
Abstract
Background
Disability imposed by headache disorders constitutes an expressive economic burden, mostly from indirect costs due to absenteeism and presenteeism.
Objective
To estimate indirect costs from absenteeism and presenteeism due to headache disorders in Brazil.
Methods
In a secondary, descriptive analysis of two nationwide databases, we estimated indirect costs based on headache-related disability and socioeconomic data.
Results
In the first database analyzed (n = 3838), 12.8% of the employed population with headache disorders missed at least 1 day of work in the last 3 months (mean, 95% CI = 4.2 days [3.7–4.6]). Based on the prevalence of headache disorders, days lost due to headaches and income data, R$ 40.4 billion (Int$ 20 billion) are lost due to headache-related absenteeism annually. For presenteeism, 26.2% of the employed population with headache disorders worked at least 1 day in the last 3 months with 50% reduced productivity (mean, 95% CI = 5.7 days [5.3–6.2]), amounting to R$ 27.3 billion (Int$ 13.5 billion) of financial loss annually. In the other database analysed (n = 205,546), 14,052 (6.8%) respondents missed work/school or household duties in the past 2 weeks due to some disease. Of these, 4.7% attributed their days lost to headaches disorders in the economically active population, which ranked 4th as main cause of days lost due to disease, among 23 common diseases.
Conclusions
The economic burden of headache disorders in Brazil, mostly due to migraine (55.4%), may cost up to R$ 67.6 billion (Int$ 33.5 billion) annually, and headache disorders represent a leading cause of absenteeism due to disease.
Introduction
Headache disorders constitute a leading cause of disability in the world (1,2), in particular primary headaches such as migraine and tension-type headaches (3). Because these primary headaches are common neurologic disorders (4,5), they represent major complaints at consultations in primary care worldwide (2,6).
Owing to the personal suffering and impact on quality of life due to disability, many studies have focused on the socioeconomic impact of headache disorders, including the indirect costs attributed to workdays lost (absenteeism) or days working with reduced productivity (presenteeism) (4,7–13). The headaches disorders-related indirect costs in the United States (8), Europe (12) and China (7), amount to US$ 13.3 billion (from migraine only), € 173 billion, and nearly US$ 82 billion, respectively. In these studies, indirect costs are unanimously the largest share of the total financial burden (7,8,12). A review on the indirect costs of migraine has shown that presenteeism may represent up to 89% of the total costs (14) and this headache subtype apportions the largest share of direct and indirect cost among all headache disorders (7,12).
In Brazil, the 1-year prevalence of migraine and tension-type headache is 15.2% (15) and 13% (16), respectively. Headache disorders may account for up to 10% of primary care consultations (17); 52% of these headaches are primary headaches (18). Migraine alone represents 45.1% of all headache-related complaints in the Brazilian public health system (18). In fact, the costs with care and treatment of migraine in the Brazilian public health system have been estimated at around US$ 140 million annually (19). However, no study has yet estimated the indirect costs from absenteeism or presenteeism due to headache disorders in Brazil.
Therefore, we aimed at estimating the indirect economic burden of headaches disorders in Brazil. We explored the data from two representative samples of the Brazilian population, retrieved from the databases of two nationwide surveys.
Methods
This is a secondary analysis of the databases of two nationwide surveys. The first was the Brazilian headache epidemiologic study (BHES), which was conducted through telephone interviews in 2007 by a multicentre research group (15,16). This survey covered 8168 households and included people aged between 18 and 79 years. The proportion of non-response was 51.1%. For 227 interviews, the questionnaires were not completed, but the questionnaires were completed by 3848 people. Headache disability data were obtained from the migraine disability assessment score questionnaire (MIDAS) (20). Absenteeism and presenteeism were estimated based on the two following headache-related questions regarding workdays lost and productivity: “On how many days in the last 3 months could you not go to work or school because of your headaches?” and “On how many days in the last 3 months could you do less than half your usual amount in your job or schoolwork because of your headaches?”.
The second survey consists of an open-data national health database (Pesquisa Nacional de Saúde, PNS) (21), conducted in 2013 by the Ministry of Health in conjunction with the Oswaldo Cruz Foundation and the Brazilian Institute of Geography and Statistics (Instituto Brasileiro de Geografia e Estatísticas, IBGE). In this survey, 81,167 households composed the sample, without inclusion criteria for age. The proportions of loss and non-response were 20.8% and 8.1%, respectively. Complete data were collected in 64,348 households, with 205,546 people interviewed using a door-to-door methodology (21). For disease-related disability data, participants answered the two following questions: “On how many days in the last 2 weeks could you not go to work, school or do your household duties due to disease?” and “Which was the main disease that prevented you of doing your habitual activities in the last 2 weeks?”. Under the latter question, there followed a formal list with 23 common diseases and a blank space for “Other diseases”. In the formal list, there was an option for “Headaches or Migraine”.
Both surveys’ samples were geographically representative of the Brazilian population and used sampling processes to match the Brazilian Census sample for age, gender, household income, and region (15,16,22). Briefly, the PNS survey adopted cluster sampling with a three-step stratification process to identify Census-based household unity areas (22), while BHES adopted quota sampling based on a database of households with a fixed telephone (15,16).
Indirect costs estimates
For annual headache-related cost estimates, we adopted the human capital method (23). Costs estimates were calculated as Brazilian Reais (BRL) and then converted into International dollars (Int$), considering the purchasing power parity (PPP) values for 2018 (1 Int$ = 2.029 BRL) (24). Indirect costs were calculated only from the BHES database (15,16).
A cost estimate formula is given as follows:

Statistics
This study employed a descriptive analysis of population-based data; thus, data are reported as proportion (percentage) or mean with 95% confidence interval (95% CI). Data analyses and graphs were performed by Microsoft® Office Excel Plus 2013 software (Microsoft®, Washington, USA).
Results
Table 1 summarizes sociodemographic characteristics of the headache population sample in both surveys. In the BHES survey, 2970 out of 3848 (77.1%) respondents presented with headaches in the last year. Regarding disability data, 1307 respondents completed the MIDAS questionnaire. Of these, 277 persons lost at least 1 day of work/school, while 518 persons worked/studied with ≥50% reduced productivity at least 1 day in the last 3 months due to headaches. Figure 1 shows the distribution of days lost (a) or worked/studied/performed with reduced productivity (b) by sex, employment status and age. Sixty-eight percent (858/1268) of all days lost, and 71% (2175/3058) of all days with ≥50% reduced productivity were from women.
Histogram (absolute values) of days lost (a) or days worked with ≥50% reduced productivity (b) due to headaches in the last 3 months by age, sex, and employment status from BHES survey. Sociodemographic data of the headache population samples from the two nationwide surveys. Unemployed, retired, student, voluntary job, or disabled.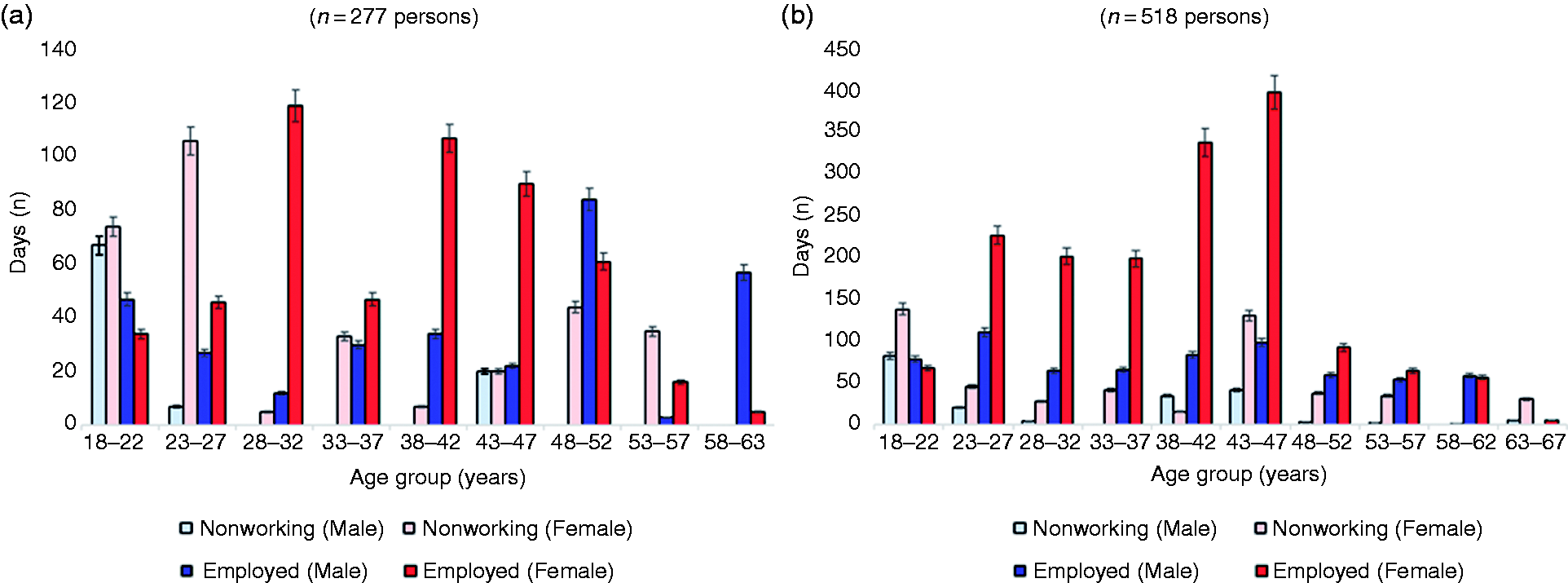

Eighty-one percent of all workdays lost were due to migraine or probable migraine (Figure 2). Two hundred respondents were employed (12.8% of the employed population with headache). In this employed headache population sample, the mean (95% CI) days missed at work in the last 3 months was 4.2 (3.7–4.6), or 3.6 (3.1–4.1) for men and 4.7 (3.9–5.6) for women. For reduced productivity data, 411 respondents were employed (26.2% of the employed population with headache). The mean (95% CI) days worked with ≥50% reduced productivity in the last 3 months was 5.7 (5.3–6.2) in the employed headache population sample, or 4.6 (4.1–5.1) for men, and 5.9 (5.2–6.6) for women.
Distribution of headaches subtypes (as %) contributing to days lost (a) or days lived with ≥50% reduced productivity (b) in the last 3 months (BHES survey).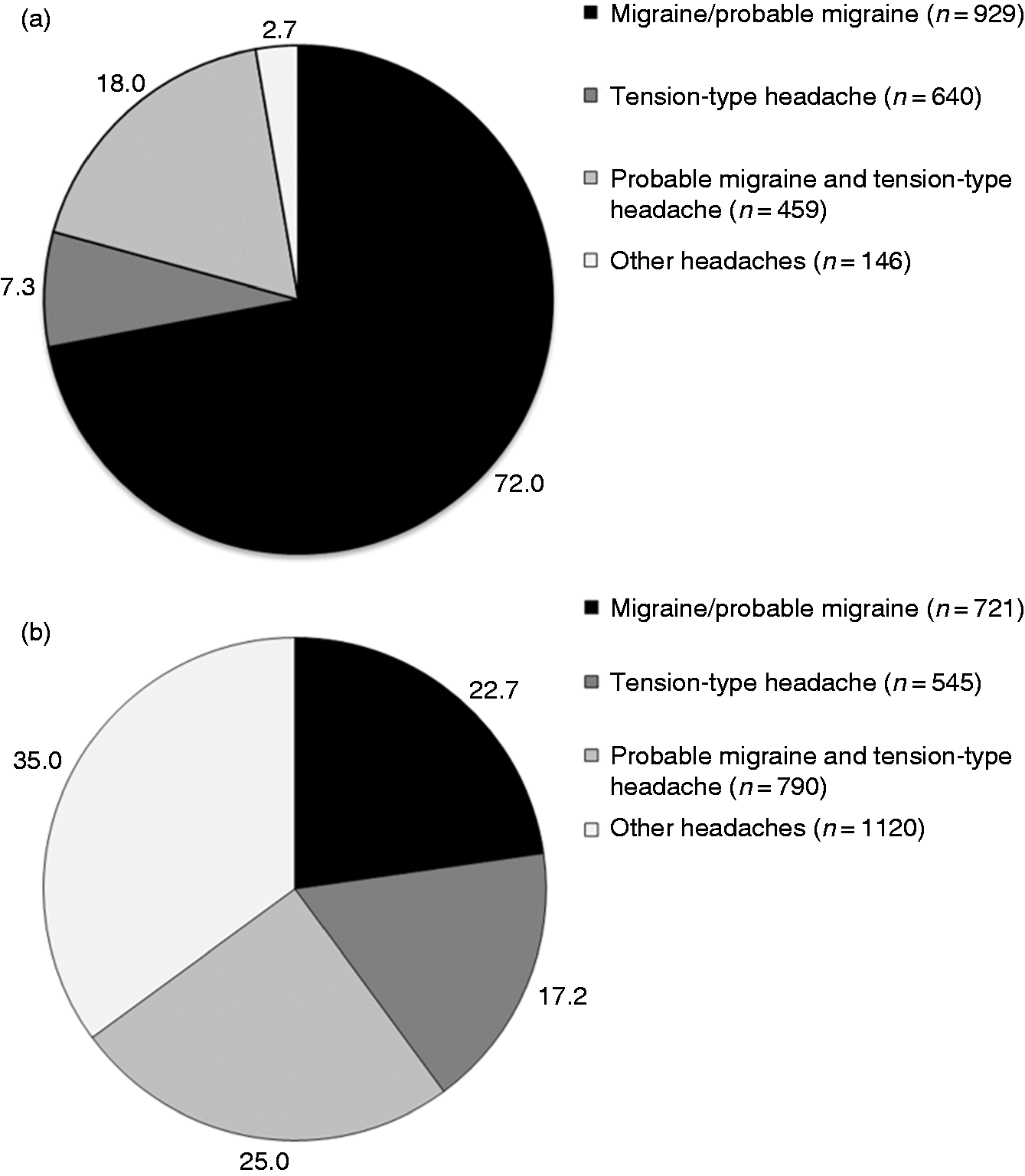
The prevalence of headaches and the proportion of disabled population in the economically active population of the BHES survey is shown in Table 2. Projecting these data to annual estimates, assuming that 53.2% of the Brazilian workforce population (56.1 million) miss on average 16.8 workdays/year, therefore 942.7 million person-days/year are lost due to primary headaches. Considering the income data, a total of R$ 40.4 billion, or Int$ 20.0 billion, are lost annually from absenteeism due to headaches, with a per-person annual cost of R$ 721 (Int$ 355.3). For the reduced productivity data, the annual costs estimate totalled R$ 27.2 billion (Int$ 13.5 billion), with 1.27 billion person-days/year performed with 50% reduced productivity due to headaches, and per-person annual cost = R$ 484.8 (Int$ 240.0). Thus, primary headache disorders constitute a toll of R$ 67.6 billion (Int$ 33.5 billion) to the Brazilian workforce. Migraine (including probable migraine) represented the majority of the total amount, or R$ 37.5 billion (Int$ 18.6 billion), with R$ 22.4 billion (Int$ 11.1 billion) lost from absenteeism and R$ 15.1 billion (Int$ 7.5 billion) from presenteeism. Figure 3 summarizes the economic burden of primary headache disorders due to absenteeism/presenteeism in Brazil.
Annual costs, population with primary headache, and person-days lost estimates from absenteeism (workdays lost) and presenteeism (≥50% reduced productivity) due to headaches disorders in the economically active population of Brazil*. Prevalence of primary headaches disorders, estimated disabled population, and indirect costs*. Based on BHES database (15,16); population and costs estimates were based on the economically active population in 2007, or 105.48 million (25). Migraine Disability Assessment Score (MIDAS); disabled population was defined as MIDAS ≥10. This impact threshold includes persons with moderate-to-severely impacted health defined by a headache frequency ≥3 attacks/month, and who are thus eligible for migraine prevention treatment (31); Int$: International Dollar in 2018 (24). TTH: Tension-type headache.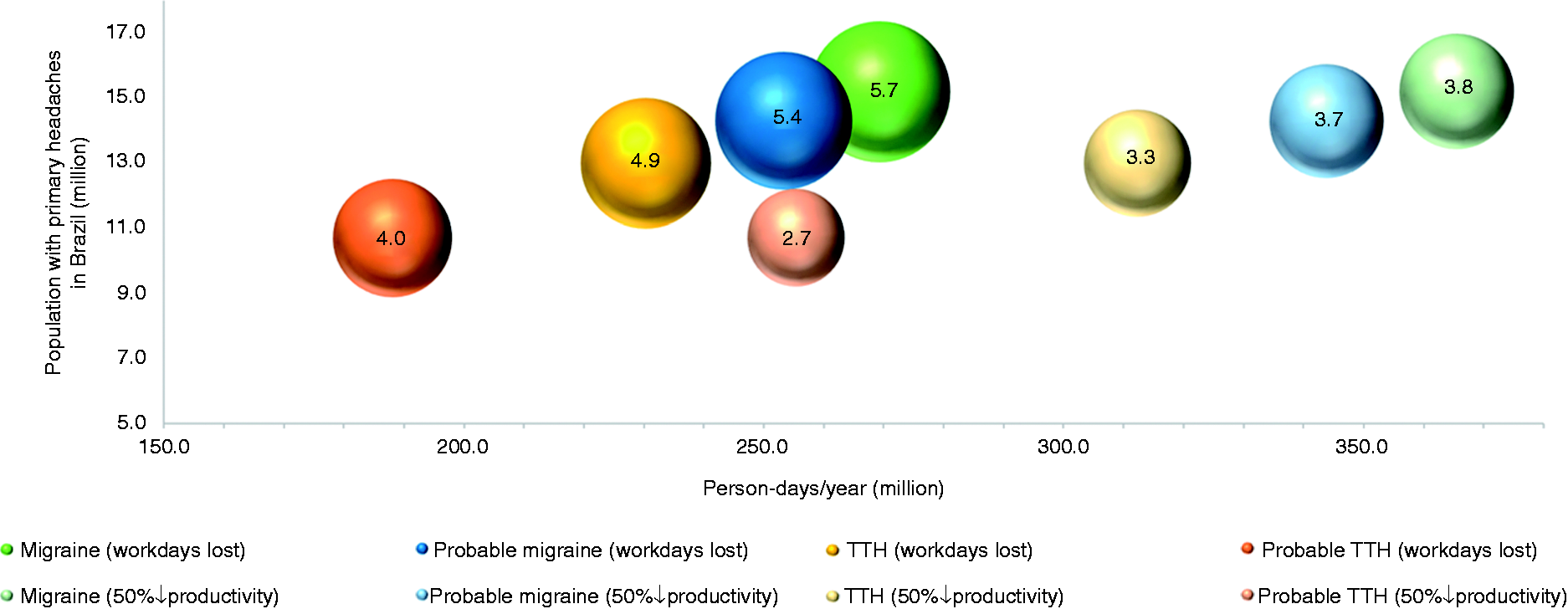

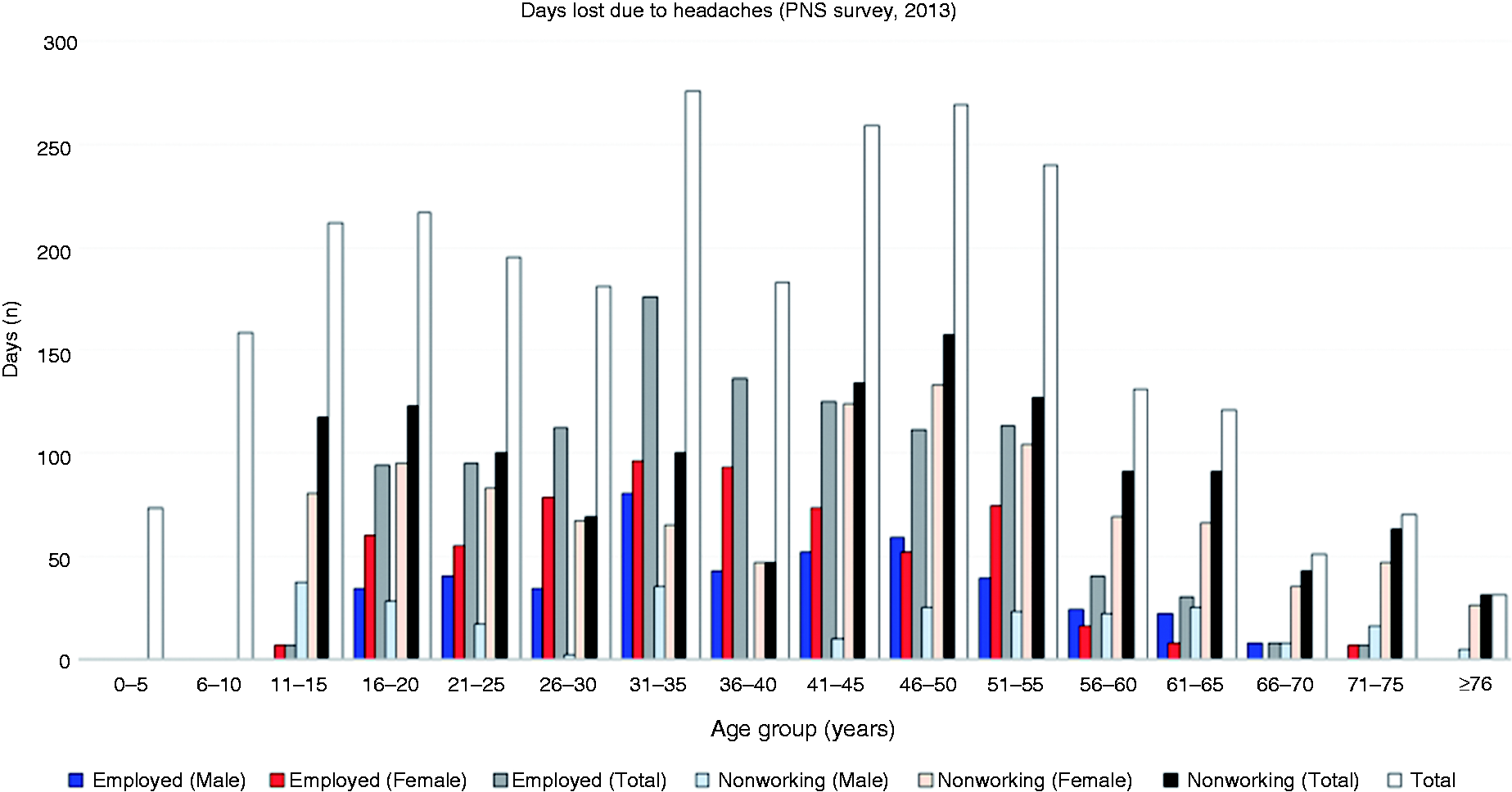
In the PNS survey, from 205,546 persons interviewed, 14,052 respondents (i.e. 6.8% of the population) reported to be unable to work/study or do household duties at least 1 day in the last 2 weeks due to disease or another health-related condition. Of these, 737 (5.2%) persons attributed to “Headaches or Migraines” their days of habitual activities lost. Fifty-five percent (1294/2348) of all days lost due to headaches were from women. Among the economically active population (n = 572), headache and migraine ranked fourth amidst the main causes of days lost due to disease (Figure 4). Figure 5 shows the distribution of days lost by sex, employment status and age. The mean (95% CI) days lost in the last 2 weeks was 3.9 (3.6–4.2), or 3.7 (3.3–4.2) for men, and 4.0 (3.6–4.3) for women. An annual projection of mean days lost in this subsample equals 93.6 days.
Main causes of days of habitual activities lost (work, school or household duties) due to disease in the workforce of Brazil, from 2013 PNS survey. Histogram (absolute values) of days lost due to headaches in the past 2 weeks by age, sex, and employment status from 2013 PNS survey.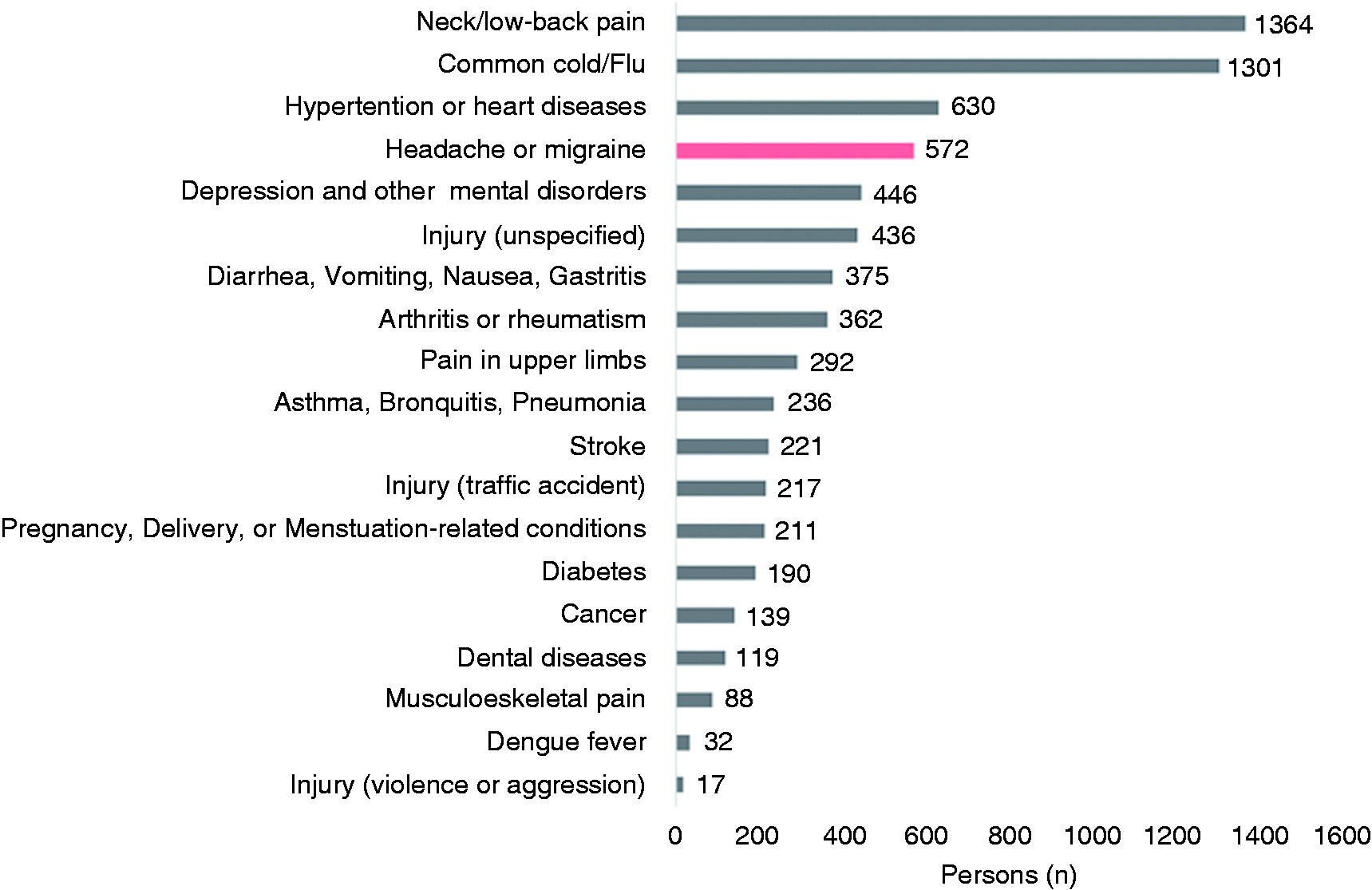
Discussion
In this study, we estimated the indirect costs from absenteeism and presenteeism due to headache disorders in the workforce of the Brazilian population by analyzing two nationwide databases. The main findings of this study are that headache disorders represent an enormous financial toll to society in Brazil, totaling R$ 67.6 billion (Int$ 33.5.0 billion) lost from absenteeism and presenteeism annually, and constitute the fourth most common cause for missing work, school or household duties due to disease. Migraine-related costs amounted to Int$ 18.6 billion, the largest share among headache disorders, and mostly from absenteeism (nearly 60%). Our data corroborate data from other nationwide surveys across the globe with regard to migraine generating the highest absenteeism rates among all headache disorders, but contrast with data on presenteeism, as most studies indicate it has the largest share of total indirect costs (7,12,14,26,27). One explanation for this discrepant data may be that our calculations were based on prevalence data, rather than on the proportion of days lost/worked with reduced productivity in the MIDAS responders’ sample.
Regarding per-person cost, it is difficult to compare the results found here (Int$ 355/year) with others due to differences in the economic aspects of countries where the studies took place, and further analyses with detailed socioeconomic parameters from each country are needed. Yet, our estimates are lower than those from US (around US$ 371–941) (8,9,26) and Europe (€1222) (12), which may reflect the lower mean income and high Gini index in Brazil (0.528 in 2007) (25). Further analyses are needed to evaluate the relative socioeconomic impact locally at each country/region based on these values. Our study adds data on TTH cost estimates. Few studies have estimated costs from TTH. The Eurolight study estimated around €278 per person per year from indirect costs in Europe due to TTH, while a nationwide survey in China estimated a loss of 33.6 billion (around 40% of total indirect costs) from this headache subtype yearly.
Studies aiming at estimating indirect costs from absenteeism/presenteeism due to headaches, albeit mostly only regarding migraine, have adopted self-report surveys, or extracting data directly from administrative records, with prevalence data being used to extrapolate to the general population (“bottom-up approach”) (7,9–12,26–28). These differences in methods have yielded a large variation in absenteeism and presenteeism rates across studies, and hence in indirect costs estimates. Early studies on this topic (again mostly regarding migraine) have shown absenteeism rates range from as low as 0.8 to as high as 74 workdays lost/year in North America (8,9,11,29). Data from nationwide surveys conducted in large populations such as in China (7) and Europe (30) have shown headache-related absenteeism rates of 12 and 55.2 days/year, respectively. For presenteeism, data from US (as for migraine) (8) and China (7) found rates as high as 70 and 65.6 days/year, respectively. Thus, our average number of days lost (16.8) or worked with reduced productivity (22.8) agree with other studies.
In agreement with the data from the PNS survey analyzed here, which ranked headaches and migraine fourth as the main cause of days lost due to disease, Goetzel et al. (26) found headaches/migraine to be a major cause of workdays/productive time lost in a large sample of employees from a medical database and nationwide survey. Still in their study, headaches/migraine indirect cost from absenteeism/presenteeism constituted 89% of the total cost (26). Also, direct costs from migraine in primary care in the Brazilian health system have been estimated at around US$ 140 million (19), which represent much less than the indirect costs found here.
We employed an amply used approach (the human capital method) for estimating indirect costs. Yet, many factors from our approach may have led to either overestimation or underestimation of the data. For example, there could be an overestimation resulting from our assumption that all disability-related data were due exclusively to workdays lost or worked with reduced productivity. Moreover, we assumed that the mean days lost/worked with reduced productivity could be extended to the headache population. A more conservative estimate would use only the proportion of disabled people according to the MIDAS ≥10 criterion for each headache subtype (31). On the other hand, as discussed in an early review on the topic (11), these surveys do not estimate costs from job loss/retirement due to headache disorders. For example, a study with underserved women showed a nearly twofold higher risk of job loss due to health conditions in women with migraine compared to women with no migraine (33).
It is well known that primary headache prevalence peaks in people’s most productive years; that is, around the 30s–40s decades of life (2,4,15,16,31). Recent data from the Global Burden of Diseases study found that migraine and tension-type headache-related disability (measured as years lived with disease, YLD) peaks between 35–39 years (3). Migraine and tension-type headache amounted to 45.1 million and 7.2 million YLDs, respectively, and among women aged between 15–50 years, these primary headaches represented 11.3% of all YLDs in this age and sex group. Accordingly, we observed a similar pattern in the number of days lost from employed women (Figures 1(a)–(b) and 5), with an exception for employed men in the BHES survey (Figure 1(a)), which exhibited a later age peak for absenteeism rate. Possibly, an increased proportion of secondary headaches due to cardiovascular diseases (e.g. hypertension and stroke) in this age group may explain this finding. Overall, these data concur with other data on prevalence by age range, and hence indirect costs from absenteeism/presenteeism (7,12,14,26–29), and stress the fact that headache disorders, led by migraine, are still an overlooked socioeconomic burden to societies, affecting the worldwide population in its most productive years.
The data here have implications for public health politics. Despite some headache disorders being highly prevalent in Brazil (15,16), no resource from the budget of the Brazilian public health system (around R$ 130 billion) has been allocated to any action or program focused on reducing their socioeconomic impact. Thus, the findings of this study should be used to justify the allocation of financial resources to further study the burden of headache disorders, as well as to implement prevention and management interventions delivered by the public health system, to tailor specific workplace health promotion programs, and promote disease advocacy campaigns in order to minimize the personal and societal economic burden of headache disorders.
Our analyses here are limited by methodological biases inherent to the surveys, such as recall bias and the fact that work impact data were not set as primary outcomes in both surveys. The strength of this study is that it explored the only nationwide samples available to date with information about headache disorders and job status in Brazil. In the case of the PNS survey, it comprises the largest and most comprehensive health survey ever conducted in Brazil. Future studies should be structured to focus on retrieving data from larger samples and directly from administrative records of workdays lost, sickness leave and/or workers’ compensation for an accurate estimate of the entire financial impact of headache disorders in Brazil.
In summary, headache disorders constitute a leading cause of absenteeism/presenteeism in Brazil, and generate a large economic burden. More studies are needed to provide updated data on prevalence and the socioeconomic impact of headache disorders in Brazil.
Public health relevance
Headache disorders rank fourth as cause of days lost due to disease in the workforce of Brazil. People with headaches disorders can miss up to 3 months per year from work, school, or household duties. The indirect cost of primary headache disorders in Brazil total R$ 67.6 billion (Int$ 33.5 billion) annually.
Footnotes
Acknowledgements
We are thankful to Associação Brasileira de Cefaleia em Salvas e Enxaqueca for supporting this study. We also appreciate Alexander Itria for his guidance on the socioeconomic analyses of indirect costs.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Associação Brasileira de Cefaleia em Salvas e Enxaqueca – ABRACES.