
Abstract
Background
Migraine is a highly prevalent, disabling, misunderstood, underdiagnosed, and undertreated neurological disease. It is a leading cause of productivity loss in the workplace.
Methods
This is the first large-scale company-wide headache education and evaluation program in the workplace.
Results
73,432 (90.5%) Fujitsu employees participated. The prevalence of migraine was 16.7%, tension-type headache 40.7%, and cluster headache 0.5%. After completing the training, 82.9% of participants without headache said they would change their attitude towards colleagues with headache disorders and 72.5% of total participants said their understanding of headache changed. The proportion of employees who thought that headache had a significant impact on people’s lives increased from 46.8% to 70.6%; 2971 (4.1%) of all participants were interested in a virtual consultation with a headache specialist as part of the program, more than half of whom had not previously consulted for headache. Approximately 14.7 days per year of full productivity per employee with headache were gained resulting in an annual productivity saving per employee of US$4531.
Conclusion
This unique headache workplace program was associated with a high level of participation, an improvement in the understanding of migraine and attitude towards colleagues with migraine, reduction in disability and increased employee productivity, and decreased costs of lost productivity due to migraine. Workplace programs for migraine should be considered for all industry sectors.
Introduction
Headache disorders are common, disabling, and affect people most during the most productive years of their lives (1). Migraine, in particular, is the leading cause of disability among people 15–49 years of age, and is the second most disabling medical condition worldwide (1). Most (89%) migraine-related productivity loss is due to presenteeism (2). A four-year study looking at the prevalence and productivity impact of 22 common health conditions on nearly 8000 employees in the US health care system found migraine to be the second leading cause of presenteeism, costing the employer about two million US dollars per year (3). Since most migraine-related productivity loss stems from presenteeism, it is seldom noticed by employers (4).
An evidence-based strategy to improve migraine-related work productivity is workplace education to raise awareness, improve diagnosis and treatment, and decrease stigma (5). Five prospective cohort studies in the US that evaluated presenteeism and absenteeism found increased productivity by 29-36% while another prospective cohort study that only assessed absenteeism (not presenteeism) did not find an association (6–11). The largest of these workplace education programs was a disease management program at the University of Minnesota, which had 18,721 employees including 7109 with migraine (11). Five other prospective cohort studies (two in the USA, one in Spain, one in Switzerland, and one in France) showed that workplace migraine education and management programs improve productivity by cutting absences in half, increasing productivity at work during a migraine attack by 36 to 59%, as well as decreasing the costs of migraine-related productivity loss (12–17). These cohort studies were relatively small and the education targeted those who had migraine rather than the entire workforce.
The Migraine Association of Ireland launched a Migraine in the Workplace Survey and found that 30% reported the most important attribute of a workplace program would be an increased understanding and awareness of migraine in the workplace, while 26% felt that a more supportive work environment should be prioritized.
The International Headache Society-Global Patient Advocacy Coalition (IHS-GPAC) was created as a collaboration between patients, headache experts, scientists, patient advocates, and professional neurological, headache and pain organizations to understand and promote the global, regional, and local interests of people with headache disorders (18). Fujitsu, one of the largest information technologies (IT) companies in the world, has led health and wellbeing initiatives as part of its commitment as a Global Responsible Business (GRB) (19). Recognizing the importance of migraine awareness and management in the workplace, Fujitsu collaborated with the IHS-GPAC to establish the “Fujitsu Headache Project” (19). The first step was to assess the prevalence and extent of migraine-related productivity loss. Fujitsu collaborated with the International Headache Society (IHS), IHS-GPAC, the Japanese Headache Society (JHS), and the World Health Organization Western Pacific Regional Office to conduct an internal survey among employees in Japan, Korea, and the Philippines (20,21). Of 2500 participants sampled randomly from the employees and surveyed, 85% (83% of men, 91% of women) had experienced headache including 53% with tension-type headache, 13% with migraine, and 4% with both (20). Of those who experienced headache, 84% had never been treated (20). Work productivity was reduced during an attack by 50% for migraine and 28% for tension-type headaches (20). Even on non-headache days, about 40% of employees with migraine had interictal symptoms, which was consistent with the results of cross-sectional population-based studies in Japan (20,22). The estimated annual economic loss to Fujitsu due to headache-related absenteeism and presenteeism was $1007 per employee with either migraine or tension-type headache (20). For employees with migraine, this economic loss was estimated at $2300 per employee (20). The estimated total annual economic loss to Fujitsu due to headache-related absenteeism and presenteeism was approximately $57 million (1.1% of the total annual salary paid to all employees) (20). Health-related quality of life scores (SF12) of employees with chronic headache disorders were found to be lower than the national standard for Japan (20). About 30% of the participants felt that their headaches disorders were not well-understood by colleagues and supervisors, which is consistent with the results of the Migraine Association of Ireland survey (20). Of the participants with migraine, 12% reported that their headache disorder interfered with their workplace interpersonal relationships and 17% thought that they placed an extra burden on their peers due to their headache disorder (internalized stigma) (20).
The aim of this study was to assess the feasibility (including implementation and participation), satisfaction, quality of life and productivity impact of the first published large-scale headache education and evaluation program in the workplace designed to educate the entire employee population including a special module for executive-level managers of the company to learn how to support people with headache, and not target the employees with headache disorders only.
Methods
Confidentiality and ethical consideration
Participants were notified of the privacy protective measures and confidentiality of the data. Participation in this program was voluntary and only participants who consented to the use of their data were included in the statistical analysis. The educational program (e-learning) protocol was approved by the Privacy Protection Rules of the Personnel Department, and the Headache Consultation program by the ethics committee of Fujitsu Clinic. The entire project was conducted according to the ethical principle of the Declaration of Helsinki. Participants who withdrew their consent were excluded from the analysis.
Participants
All 81,159 Fujitsu employees (including managers) based in Japan were invited to participate. The Fujitsu Headache Project was a part of the Fujitsu health promotion campaign, which is well acknowledged by employees. The importance of this health promotion campaign was repeatedly announced, but no incentive was offered to participate. Employees were invited to participate in the Fujitsu Headache Project via the intranet and newsletters. The health promotion officer and the headache specialist leading the project were interviewed on the importance of the project. These interviews were broadcast on the intranet to all employees. The preliminary program of the e-learning was also sent to the employees.
Intervention
The Fujitsu Headache Project was conducted from July 2019 to February 2022. It consisted of an e-learning program, detailed video seminars, and on-line headache consultation by a staff physician. Industrial health nurses joined the consultation. Additional resources such as a headache school, group work training, and exercise class (see Figure 1), have been planned, but due to the Covid-pandemic, have not yet been implemented. To maintain confidentiality, employees who participated in this study and the virtual consultations were not asked to state their age nor sex.

Fujitsu Headache Project implement a series of programs starting from this e-learning course followed by the headache seminar, headache consulting, referral to specialist care.
The e-learning was a 45-minute educational video program of power point slides with narration made by the health promotion office of Fujitsu to educate employees on the diagnosis and treatment of headache disorders. This e-learning was offered to all Fujitsu employees based in Japan and was delivered on the company’s intranet system. The system did not allow a fast forward option on the videos. To enhance engagement, dynamic content method using the common gateway interface (CGI) system was used (23). The e-learning module provided participants with a test to self-check for a potential headache disorder. The self-check questionnaire was developed by expert consensus based on the International Classification of Headache Disorders (ICHD-3 beta) and was used in prior publications (see online Supplemental Material) (20,24). Participants were informed that the diagnosis shown on the screen was not an official medical diagnosis, but a web-based preliminary diagnosis. Employees who participated in the self-check were asked for their employee number, which led to information about their sex.
Participants were also asked to voluntarily fill a pre- and post-questionnaire to assess their learning from the e-learning (see Table 1). One of the pre-e-learning questions was: “What comes to your mind first about headache?” The first word that appeared was counted by the computer program and considered the key word (25). If the word “headache” was the first word of the sentence, then the second word in the sentence was considered the key word. We regarded the first word picked up by the computer as important as it illustrated the responder's word association with headache. The frequency of the first word or key word was counted and listed manually in descending order to speculate the participants’ first image or their impression of headache.
Questions asked pre- and post-e-learning (N = 73,432 employees who completed the e-learning).

The learning objectives of the program were:
To understand the types, prevalence, impact, and mechanism of headache To understand the impact of a headache on one’s daily life and work To understand how to deal with headache, including prevention, treatment and selfcare To understand how to support people with headache, particularly by the executive-level managers of the company
The e-learning was divided into five sections:
Introduction
The introduction summarized the results of the internal survey discussed above, including the high prevalence and headache-related productivity-loss (20) associated with migraine. It also described the components of the Fujitsu Headache Project.
2. Epidemiology and pathophysiology of migraine
This section offered participants the opportunity to self-check for headache disorder. The questions to help participants make a self-diagnosis of headache were based on the International Classification of Headache Disorders (ICHD-3) as used in the previous prevalence survey, including location, frequency, severity, duration of pain, associated symptoms, aggravating factors, and disability (20). The intranet program promptly showed participants their tentative headache diagnosis including migraine, tension-type headache, cluster headache, or unclassifiable. This section explained the main differences between primary and secondary headaches. It also described the characteristics, potential triggers, and mechanism of tension-type headache, migraine, cluster headache, and chronic migraine versus co-existent migraine and tension-type headache. It ended with the characteristics of secondary headaches.
3. Impact of migraine/headache on daily life and work
This section discussed the lower quality of life and higher disability associated with migraine. It explained that the burden is increasingly high with increasing headache frequency. It described the misunderstanding and stigma associated with migraine, which impacts interpersonal relationships.
4. Headache management
This section was mostly based on the Clinical Practice Guideline for Chronic Headache 2013 (26). It started with the importance of getting a diagnosis and collecting data with a headache diary. Both pharmacological and non-pharmacological treatments were discussed including lifestyle behavioral changes. Recommended self-care practices included nutrition, sleep, exercise (daily three-minute stretching-exercise for headache), and bathing.
5. Creating a headache-friendly work environment
The fifth section was mandatory for executive-level managers of the company, but open to all. It started with the need for headache awareness and understanding, improved workplace interpersonal relationship, and guilt/internalized stigma reported by the participants with headache disorders in the internal survey discussed above (20). It then explains the key components to establish a “workplace of high psychological peace of mind.” It concludes with the workplace factors that can trigger and/or worsen migraine attacks.
Detailed video seminars
The pre-recorded video seminars were 10–15 minutes each and covered various topics such as tension-type headache, migraine, headache in women, and headache exercises. Headache exercises presented in the video seminar consisted of self-care approaches including muscle stretching and the trigger-point stretching at the neck (giving mild stimulation to C2 and trigemino-cervical complex) to help relieve tension-type headache (27,28). Exercise therapy is part of the typical approach to management of chronic tension-type headache in Japan (26).
On-line headache consultation by staff physicians
Employees were invited to participate in a virtual headache consultation via Skype on first-come first-served basis. The plan in the protocol was for consultations to last 20 minutes, but in practice the consultations lasted between 20 and 25 minutes. All the employees who received a consultation were asked to state why they wanted a headache consultation, to complete a headache diary, and to answer questions about their headache including completing the Migraine Disability Assessment (MIDAS) questionnaire before their consultation as well as six months later (29). The consultation included a review of the participants’ headache diary to identify headache characteristics, migraine frequency, number of analgesics taken, potential triggers (such as stress relief on weekends, menstruation, weather changes). During the consultation, treatment options and self-care practices were reinforced. No medication was prescribed. The goals of consultations were to discuss patients’ headache diagnoses and provide potential treatment options including lifestyle and behavioral changes.
Statistical methods
According to the ICHD-3 beta participants’ headaches were classified into five groups: migraine, tension-type headache, cluster headache, unclassifiable, and no headache. Descriptive statistical analyses were performed to compare the prevalence of headache and other clinical features. Chi Square was used to compare the pre- and post-e-learning questionnaire results. Non-parametric paired-t test was used to compare the changes in MIDAS scores pre- and post-headache consultation. The statistical analysis was done with SPSS version 22.
Results
Participation rate
Among the 81,159 Fujitsu Co. Ltd employees including managerial staff in Japan, 73,432 (90.5%) completed the e-learning between October 2020 and June 2021.
Demographics
According to the health promotion campaign data, of the 81,159 employees, 66,550 (82%) were men and 14,609 (18%) were women. Mean age was 47.5 (SD 9.7 years, range 20–72 years) for men and 45.5 (SD 10.5 years, range 21–68 years) for women.
Headache prevalence, diagnosis and management
Out of the 73,432 employees who responded to the self-diagnosis questionnaire offered at the beginning of the e-learning, 12,295 (16.7% of the participants) screened positive for migraine, 29,837 (40.67%) screened positive for tension-type headache, and 355 (0.5%) screened positive for cluster headache (Table 2, this table also provides prevalence by sex). Less than a third of participants, 21,614 (29.8%), did not have headaches. As to the severity of headache, 2323 (5.1%) of 45,492 employees answered “severe to moderate.” Before the e-learning, 18,880 (36.9%) of participants with headache reported not doing anything and just waiting for their headaches to go away when they occurred, 18,370 (35.7%) reported using over-the-counter medications to reduce the pain, and only 1888 (3.7%) sought clinical evaluation for prescription treatment. Out of the 48,238 participants who had headaches, 1169 (2.4%) actively followed regularly with a clinician for their headaches, 7971 (16.5%) sought care in the past, and 39,098 (81.1%) never visited a doctor for their headaches.
Prevalence of headache disorders using the self-check.

Headache word association responses
Although 18,069 employees wrote a short sentence on their image or first impression of “headache,” only 14,676 sentences were included in the analysis once the comments with illegible words or symbols were excluded. Figure 2 shows the frequency of the first words that came to mind thinking of “headache”. The most frequent first or key word was weather (13% of the participants), followed by warning sign of brain disease, migraine (‘migraine’ in Japanese means unilateral headache), shoulder stiffness, sleep (lack or too much), stressful tension, pain (of various cause), eye strain, work (overwork), and concentration (loss). The items ranked low but considered important were “headache is not understood by others”, which ranked 15th and, “work efficiency gets reduced”, which was 16th. “Visiting physician” was ranked 23rd.

Frequent first words in the comment to the pre-questionnaire: What comes to you mind when you think “headache”? (n = 14,676).
e-learning evaluation
Before the e-learning, 26,149 (38.1% of 68,563 responders) considered headaches to not be a disease or a mild disorder compared to 10,938 (14.9% of 73,432 responders) after completing the e-learning (see Table 1). The proportion of participants who found headaches to be part of a disease with a significant impact on someone’s life raised from 32,112 out of 68,563 responders (46.8%) to 51,829 out of 73,432 responders (70.6%) (p < 0.01) (see Figure 3). There was no significant difference between the group who experienced headache and the group who never had headache regarding the change in the concept of headache. The proportion of participants who considered headache to be a potentially life-threatening disorder (8997 of 68,563 responders, 13%) did not change. More than three quarters of total participants (56,434 out of 73,432, 76.9%) answered their attitudes towards their colleagues’ headache disorders changed as a result of the e-learning (Figure 3). Out of the 22,404 participants without headache, 18,577 (82.9%) changed their attitude towards colleagues with headache disorders as a result of the e-learning. Out of those who did not find the e-learning changed their attitudes towards colleagues with headache disorders, 15,035 of 16,998 (88.5%) thought it was because they already had a good understanding of headache, 868 (5.1%) said it was because headache is a private matter with which colleagues should not interfere, and 281 (1.7%) said employees with headache disorders should take care of it themselves for it to not affect their work. The great majority of participants 69,380 out of 73,432 (94.5%) said the e-learning was necessary. The content of the e-learning was understood by 70,715 out of 73,432 (96.3%), 31,450 participants (42.8%) said they understood well and 39,265 of 73,432 (53.5%) said they understood. As to the difficulty of the e-learning, 31,480 out of 73,432 participants (42.8%) said it was easy or very easy, and 33,784 out of 73,432 (46.0%) said it was intermediate. As to its usefulness, 22,214 out of 73,432 participants (30.3%) answered it was very useful and 44,424 out of 73,432 participants (60.5%) said it was useful.

Changes in thought on headache after e-learning.
On-demand 15-minute video seminars on five different topics were prepared, the number of views for each seminar were: Tension-type headache, 722 views; Headache-relieving exercises, 519 views; Migraine, 484 views; Selfcare of headache, 473 views; Women’s headache, 278 views. Less than 1% of participants watched the video seminars.
Workplace virtual headache evaluation
Out of the 73,432 participants who completed the e-learning, 2971 (4.1% of all 73,432 participants, 6.2% of the 48,238 who had experienced headache) were interested in having a virtual headache consultation with a physician. A total of 362 employees including 21 family members and one employee’s friend were booked so far on a first-come first-served basis. Of 362 participants, 247 participants completed their post-six month evaluation of their headache and MIDAS scores, and were included in the analysis. Participants found their consultations useful in terms of clarification of the type of headache (91 of 247, 36.8%), new interest in visiting a headache clinic (58 of 247, 23.0%), knowledge of good treatment for headache and multiple treatment options other than over-the-counter analgesics (59 of 247, 24%), awareness of disability caused by headache (45 of 247, 18.2%), reduction in headache-related anxiety (37 of 247, 15.0%). At the six-month follow-up, absence from work was reduced from 0.72 to 0.45 days per three months (p < 0.05), number of headache days with productivity reduced by at least half due to headaches was reduced from 16.7 to 13.3 per three months (p < 0.01).
According to the web-diagnosis that all the 362 participants interested in a headache consultation filled, 182 (50.3%) had migraine, 142 (39.2%) had tension-type headache, 15 (4.1%) had cluster headache, 57 (23.1%) had other or unclassifiable disorder. Among these employees 176 out of 362 participants (48.6%) never visited physician for their headaches, 136 (37.6%) visited physician in the past, and only 43 (11.9%) were regularly following up for their headaches. A total of 196 (57.0% of 340 employee participants) never consulted with any healthcare professional (including nurses or other advanced practitioners of the health promotion team) for headaches. The reasons for not seeing a physician were 1) being able to reduce the pain with over-the-counter medications, 2) not thinking it to be necessary to see a physician, 3) not knowing which type of physician to visit. Headache-related disability (reduction in work and daily activities) was rated as severe by 140 of 362 (38.7%) participants, moderate by 159 of 362 (43.9%), and mild by 58 (16.0%). The most frequent reasons for seeking headache consultation after the e-learning were 1) suffering from headache for many years (290 of 362, 80.1%), 2) wanting to know about headaches more after completing the e-learning (225 of 362 62.2%), 3) headache interfering with daily activity (152 of 362, 42.0%) and/or interfering work (137 of 362, 37,8%).
The clinical diagnoses made by a Headache Specialist during the virtual consultations (n = 362) using the ICHD-3 beta criteria were compared to the self-check web tentative diagnoses to estimate the accuracy of the self-check diagnoses (24). Among 204 employees who received a self-check diagnosis of migraine, 179 (87.7%) were diagnosed with migraine and 18 (8.8%) with migraine and tension-type headache by the Headache Specialist (96.5% of correct self-diagnosis). Among 87 who received a self-check diagnosis of tension-type headache, 29 (33.3%) were diagnosed with tension-type headache and 56 (64.4%) were diagnosed with tension-type headache and history of episodic migraine of low frequency. Among the six employees who had a self-check tentative diagnosis of cluster headache and who attended a virtual headache consultation, two were in cluster period during their virtual consultation, one employee had a recent cluster attack and was headache free by the time of the virtual consultation, and three employees had a prior history of cluster headache but they only had clinical characteristics of migraine and/or tension-type headache in the two months preceding their virtual visits according to their diary.
Discussion
This was the first large-scale company-wide workplace headache education and clinical evaluation program aimed at raising awareness, increasing understanding, improving workplace relationships and environment, reducing stigma on headache disorders and optimizing diagnosis and treatment for employees with headache disorders.
The 90.5% participation rate (73,432 out of 81,159 employees) highlighted the remarkable project implementation from promotion, reminders, leadership support, dynamic content, and ability for participants to self-check their headaches and receive a preliminary diagnosis.
According to the web diagnoses using ICHD-3 beta criteria, the prevalence of tension-type headache and migraine was 40.6% and 16.7%, respectively, among the 73,432 employees who responded. This was higher than in prior surveys done in smaller samples and the random sampling of 2458 Fujitsu employees in the prior study (20,30,31). The prevalence of cluster headache was higher (0.5%) than in a prior population-based study in Japan (31). When comparing the self-check web diagnoses to the virtual headache clinic diagnoses (n = 362), the accuracy was high for migraine (96.5%). All six employees who received a web diagnosis of cluster headache either were in cluster period (two employees), recent cluster period (one employee), or had a prior history of cluster (three employees).
Headache disorders were largely underdiagnosed and undertreated: 81.1% of participants never visited a doctor for their headaches, which was consistent with prior studies (20,31). About one-third of participants simply waited for their headache attacks to resolve while about a third treated with over-the-counter medications only. The reasons for not seeking headache care were multifactorial, but one of top three most common reasons was not being able to miss work to seek care (32).
When participants thought of headache, the most common word that came to mind was weather (including atmospheric pressure, typhoon, temperature, and humidity) (13%). It can be discouraging that headaches are most associated with an external factor that cannot be controlled. It raises the question as to whether one of the reasons why most people with headaches did not seek care was a sense of fatality – nothing could be done to prevent or help headaches that are related to weather. When patients with chronic recurrent headaches presenting to a Japanese public health center for headache were asked why they had not previously sought medical attention, having known triggers was one of the reasons in 22.9% of patients with migraine and 10.7% of patients with tension-type headaches (32). Some of the factors contributing to participants’ satisfaction after their virtual headache consultations were awareness of the multitude of treatment options and reduction in headache-related anxiety.
The second most common word associated with headache was warning of brain disease and/or severe disease (13%). Although the e-learning addressed secondary headache disorders, the proportion of participants who thought that headache could be a life-threatening disorder did not change between the pre- and post-assessment of the e-learning (13%). About 14% of people with primary headache disorders did not seek care for their headaches out of fear of being diagnosed with a life-threatening and/or severe disease (32).
Despite the term headache being used to mean nuisance, annoyance, vexation, concern, and worry rather than head pain in Japanese, as in English, it is encouraging that those terms did not come up when participants were asked about the first thing that came to their mind when they heard the term headache (33,34).
The participation rate, satisfaction with, and educational impact of the e-learning component of the program was considerable. It raised awareness and increased understanding and substantially increased the proportion of participants who understood that headache disorders have a significant impact on people’s lives. It filled a need; nearly all participants found the e-learning to be necessary. It was also well-understood and was perceived to be of intermediate difficulty. One of the major objectives of the Fujitsu Headache Project was to raise awareness of headache disorders company-wide, and not just among those with headache. One of the most important outcomes is that the e-learning led to a substantial decrease in stigma; 83% of participants without headache changed their attitude towards colleagues with headaches disorders as a result of the e-learning. The Fujitsu Headache Project therefore responded to two of the biggest needs of people with headache disorders in the workplace: feeling understood and supported (20,35). Lack of understanding by colleagues and/or supervisors and stigma are associated with feelings of guilt, impaired work interpersonal relationships, and decreased productivity (increased presenteeism) (20,21,33,36).
The e-learning prompted some employees with recurrent and disabling headaches to seek headache consultation. Out of the 73,432 participants, 2971 (4.1%) were interested in a virtual headache consultation. In the 247 participants who completed their headache consultations and six-month follow up including MIDAS, a web-diagnosis of migraine (41.7%) and tension-type headache (which could include migraine and/or probable migraine) (32%) were most frequent. More than half had never consulted a physician for their headaches despite years of disabling headaches. Most of those 247 participants (82.6%) reported their headache-related disability to be moderate or severe. The demand for virtual headache evaluation far surpassed the capacity of the headache physician. The estimate of about 4% of total employees being interested in headache consultation after a company-wide headache education intervention is extremely important information when planning a headache education and management program in the workplace. The headache consultations helped participants receive an accurate headache diagnosis, understand the myriad treatment options and approaches available, become aware of migraine-related disability, lessen their anxiety related to impending attacks and secondary etiologies, and reduce migraine-related absenteeism and presenteeism.
Cost-effectiveness analysis
The 244 employees who had a virtual headache consultation and completed their six-month evaluation were included in the cost-effectiveness analysis. Extrapolating the MIDAS change results to one year, 1.17 days per employee per year in terms of absences plus 14.0 days per employee per year in terms of presenteeism, results in a gain of approximately 15.2 days of full productivity per employee with headache disorder per year. Using the wage data from the Japanese Ministry of Health, Labor, and Welfare, the average cost of a day of work among Fujitsu employees in 2021, as a company classified as Information and Communication, 1000 employees or more, employee age group of 45–49 years (Fujitsu’s mean is 47.5 years), and average education is University graduate is 7,397,200 yen per year for about 240 actual workdays per year (37). Hence, the estimated annual productivity saving per employee who came for a headache consultation was 469,164 yen or 4692 US dollars..
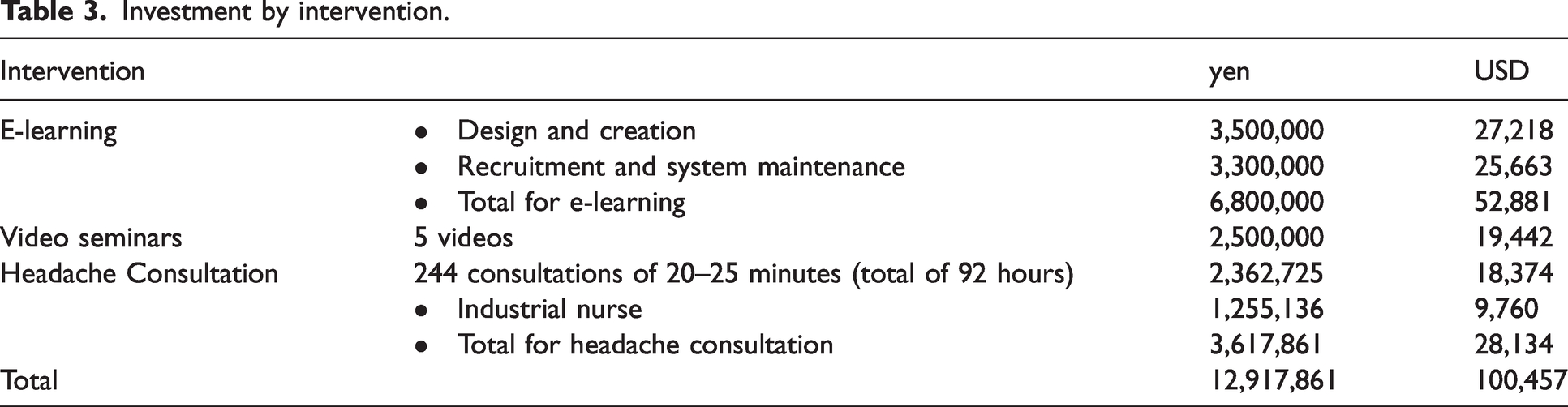
The estimated total investment in the program was 100,457 US dollars for 73,432 employees (Table 3). This is an underestimation as some of the work was done on a voluntary basis including the planning and execution, expert teaching during the video seminars, and the resources and time spent by the Fujitsu Health Promotion team on this project. Only the first 244 consultations already done were counted in the estimated investment, more consultations are pending. Since most of the employees who had a virtual headache consultation had self-reported severe or moderate headache-related disability (299 of 362 participants [82.6%]) and 2323 of the total employees rated their headaches as moderate or severe during the self-check module of the e-learning, the productivity saving of the participants who had a headache consult was extrapolated to the 2323 employees with moderate to severe headaches. The estimated annual headache-related productivity saving was 10,899,516 US dollars. Within the approximations of the estimation described in the limitations paragraph below, the company’s return-on-investment (ROI) was estimated at 3204%.
Investment by intervention.
Of the previous workplace headache education and/or management programs, a ROI calculation was only published for the Novartis Migraine Care study, which also offered e-learning and headache consultation to participating employees. The reduction in absences with the Fujitsu Headache Project was similar to the Novartis Migraine Care study (1.17 days at Fujitsu compared to 1.5 days at Novartis). The reduction in presenteeism was higher at Fujitsu (15.2 vs 9.3 days) (17). With the 10.8 days of increased productivity per employee with migraine per year, the Novartis Migraine Care program led to a positive return on investment of 490% for the employer (17). Both programs were cost-effective and led to substantial decreases in presenteeism.
Limitations
This study had limitations. It was not specifically designed to evaluate the exact total budget needed for this specific health promotion project. All the investment was not accounted for due to voluntary work and use of shared resources with other health promotion programs. The productivity saving estimation has significant limitations as it was estimated from the 244 participants who had a virtual headache consultation. The participants who had a virtual headache consultation may have had more severe and/or disabling headache disorders and the consultation itself may have added impact on both headache burden and work productivity. Given the limitations in the ROI estimation, careful interpretation of the data looking at the details provided in this manuscript is needed. These limitations notwithstanding, the potential to improve the disease burden, quality of life, and productivity of employees with migraine through the implementation of a workplace educational and intervention program, is very substantial. No industry-specific business metric was recorded as outcome. E-learning and virtual headache consultations were necessary because the program was launched during the COVID19 pandemic and in-person headache classes and exercise programs were not possible due to physical distancing requirements during this time. Employees did not undergo a second survey to determine whether an additional cohort may desire a headache consultation. The strength of the study was the participation of leadership which resulted in robust engagement. The ability to access headache specialty care, even if virtual, was a major advantage of this program.
Further studies
A validated tool to measure presenteeism is needed. Studies with business metrics such as industry-specific objective productivity outcomes (e.g. boarding times for airline companies) and/or safety events as primary outcomes of migraine education and/or management programs in the workplace are needed to help advocate for such programs. Studies that confirm the additional impact on disease burden and productivity of a workplace campaign that includes the opportunity for consultation with a medical practitioner or headache expert, as in this study, are needed. Future studies may benefit from a sub analysis of baseline and follow-up migraine-related productivity based on migraine frequency, differentiating low frequency episodic, high frequency episodic, lower frequency chronic, and high frequency chronic (38).
Conclusion
The first large-scale educational and interventional initiative demonstrated the ability for workplace programs in headache to raise awareness, increase understanding, reduce stigma, improve workplace environment, reduce headache-related disability, improve work productivity, and reduce employer costs. Collaboration with the International Headache Society Global Patient Advocacy Coalition – a global coalition of leading headache, neurology, and pain societies, patient advocacy organizations, and patient advocates is instrumental to maximizing the impact of workplace programs in headache. The ability to reduce the burden of illness and improve the health and work-related quality of life in a population of employees impacted by the most disabling medical condition in the world among adults aged 50 years and under, is a model of a public health strategy that should be implemented in workplaces around the world.
Public health relevance
The Fujitsu Headache Project had a high participation rate; 73,432 (90.5%) employees completed the e-learning. The prevalence of headache among participants was high. The prevalence of migraine was 16.7% (11.5% for men, 21.8% for women), of tension-type headache was 40.67% (40.2% for men, 41.4% for women), of cluster headaches was 0.5% (0.5% for men, 0.2% for women. Less than a third of participants had no headache. After completing the headache education program, 82.9% of participants without headache said they would change their attitude towards colleagues with headache disorders and 72.5% of total participants said their understanding of headache changed. Participation in the headache education and clinical evaluation program was found to increase productivity by 1.17 days per employee per year in terms of absences and 14.0 days per employee per year in terms of presenteeism, which represents an estimated 3204% positive return-on-investment.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024231165682 - Supplemental material for Diagnosis, knowledge, perception, and productivity impact of headache education and clinical evaluation program in the workplace at an information technology company of more than 70,000 employees
Supplemental material, sj-pdf-1-cep-10.1177_03331024231165682 for Diagnosis, knowledge, perception, and productivity impact of headache education and clinical evaluation program in the workplace at an information technology company of more than 70,000 employees by Fumihiko Sakai, Hisaka Igarashi, Masako Yokoyama, Olivia Begasse de Dhaem, Hirohisa Kato, Yasuhiro Azuma, Rachel Koh, Heather Phillips, Nim Singh, Audrey Craven, David W Dodick and Hitoshi Miyake in Cephalalgia
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Fumihiko Sakai is consultant for Amgen, Lilly, and Otsuka. Hisaka Igarashi received personal fees for speaker and consulting services from Eli Lilly Japan K.K., Amgen K.K., Otsuka Pharmaceutical Co., Ltd, Sawai Pharmaceutical Co., Ltd., Takeda Pharmaceutical Company Limited, and Daiichi Sankyo Company, Limited. Olivia Begasse de Dhaem receives a stipend for her contribution as Executive Editor of the Pain Medicine journal. She received consulting fees from the virtual headache clinics NeuraHealth and Mable.
Masako Yokoyama, Hirohisa Kato, Yasuhiro Azuma, Hitoshi Miyake, Rachel Koh, Heather Phillips and Nim Singh have no conflicts of interest.
David W Dodick, Consulting: Amgen, Atria, CapiThera Ltd., Cerecin, Ceruvia Lifesciences LLC, CoolTech, Ctrl M, Allergan, AbbVie, Biohaven, GlaxoSmithKline, Lundbeck, Eli Lilly, Novartis, Impel, Satsuma, Theranica, WL Gore, Genentech, Nocira, Perfood, Praxis, AYYA Biosciences, Revance, Pfizer. Honoraria: American Academy of Neurology, Headache Cooperative of the Pacific, Canadian Headache Society, MF Med Ed Research, Biopharm Communications, CEA Group Holding Company (Clinical Education Alliance LLC), Teva (speaking), Amgen (speaking), Eli Lilly (speaking), Lundbeck (speaking), Pfizer (speaking), Vector Psychometric Group, Clinical Care Solutions, CME Outfitters, Curry Rockefeller Group, DeepBench, Global Access Meetings, KLJ Associates, Academy for Continued Healthcare Learning, Majallin LLC, Medlogix Communications, Medica Communications LLC, MJH Lifesciences, Miller Medical Communications, WebMD Health/Medscape, Wolters Kluwer, Oxford University Press, Cambridge University Press. Non-profit board membership: American Brain Foundation, American Migraine Foundation, ONE Neurology, Precon Health Foundation, International Headache Society Global Patient Advocacy Coalition, Atria Health Collaborative, Domestic Violence HOPE Foundation/Panfila. Research support: Department of Defense, National Institutes of Health, Henry Jackson Foundation, Sperling Foundation, American Migraine Foundation, Henry Jackson Foundation, Patient Centered Outcomes Research Institute (PCORI). Stock options/shareholder/patents/board of directors: Ctrl M (options), Aural analytics (options), Axon Therapeutics, ExSano (options), Palion (options), Man and Science, Healint (options), Theranica (options), Second Opinion/Mobile Health (options), Epien (options/board), Nocira (options), Matterhorn (shares/board), Ontologics (shares/board), King-Devick Technologies (options/board), Precon Health (options/board), AYYA Biosciences (options), Axon Therapeutics (options/board), Cephalgia Group (options/board), Atria Health (options/employee). Patent 17189376.1-1466:vTitle: Onabotulinum Toxin Dosage Regimen for Chronic Migraine Prophylaxis (Non-royalty bearing). Patent application submitted: Synaquell® (Precon Health).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.