
Abstract
Objective
To identify factors associated with work productivity in adults with migraine, and accommodations or interventions to improve productivity or the workplace environment for them.
Methods
We conducted a scoping review by searching MEDLINE, Embase, PsycINFO, Cumulative Index of Nursing and Allied Heath Literature, and Web of Science from their inception to 14 October 2019 for studies of any design that assessed workplace productivity in adults with migraine.
Results
We included 26 articles describing 24 studies after screening 4139 records. Five prospective cohort studies showed that education on managing migraine in the workplace was associated with an increase in productivity of 29-36%. Two studies showed that migraine education and management in the workplace were associated with increased productivity (absenteeism decreased by 50% in one study). One prospective cohort study showed that occupational health referrals were associated with more than 50% reduction in absenteeism. Autonomy, social support, and job satisfaction were positively associated with productivity, while quantitative demands, emotional demands, job instability, and non-conducive work environment triggers are negatively associated with productivity in workers with migraine.
Conclusion
Despite migraine being the second leading cause of disability worldwide, there is a paucity of strong data on migraine-related work factors associated with productivity.
Introduction
Migraine is a highly prevalent disorder that affects 15% of the global population and peaks during the most productive years (25–55 years of age) (1). It is the leading cause of disability for ages 15–49 and the second most disabling medical condition both in the US and worldwide (2).
The Americans with Disabilities Act (ADA), enacted in 1990, and its amendment in 2008 provide people with migraine the right to reasonable accommodations in the workplace. This includes adaptations to enable them to perform their essential job functions despite the disability associated with migraine attacks (3). Maintaining work productivity in the context of chronic illnesses requires job adaptations from both the employers (e.g. work schedule flexibility) and employees (e.g. wearing light sensitivity glasses, optimizing desk ergonomics) (4,5). Migraine-related disability is complex and multifactorial. Disability associated with migraine is attributable to a combination of headache pain, migraine accompanying symptoms such as nausea and photophobia, comorbidities, and psychosocial factors (6,7).
Despite the legal requirement for accommodations to support work productivity in people with disabling migraine, migraine remains a substantial economic burden and source of lost productive time. According to Stewart and coauthors, lost productive time (LPT) is the sum of absenteeism (missed work time) and presenteeism (number of work hours with decreased productivity weighted by the percent decrease in productivity during those hours) (8). Absenteeism refers to the time absent from work due to a medical condition or disability (9). Presenteeism refers to decreased productivity at work due to a medical condition or disability (10). The annual cost of migraine productivity loss to employers is estimated at $13 billion in the US and €27 billion in Europe (11,12). Although people with migraine are more likely to have short-term disability claims compared to people without migraine, presenteeism represents up to 89% of the migraine-related productivity loss (13). Presenteeism is thought to cost 10 times more than absences to employers (14). A narrative review including 15 studies of migraine-related work productivity loss estimated that people with migraine were absent on average 4.4 workdays per year and present at work with reduced productivity due to migraine for another 11.4 days per year (15).
In this scoping review, we aim to systematically survey the literature for quantitative and qualitative evidence regarding factors and interventions associated with workplace productivity in people with migraine or severe headache. Defining these elements will guide employers in establishing reasonable work accommodations and developing interventions to increase productivity and improve the work environment of workers with migraine.
Systematic reviews are meant to test specific hypotheses with predefined populations, interventions, comparisons, and outcomes, while scoping reviews aim to gather all available data on a topic (16). A scoping review methodology was deemed to be more fitting for this study due to the lack of current literature in the area of migraine-related work factors and interventions associated with productivity (16).
Methods
Protocol and search strategy
The protocol is available in Supplemental Material A. There is no registration process for scoping review protocols, so the protocol was not registered. An initial limited search of PubMed and MEDLINE on 7/24/2019 led to the analysis of terms contained in title, abstract, index, and MESH of relevant articles. The initial search led to a draft search strategy for the MEDLINE database. One of the authors (OBdD) ensured that previously known relevant articles were included in the results of the draft search strategy and that the draft search strategy identified articles of interest. The search strategy and protocol were finalized in October 2019. The search strategy is available in Supplemental Material B. Titles and abstracts were searched for terms relating to migraine or headache, and terms related to work productivity such as absenteeism, presenteeism, sick leave, work performance, unemployment, employment.
Studies examining factors associated with work productivity or performance in adults with migraine, or interventions to improve work productivity, were identified by searching MEDLINE (Ovid Technologies), Embase (Elsevier), PsycINFO (EBSCO), Cumulative Index of Nursing and Allied Heath Literature (CINAHL, EBSCO), and Web of Science (Clarivate Analytics) from their inception to 14 October 2019. Controlled vocabulary terms were included when available, and no language or date limits were applied. Bibliographies of relevant articles were scanned to identify additional studies. All searches were designed and carried out by an experienced information professional. Only published material was reviewed. Abstracts were included. There was no restriction on the time frame. We searched all databases since inception. The study inclusion and exclusion criteria are listed in Table 1. We did not restrict studies by geography, language, ethnicity, or gender. There was no restriction by type of setting. Settings included national data on work environment and living conditions, national working population databases, workplace databases, population-based surveys of participants with primary headache, and clinic-based surveys of patients with clinically confirmed headache diagnosis per ICHD criteria.
Inclusion and exclusion criteria.

Literature search results were managed with the Covidence software. The bibliographic information was recorded with EndNote.
Selection and collection process
One author (OBdD) screened the titles and abstracts obtained from the literature search. As illustrated in Figure 1, two authors independently duplicated the process (BH and MHG). A fourth author (RB) independently resolved any conflicts. Two authors (OBdD and MHG) independently reviewed the full texts for all the titles that appeared to meet the inclusion criteria. These two authors (OBdD and MHG) extracted the data independently and in duplicate for each eligible study. One author (OBdD) created a charting table to record the key information from the articles, including: author, reference, year of publication, country, sample size, participants’ characteristics, study design, migraine-related work factor, study duration, outcome, results, and method of headache diagnosis. Two authors (OBdD and MHG) assessed the risk of bias for each study using the Newcastle Ottawa score (17). After reviewing the selected articles, one author (OBdD) organized the results under the four main categories presented below, which were not a priori defined.

Data extraction.
Results
Data extraction
The search of electronic databases returned a total of 7009 records and 4139 records after removing duplicates (Figure 1). Out of the 62 full texts screened, 26 were included in data extraction (Figure 1). The 26 extracted articles described 24 studies from all over the world. The study locations were: US (10 studies), EU (10 studies), UK (one study), Australia (one study), Burkina Faso (one study), Canada (one study) (Figure 2). The study designs included 13 prospective cohort studies, 10 cross-sectional studies, and one focus group study. The migraine-related work factors and interventions evaluated included employer-sponsored migraine education programs (six studies), employer-sponsored migraine education and management programs in the workplace (three studies), job characteristics (14 studies), and one study of screening for migraine in the workplace and referring to a headache center for management and follow-up.

Study locations.
Migraine education programs in the workplace
Table 2 lists the six prospective cohort studies, all completed in the US, that looked at the association between migraine education at work and productivity (9,18–22). The types of education varied: disease management program with a nurse call-in line, printed information with newsletters, computer-based program, a 45-min kit on managing migraine in the workplace, a 3-h long lunch educational program (on impact of headache and diagnosis and lifestyle and pharmacologic management and prevention led by a neurologist, psychologist, and nurse), and the Healthy Living with Migraine educational program (five webinars followed by weekly emails with tips for managing migraine in the workplace organized by a Headache Medicine specialist, a pharmacist, a behavioral health counselor, and a dietitian). The disease management program included health risk assessment, lifestyle changes, online self-help modules, daily walk-in program, nurse call-in line, web-based library of informal materials, and telephonic coaching (9). Five of these studies showed a positive association between migraine education and productivity (18–22). These interventions increased productivity by 29–36%. There was no association between the migraine disease management program and work absences, but that study did not evaluate presenteeism (9).
Association between workplace migraine education programs and productivity.

Migraine education and management programs in the workplace
Table 3 lists the three prospective cohort studies that assessed whether migraine education followed by migraine management programs in the workplace were associated with productivity (23–26). Two of those studies were conducted in the US and one in Spain (23–26). Two of the studies showed a positive association between migraine education and management in the workplace and productivity (23–26). In Vicente-Herrero et al., worker productivity on headache days increased from 59% to 94.8% and absenteeism decreased by about 50%. In Parker et al., the participants’ MIDAS score decreased from 20 to 6.7. One study only found a positive association between migraine education and management in the workplace and productivity for the subgroup of participants who sought medical care for their headaches and had successful migraine control (25). The worksite disease management program (DMP) used in that study consisted of tailored behavioral print material and web resources, physician-led migraine educational conferences in the workplace, and access to worksite physicians for same-day treatment (25).
Association between workplace migraine education and management programs and productivity.

Migraine screening in the workplace and referral
One prospective cohort study studied the impact of migraine screening and referral to outside clinics for migraine care on work productivity. This study included 575 workers recruited from occupational health centers of 17 different French companies with a wide array of jobs (27). Migraine-related absenteeism rates were significantly reduced for both groups after intervention. Absenteeism reduced from 26.6% to 10.4% in the group who already followed with a provider for migraine and had more disability at baseline, and from 13.4%% to 2.2% in the group who had not seen a provider for migraine in at least 1 year.
Job characteristics
Table 4 lists 14 studies that assessed the impact of job characteristics on work productivity in people with migraine. The study designs included cross-sectional (10 studies), prospective cohort (three studies), and a focus-group (one study). Those studies were conducted in Europe (eight studies), the US (two studies), Burkina Faso (one study), Canada (one study), the UK (one study), and Australia (one study) (12,28–41).
Association between job characteristics and productivity.
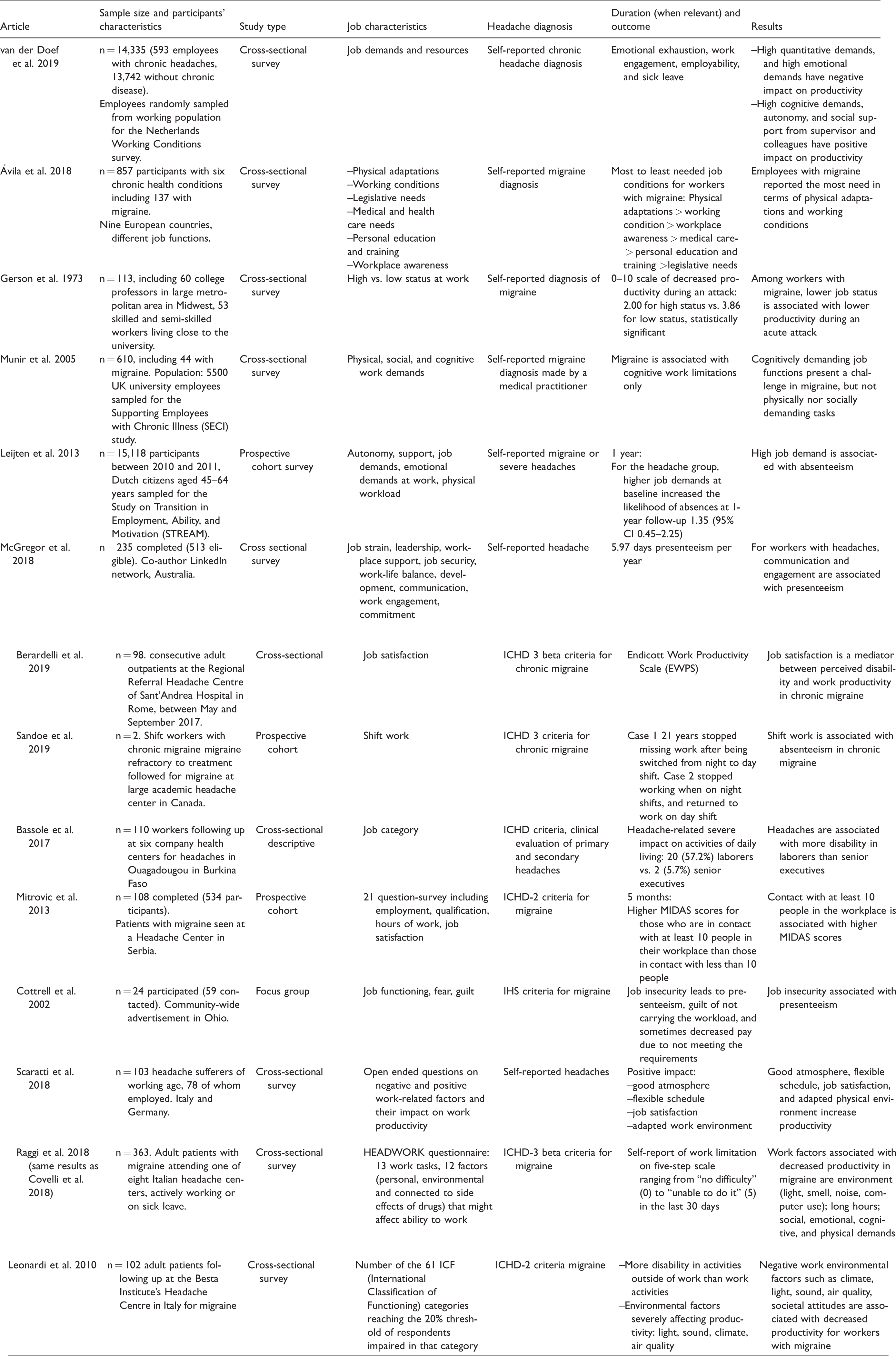
Job characteristics that were found to be positively associated with productivity included sense of autonomy, social support especially from the supervisor, and job satisfaction. One cross-sectional survey assessed the impact of autonomy on work productivity (28). In regression analyses, autonomy was associated with better productivity and less burnout. Three cross-sectional surveys assessed the impact of support on work productivity such as support from supervisor, social support, and good atmosphere (28,38,39). In regression analyses, support at work was also associated with better productivity, increased dedication, and less burnout (28). A focus group of 24 participants discussed that the fear of losing a job or being paid less due to migraine-related missed work led to presenteeism. Pushing through at work despite a migraine attack led to lost productivity, feelings of guilt for not carrying the workload, and sometimes decreased pay for not meeting the requirements (38). In an open-ended survey of work factors positively or negatively affecting productivity, good atmosphere was thought to be associated with increased productivity (44). Table 4 lists three cross-sectional surveys that assessed the impact of job satisfaction on work productivity (30,34,39). There was no strong evidence to support those seemingly positive work factors.
Job characteristics that were negatively associated with productivity included the work environment harboring common migraine triggers (e.g. light, noise, smell, poor air quality, and lack of restrooms), quantitative demands (e.g. high work load, long work hours, inflexible schedule), emotional demands (e.g. stressful work atmosphere), lower job status (e.g. semi-skilled worker vs. university professor, laborer vs. senior executive), and shift work (working night shifts vs. day shifts). Non-conducive work environments for people with migraine (lights, computer use, noise, smell, restricted access to water and restroom, restricted breaks) were associated with decreased productivity. Accordingly, migraine-friendly physical adaptations to the work environment were associated with increased productivity (12,29,39,40). Two cross-sectional studies and one prospective cohort study suggested a negative association between quantitative work demands and productivity (28,32,40). Two cross-sectional studies found a negative association between emotional work demands and productivity (28,40). The question of job status was limited between semi-skilled worker versus university professor and laborer versus senior executive (30,36). A prospective study of two selected shift workers with chronic refractory migraine suggested an association between night shifts and work absences, but the sample size of two was too small to make definite conclusions (35).
The data on work productivity was equivocal for cognitive demands, physical demands, and social demands. Three cross-sectional surveys evaluated the association between cognitive demands and productivity for workers with migraine (28,31,40). Two found a negative association and one found a positive association. In the one that found a positive association, cognitive demands were markers of engagement (28). In the studies that found a negative association, cognitive demands were challenging to the workers with migraine (31,40). One cross-sectional survey addressed physical demands in workers with migraine and did not find an association between physical work demands and productivity (31). One cross-sectional study did not find an association between social work demands and productivity in people with migraine (31). A cross-sectional survey found that social demands at work and engagement were associated with presenteeism in people with migraine (33). A prospective observational survey of 108 participants followed at a Headache Center in Serbia showed a positive association between MIDAS score and contact with at least 10 other people in the workplace (37).
Risk of bias
The average Newcastle Ottawa score was 3.4 with scores ranging from 1–9 and most common scores 2 and 4 (Table 5). Since there is no widely accepted method to assess work presenteeism, this is a self-reported outcome assessed in a multitude of ways in different studies. Most of the studies evaluating headache-related work factors and productivity relied on self-reported headache diagnosis, were based on convenience samples or otherwise non-representative samples, lacked control-groups, and relied on self-reported outcomes with no or inadequate follow-up. These study designs are susceptible to substantial bias and account for the low Newcastle Ottawa scores (48). No randomized control trial of migraine-related work intervention for increasing work productivity was identified.
Newcastle Ottawa scores as risk of bias assessment.

Discussion
In this study, we identified headache-related work factors and interventions associated with productivity in people with migraine. Workplace migraine education programs with or without subsequent integrated migraine management at work are positively associated with decreased presenteeism. Screening for migraine via occupational health centers and referral to outside appropriate care is associated with a reduction in absenteeism in one study. Disclosing migraine or severe headaches to a work supervisor can be difficult given the stigma associated with migraine (42). Creating migraine education venues in the workplace and referral pathways to headache care allows people with headaches to access resources without having to disclose their disease if they do not feel comfortable. Potentially modifiable headache-related work factors associated with increased productivity include sense of autonomy, social support, and job satisfaction (Table 6). Other potentially modifiable headache-related work factors associated with decreased productivity include work factors conducive to migraine attacks (e.g. light, noise, smell, poor air quality, and lack of restrooms), quantitative demands (e.g. high work load, long work hours, inflexible schedule), and emotional demands. A non-modifiable headache-related work factor associated with decreased productivity identified in this study is lower job status (e.g. semi-skilled worker vs. university professor, laborer vs. senior executive). Given that those jobs are fundamentally different, the difference in migraine-related productivity might be due to factors other than job status such as physical demands, outside versus inside activities for example. It is encouraging that most headache-related work factors associated with productivity are potentially modifiable.
Headache-related work factors associated with productivity.

The identification of modifiable workplace factors and interventions that positively affect productivity for people with migraine is an important step in addressing the significant economic loss associated with migraine (3). Two retrospective observational cohort studies estimated that people with migraine had total mean annual indirect costs $2350 to $2834 higher and 1.94 more odds of having short-term disability claims compared to matched people without migraine (43,44). Three quarter of the indirect costs were attributed to absenteeism, 21% to short term disability, and 4% to workers compensation (44). Presenteeism was not measured (44). Since there is no standardized assessment of migraine-related presenteeism, presenteeism can be difficult to quantify and hence is often not measured (45,46). A 15-month prospective study of setting up a headache clinic within Occupational Health for a factory of 7200 employees in Turkey showed that chronic migraine was associated with 3.5 missed work days per year and 87 annual days of presenteeism, representing a 38% productivity loss per year (47). According to a literature review on the specific work impairments of people with migraine, there is a paucity of data on the types of work activities affected by migraine attacks. The authors found some evidence in at least one paper for limitations in problem-solving skills, speaking, driving, and ability to perform all expected duties (48).
Our study suggests that employers could potentially increase workplace productivity by adapting work environment and conditions to the needs of people with migraine. For example, physical accommodations such as reductions in exposure to bright light, noise, and odors, improvement of air quality, and accessible restrooms could increase work productivity in those with migraine. Adjusting workload, adding flexibility to the work schedule, and creating a supportive atmosphere at work could also increase work productivity in those with migraine. Providing migraine education and ensuring access to headache care for those who need it may also improve work productivity.
Our study also highlighted the need to standardize methods to assess presenteeism (49). An Italian group recently developed the HEADWORK questionnaire, a self-reported measurement of work-related migraine disability (50). A standardized assessment of presenteeism would improve the quality and comparability of future studies of headache-related work factors and productivity. More research is needed in terms of cognitive demands, social demands, and physical demands specifically.
Limitations
One of the limitations of this study is that it encompasses a significant number of quality-based surveys and quality assessment for quality-based surveys is challenging. The Newcastle Ottawa quality assessment scale for cohort studies is not a good fit for such a study design. Another limitation is that different studies assess different work factors. There are no side-by-side comparisons of migraine-related work factors affecting productivity.
Conclusion
Despite migraine being the second leading cause of disability both in the United States and worldwide, there is a paucity of data on migraine-related work factors and interventions associated with productivity, and the existing evidence is of low quality. Education on managing migraine in the workplace is associated with decreased presenteeism. Occupational health referrals to headache care might decrease headache-related absenteeism. Autonomy, social support, and job satisfaction are positively associated with productivity in workers with migraine. Quantitative demands, emotional demands, job instability, and non-conducive work environment headache triggers are negatively associated with productivity in workers with migraine. Even if more research is needed to guide advocacy efforts for people with migraine in the workplace, our study identified modifiable headache-related work interventions and factors that could not only increase productivity when adapted to those with migraine, but potentially also reduce the economic burden of episodic and chronic migraine.
Public health relevance
Workplace migraine education and management programs increase productivity. Autonomy, social support, and job satisfaction are positively associated with productivity in adults with migraine. Quantitative and emotional job demands, job instability, and work environment harboring migraine triggers are negatively associated with productivity in people with migraine. The identified studies have a high bias risk. A validated assessment of presenteeism would improve the quality and comparability of future studies.
Supplemental Material
sj-pdf-1-cep-10.1177_0333102420977852 - Supplemental material for Identification of work accommodations and interventions associated with work productivity in adults with migraine: A scoping review
Supplemental material, sj-pdf-1-cep-10.1177_0333102420977852 for Identification of work accommodations and interventions associated with work productivity in adults with migraine: A scoping review by Olivia Begasse de Dhaem, Mohammad Hadi Gharedaghi, Paul Bain, Gabrielle Hettie, Elizabeth Loder and Rebecca Burch in Cephalalgia
Supplemental Material
sj-pdf-2-cep-10.1177_0333102420977852 - Supplemental material for Identification of work accommodations and interventions associated with work productivity in adults with migraine: A scoping review
Supplemental material, sj-pdf-2-cep-10.1177_0333102420977852 for Identification of work accommodations and interventions associated with work productivity in adults with migraine: A scoping review by Olivia Begasse de Dhaem, Mohammad Hadi Gharedaghi, Paul Bain, Gabrielle Hettie, Elizabeth Loder and Rebecca Burch in Cephalalgia
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: OBdD receives an honorarium for her work as Co-Head of the Headache and Facial Pain Section of the Pain Medicine journal.
MHG, PB, GH, EL, and RB report nothing to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.