and clinical characteristics of these cohorts are presented in Table 1. The parameters used for selecting the matched controls (sex, age, demographic group, SES) were well-balanced between the cohorts. In both groups, the majority were females (78.7%), the mean age at data extraction was 45.8 (SD, 14.8) years, the mean SES was 8.8 (SD, 3.6), and the majority of subjects were categorized as the general population (63.8%). In other evaluated baseline parameters, some imbalances were noted. Specifically, the geographic distribution varied between the cohorts (the migraine cohort had more subjects from northern Israel and fewer subjects from the Jerusalem area). Additional statistically significant differences involved BMI with lower BMI in the migraine cohort compared to the control cohort (mean [SD] of 27.2 [5.6] vs. 27.6 [5.9] kg/m2, P < 0.001), and smoking status with more current smokers in the migraine versus the control cohort (20.4% vs. 19.1%, P = 0.03). No statistically significant differences between the cohorts were noted in the proportion of subjects not engaging in physical activity.
Baseline demographic and clinical characteristics of the migraine and control cohorts.

BMI: body mass index.
P values were determined using Fisher’s exact test and two-sample t-test for categorical and continuous variables, respectively. Bold font represents statistical significance. Socioeconomic status is based on a 1–20 scale.
Migraine and comorbidities
The prevalence of the evaluated comorbidities in the two cohorts and the corresponding OR (95% CI) values are presented in Table 2 and Figure 1. Within cardiovascular diseases, high OR values were reported for transient ischemic attacks (TIAs, prevalence of 0.55% vs. 0.30% for the migraine and control cohorts, respectively; OR, 1.84 [95% CI, 1.31–2.61], P < 0.001), and cerebrovascular accidents (CVAs, prevalence of 1.8% vs. 1.3%, respectively; OR, 1.42 [95% CI, 1.19–1.68], P < 0.001) despite a lower rate of diabetes (10.0% vs. 12.1%; OR, 0.81 [95% CI, 0.76–0.86], P < 0.001) and a similar activity level. The prevalence of hypertension was also higher in the migraine cohort (23.5% vs. 19.9%; OR, 1.23 [95% CI, 1.17–1.30], P < 0.001). The observed lower prevalence of diabetes correlates with the significantly lower rate of chronic kidney disease (CKD) in the migraine versus the control cohort (0.92% vs. 1.2%; OR, 0.79 [95% CI, 0.64–0.98], P = 0.028). Also, within cardiovascular diseases, the rate of myocardial infarction (MI) was significantly lower among the migraine cohort (1.0% vs. 1.2%; OR, 0.78 [95% CI, 0.64–0.95], P = 0.015). The rates of ischemic heart disease, congestive heart failure, and peripheral vascular disease were similar between the groups. Lastly, the rate of valvular disorders was significantly higher among the migraine cohort (2.8% vs. 1.8%; OR, 1.57 [95% CI, 1.37–1.81], P < 0.001). Notably, in a post-hoc analysis, the proportion of patients undergoing echocardiograms was also significantly higher among migraineurs compared to controls (46.0% vs. 32.3%; OR, 1.79 [95% CI, 1.71–1.87], P < 0.001).

Prevalence of reported comorbidities in the migraine and control cohorts. *P < 0.05, Fisher's exact test comparing the migraine cohort to the control cohort for each evaluated comorbidity.
Reported comorbidities in the migraine and control cohorts.
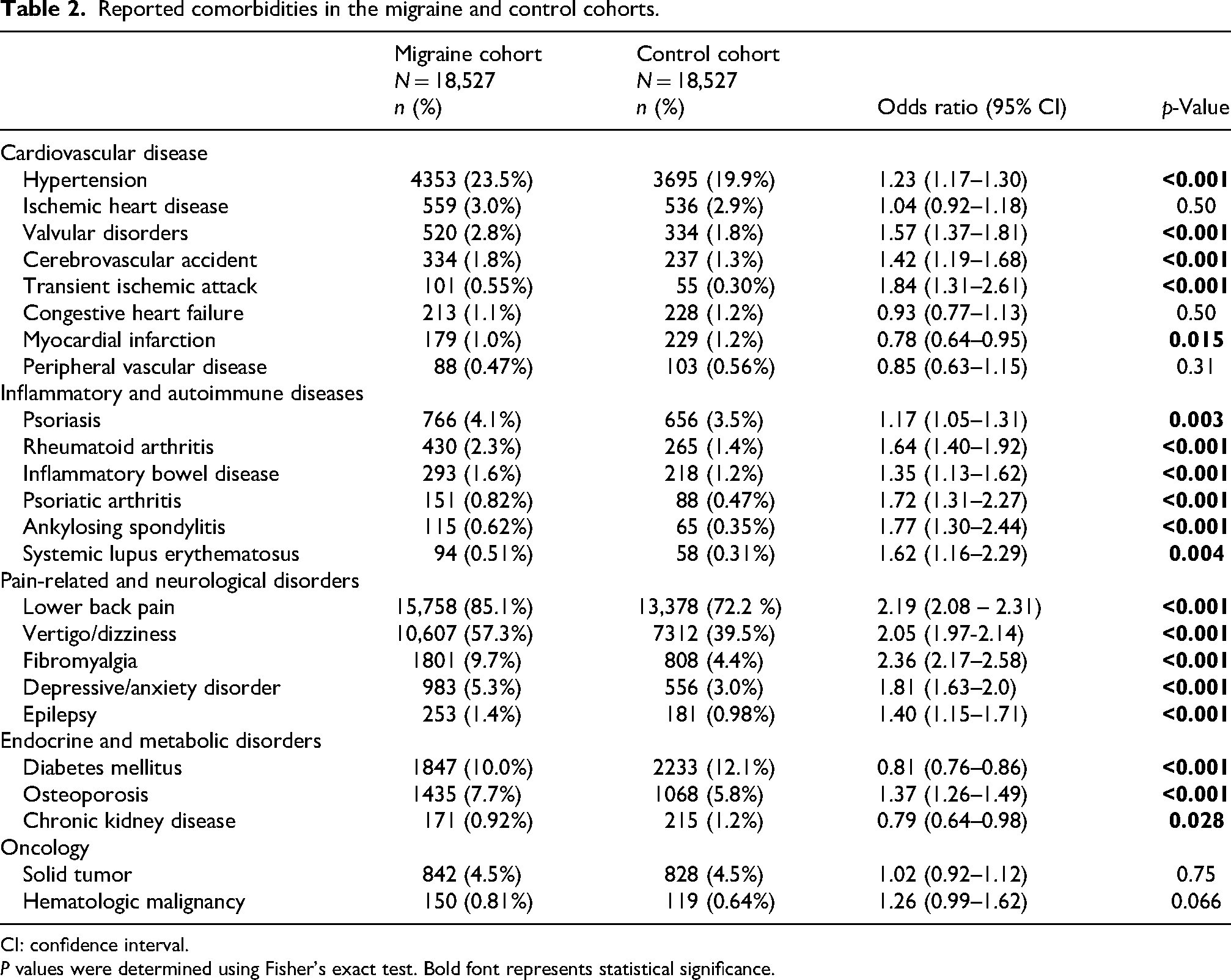
CI: confidence interval.
P values were determined using Fisher’s exact test. Bold font represents statistical significance.
All evaluated inflammatory/autoimmune diseases (psoriasis, rheumatoid arthritis, inflammatory bowel disease, psoriatic arthritis, systemic lupus erythematosus, and ankylosing spondylitis) were significantly more prevalent in the migraine cohort than in the control cohort. The corresponding OR values ranged from 1.17 for psoriasis to 1.77 for ankylosing spondylitis. Similarly, the evaluated pain syndromes (lower back pain, fibromyalgia) and neurological disorders (vertigo/dizziness, depressive/anxiety disorder, and epilepsy) were also statistically significantly more prevalent in the migraine cohort compared to the control cohort, with OR values ranging from 1.40 (epilepsy) to 2.36 (fibromyalgia). No difference in prevalence was observed between the cohorts for oncological diseases (both solid tumors and hematological malignancies) (Table 2, Figure 2).

Forest plot showing the odds ratio for having comorbidities in the migraine versus the control cohort. Odds ratio values >1 indicate higher odds for the comorbidity in the migraine cohort compared to controls. Error bars represent 95% CI. CI: confidence interval.
Utilization of healthcare resources: Migraine cohort versus controls
HCRU among the migraine cohort was compared to that of the control cohort for the 2022 calendar year. The proportion of subjects utilizing healthcare resources was significantly greater in the migraine cohort compared to the control cohort across all evaluated parameters. Thus, significantly more subjects in the migraine cohort had at least one visit in 2022 with a general practitioner (GP), neurologist, pain specialist, other specialists, and nurses, as well as at least one visit to the ED. Likewise, the proportion of subjects requesting approvals for sick days was significantly higher in the migraine cohort compared to controls. Correspondingly, the OR values for utilizing any of the evaluated healthcare resources ranged from 1.3 (day hospitalization or hospitalizations of >1 day) to 4.3 (a nerve block) (Table 3, Figures 3 and 4).

Rates of using variable healthcare resources in the migraine and control cohorts. *P < 0.001, Fisher's exact test comparing the migraine cohort to the control cohort for each evaluated variable. ED: emergency department; GP: general practitioner; HCRU: healthcare resource utilization.

Forest plot showing the odds ratio for using healthcare resources in the migraine versus the control cohort. Odds ratio values >1 indicate higher odds for utilizing the healthcare resource in the migraine cohort compared to controls. Error bars represent 95% CI. ED: emergency department; GP: general practitioner; HCRU: healthcare resource utilization; CI: confidence interval.
Utilization of healthcare resources and sick leave requests among the migraine and control cohorts for the 2022 calendar year.

CI: confidence interval; ED: emergency department; GP: general practitioner.
P values were determined using the two-sample t-test for continuous parameters and Fisher’s exact test for categorical variables. Bold font represents statistical significance.
The extent of HCRU differed significantly between the migraine and control cohorts. The mean number of encounters with a medical professional for 2022 was significantly higher in the migraine cohort across all medical provider categories, including GPs, neurologists, pain specialists, other specialists, and nurses. Similarly, the mean number of ED visits and day hospitalizations was also significantly greater in the migraine cohort. No difference was observed with respect to the mean number of hospitalizations lasting over a day, and the mean number of these hospitalization days. Additionally, the mean number of requested sick days was significantly higher in the migraine cohort compared to controls (mean [SD] of 11.1 [28.4] vs. 8.2 [23.8] days, P < 0.001) (Table 3, Figure 5).

The extent of utilization of healthcare resources in the migraine and control cohorts for the 2022 calendar year. The mean number of events for each parameter is presented, and error bars represent SE. *P < 0.001, Fisher's exact test comparing the migraine cohort to the control cohort for each variable. ED: emergency department; GP: general practitioner; HCRU: healthcare resource utilization.
Discussion
This retrospective matched-control cohort study showed that certain comorbidities were more common in patients with clinically significant migraine compared to controls, while others were similar or lower. Comorbidities with higher prevalence included certain cardiovascular diseases (e.g. hypertension, TIA, CVA, and valvular disorders), whereas the rates of diabetes and CKD were lower in the migraine cohort. Additionally, inflammatory/autoimmune diseases and pain-related/neurological disorders were also significantly more common in the migraine cohort. Furthermore, our study showed that utilization of healthcare resources was significantly greater among migraineurs compared to the controls, and that requests for sick days was also significantly greater.
Our findings regarding comorbidities are broadly consistent with those of other epidemiological studies conducted worldwide, most of which did not employ a matched controlled design.3,11–13 Given that migraine prevalence varies by sex and age, 5 having a matched control or adjusting for these key demographic variables is important to gauge the clinical relevance of migraine epidemiological studies. The limited number of studies that used matched-control designs, although differing in their matching methodologies and endpoints, showed that migraine was associated with an increased risk for the evaluated comorbidities (e.g. neurological disorders, backache, respiratory system infections, and peripheral occlusive artery disease).14,15 Similarly, consistent with our findings, a prospective web-based survey study found significantly greater risk for comorbidities among migraineurs, including hypertension, stroke, inflammatory diseases, and neurological diseases after adjusting for demographic confounders. The risk of these comorbidities increased with higher frequency and greater intensity of the migraine. 16 Notably, our results are not always aligned with published reports. For example, this web-based study found an increased risk for kidney disease with migraine, as did one of the matched-control studies,16,17 whereas in our analysis, the CKD risk was significantly lower. This misalignment could stem from differences in study designs, endpoints, and the patient populations.
The absence of significant differences in the rates of certain cardiovascular diseases (ischemic heart disease, congestive heart failure, and peripheral vascular disease) and the lower rate of MI in the migraine cohort compared to controls may be attributed to the significantly lower prevalence of diabetes in the migraine cohort, potentially influenced by the observed lower obesity rate. Also, only 20% in each of the cohorts were 60 or over, which is the age at which most cardiac complications occur. In a recent cross-sectional study involving approximately 5700 individuals, severe headaches or migraine were significantly associated with increased risk for cardiovascular disease overall (OR, 2.8 [95% CI, 1.6–4.9]), after adjustments for confounders (e.g. age, gender, race, smoking/alcohol drinking status, etc.). However, upon evaluating specific cardiovascular diseases, the significant association was not consistent across all evaluated diseases (e.g. it was evident for stroke and angina, but not for MI, or congestive heart failure). 18
The observation that migraineurs had an increased rate of valvular disorders, which are mostly anatomical and not clinically significant, combined with the increased rate of echocardiograms performed, suggests overdiagnosis of valvular disorders among migraineurs rather than a true association with migraine.
Evidence of the association between migraine and diabetes has not been conclusive.19,20 A recent meta-analysis encompassing eight cross-sectional studies with over a million migraineurs showed no significant increase in the odds of having diabetes compared to non-migraineurs (OR, 1.0 [95% CI, 0.73–1.37]), and similar results were shown in a meta-analysis of two cohort studies with over 32,000 migraineurs (OR, 0.98 [95% CI, 0.85–1.14]). 19 In contrast, in a web-based study, the odds of reporting a diabetes diagnosis were significantly higher among migraineurs (OR, 1.37 [95% CI, 1.3–1.5]). 16 The association between migraine and diabetes is nuanced, and parameters such as migraine with or without an aura, type 1 versus type 2 diabetes, and a past migraine versus active migraine should be considered.19,21,22 In our study, given the higher HCRU among the migraine cohort, the lower rate of diabetes among migraineurs could be due to a higher rate of pre-diabetes diagnosis, prompting preventative measures.
The evidence regarding the associations between migraine and hypertension has not been consistent, with cross-sectional studies reporting positive, neutral, and inverse associations.20,23 Similarly, an in-depth understanding of the pathophysiological mechanism linking the two is also lacking, with subclinical atherosclerosis, increased arterial/aortic stiffness, and endothelial dysfunction all considered contributing factors to both conditions. Interestingly, when focusing on the non-elderly population, the associations seem to be mainly positive. 23 In our study, the population was primarily non-elderly, consistent with the observed positive association in such patients. Additional contributing factors to the increased hypertension rate among migraineurs may be the increased rate of anxiety disorders, as well as likely more blood pressure testing, given the increased HCRU.
The current study, although epidemiologic, points to a mechanistic link between inflammatory diseases and migraine, thereby supporting an increasing number of preclinical studies demonstrating such a connection, through changes in cytokine profiles.4,24,25 Another mechanistic link involves CGRP, whose role in migraine pathophysiology is well established and forms the basis of CGRP inhibitor therapies, since CGRP is involved in the modulation of glucose-stimulated insulin release, influences the secretion of other pancreatic and gut hormones, and is considered a mediator of arthritis. 26 Release of CGRP was also demonstrated in musculoskeletal pain disorders. 26 Aligned with our findings of increased backpain among the migraine cohort, a population based cohort study involving nearly 10,000 subjects found that after adjusting for relevant covariates (e.g. age, gender, drinking/smoking status, etc.), the odds of having backpain were higher in those with episodic migraine, and even more so in those with chronic migraine compared to those with no headache (OR, 4.8 [95% CI, 4.2–5.5] and OR, 9.3 [95% CI, 5.6–15.5], respectively). 27
Our findings regarding increased CVA and TIA rates alongside a lower diabetes rate among migraineurs suggest that migraine may be an independent risk factor for CVA and TIA and support a mechanistic link between them. Indeed, numerous studies suggest that the interplay between stroke and migraine is bidirectional, multifaceted, and involves genetic, hormonal, vascular, and neurobiological factors.28–30
The substantial HCRU reported in our study among subjects with migraine is also consistent with other studies across the world (Europe, USA, Canada), which investigated HCRU among migraineurs, including several studies with a matched control design.14,31–35 Our finding that the migraine cohort had more sick day requests than the control cohort indicates that, beyond the burden of increased HCRU, migraine has a societal impact through missed work and reduced productivity. Notably, the current study utilized EHR and therefore could only analyze sick day requests as a proxy for sick days taken. Regardless, sick days constitute only one aspect of the societal impact and the indirect costs associated with migraine.5,11 Thus, our findings underscore the need for additional research to examine the broader societal and economic impact of migraine, as well as the development of migraine-related healthcare policies that could mitigate the HCRU, societal burden, and economic costs of this disease.
The current study has several strengths. Unlike the majority of studies on migraine epidemiology, this real-world study utilized a matched-control design, allowing to control for age, sex, SES, and demographic group. Other strengths of this study include its use of recent national-level data with long-term follow-up, encompassing populations at risk for health disparity, such as those with medium-to-low SES and those in the Arab and Ultra-Orthodox Jewish communities. Furthermore, the dataset used for the analysis was not based on surveys/questionnaires, which are common practices in the field, but rather on extracting LHS EHR data, which have been previously shown to accurately reflect chronic diagnoses, while employing stringent criteria for identifying subjects for the migraine cohort. 7 Prior studies have confirmed the accuracy of chronic diagnosis records in the LHS EHR system and the utility of this system in investigating population health trends.7,8 The study is limited by its retrospective, observational design that examines associations and not causation. Also, data on the severity and frequency of migraine symptoms or medications purchased privately (not through LHS-affiliated pharmacies) were not available. Lastly, the data presented were not standardized for age or gender, which confounded the comparison to other studies.
Conclusions
This matched-control retrospective cohort study reflecting real-world, national-level data demonstrated that patients with clinically significant migraine had significantly higher rates of certain comorbidities, including certain cardiovascular diseases (hypertension, TIA, CVA, and valvular disorders), inflammatory/autoimmune diseases, and pain-related/neurological disorders, compared to controls. HCRU was also significantly greater among migraineurs than controls. Further research is warranted to elucidate the underlying mechanisms linking migraine with its associated comorbidities and to evaluate the overall economic and policy-making implications of the HCRU findings. Future studies could also examine the rates of imaging and other tests used to diagnose associated diseases.
Clinical implications
This retrospective matched-control cohort study (37,054 subjects in total) showed that certain cardiovascular diseases, inflammatory/autoimmune diseases, and pain-related/neurological diseases were more common in the migraine cohort compared to the controls.
Additionally, utilization of healthcare resources was significantly greater in the migraine cohort compared to the controls, and their request of sick days was also significantly greater.
Footnotes
Ethical considerations
The study was approved by the institutional review board (IRB) of Leumit Health Services (approval number: LEU 0008-23) and was granted a waiver for obtaining informed consent because of its retrospective design relying on secondary analysis of anonymized EHR data. The study was conducted in accordance with the Declaration of Helsinki.
Consent for publishing
All authors have given consent for publication of the accepted manuscript in Cephalalgia Reports.
Author contributions
Concept and design: AS, DD, MT, and AI. Acquisition, analysis, or interpretation of data: AS, ED, DD, MT, AB-S, SV, and AI. Statistical analysis: AI. First draft writing: AB-S. Reviewing and editing: all authors. Final approval: all authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was sponsored by Pfizer Pharmaceutical Israel, Ltd.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DD and MT are employed by Pfizer. AS and AB-S have received consulting fees from Pfizer. ED, SV, and AI declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The raw (unaggregated) data supporting the findings of this study contain sensitive personal health information and are therefore not publicly available. Access to individual-level data is restricted by the institutional review board (IRB) and is permitted only to qualified researchers who receive IRB approval, in accordance with applicable regulatory and privacy restrictions.