
Abstract
Aims: The aim was to estimate the prevalence of medication overuse headache (MOH) in Sweden and to analyze the occurrence of this disorder in different population groups.
Methods: A total of 44,300 randomly selected individuals (55% women), aged 15 years and above, were interviewed in a national telephone survey, using a standardized questionnaire including the International Headache Society criteria for MOH and questions about sociodemographic factors, headache history and medication use.
Results: In Sweden, 3.2% (95% confidence interval (CI) 3.1–3.4), n = 1428) suffer from chronic daily headache (CDH) and out of those, 56% (n = 799) have MOH. The prevalence of MOH is 1.8% (95% CI 1.7–1.9). The mean age of onset was higher among men than women as well as among those with tension-type headache as primary headache compared to those who originally had migraine. A multivariate analysis showed that socioeconomic factors such as having a low level of education and/or a low household income were associated with MOH.
Conclusions: This is the first Swedish population-based study of MOH and we conclude that MOH is a significant public health problem in Sweden, as it is in other parts of the world.
Introduction
Medication overuse headache (MOH) is a recognized, worldwide health problem. It is a secondary chronic daily headache (CDH) that develops in individuals with primary headache who overuse acute headache medication. It is the third most common headache disorder after tension-type headache (TTH) and migraine (1).
Studies from other countries analysing MOH in the adult population have reported varying prevalences. In a recent Norwegian study the prevalence was 1.7%, and in a study from Spain it was 1.4% (2,3). MOH has been shown to affect 0.9% of the adults in Georgia and a recent German study demonstrated a prevalence of 1% (4,5).
Women are more prone to developing MOH than men, with a male:female ratio of about 1:3.5 (6). MOH is most prevalent in the forties and thus is particularly prevalent at ages when people are most productive, and it thereby affects productivity at work and work attendance (1,7). Earlier research from Norway and Turkey has shown that CDH is more prevalent among those with a low socioeconomic status (8,9). Atasoy et al. showed that MOH patients had a lower level of education than migraine patients (8). Hagen et al. found that low socioeconomic status was associated with CDH. They also found that the risk of CDH decreased with increasing income, but only among men (9). A German study observed a higher prevalence among Turkish immigrants than among native Germans (10).
In a Swedish study of headache among schoolchildren, Laurell et al. concluded that there had been a marked increase of headache during the last 40 years (11). The national pharmacy market has recently undergone an extensive deregulation process with the main aim of increasing the availability of medications. This process has already led to an increased consumption of over the counter (OTC) medications, analgesics included (12). In addition to this, several triptans (e.g. sumatriptan tablets and zolmitriptan nasal spray) have recently been released from prescription to OTC-sale in Sweden. In relation to similar decisions regarding triptans in the UK and in Germany, the risk of an increased incidence of MOH has been stressed (13). The topic of MOH is thus more relevant than ever in Sweden. However, the prevalence of MOH in Sweden is unknown. The aim of this study was therefore to estimate the prevalence of MOH in the general Swedish population and to analyze the occurrence of the disorder in different population groups.
Methods
Sampling
Data was collected through a national telephone survey conducted by SIFO Research International, a Swedish opinion poll agency. The survey is of a so called omnibus design. It runs continuously and provides means for data collection for various different research projects, companies and organisations. Sampling for this study was performed between March 2009 and March 2010 and consisted of randomized cluster sampling in two steps.
In the first step, a household was selected, and in the second step, a household member from that specific household was singled out. The basis for selection was the national telephone catalogue. A computer program randomly chose telephone numbers from the catalogue. It also constructed new telephone numbers by adding random digits to the chosen ones. This procedure ensured the inclusion of ex-directory telephone numbers. Households without telephones were not included. If there was no answer, if the number led to a company or a public authority, or if there was an unobtainable tone, a new number was chosen. When the interviewer came into contact with a household, he or she initially collected information on the number of household members aged ≥15 years and the computer program randomly chose one of these people for the interview.
Questionnaire
The questionnaire was administered by lay interviewers who had an average interviewing experience of 2 years. They introduced the interview by explaining that it was a survey from SIFO covering several different areas, lasting approximately 5–25 minutes. Verbal informed consent was obtained. All had a right to decline participation or to turn down specific questions without having to give an explanation. The study protocol was approved by the regional ethical review board in Gothenburg. All respondents were asked background questions concerning sex, age, educational level (elementary school, high school or university), house hold income, Swedish citizenship and main occupation (blue collar worker, white collar worker, pensioner, student, sick listed, unemployed or other), The term blue collar worker usually refers to employees who perform manual or technical labour, in contrast to white-collar workers, who do non-manual work, generally at a desk. The term sick-listed refers to all participants who stated sick leave as their main occupation, regardless of whether they were receiving sickness benefits or not.
The interviewers introduced the part of the survey that was specifically related to MOH by explaining that the questions concerned headache and came from the University of Gothenburg. This section of the survey began with two screening questions and only respondents who passed those were asked further questions about headache and medication use. Criteria to pass the screening were having headache present on ≥15 days/month and using medication for ≥10 days/month during the past 3 months. The subsequent interview comprised questions about headache and medication use.
Headache diagnoses were established, among participants only, according to criteria by the International Headache Society (IHS). The 2006 IHS appendix criteria were used to diagnose MOH (14). Medication overuse was defined as regular overuse for >3 months of one or more acute/symptomatic treatment medications, either a) ergotamine, triptans, opioids, or combination analgesic medications on ≥10 days/month or b) simple analgesics or any combination of ergotamine, triptans, analgesic opioids on ≥ 15 days/month without overuse of any single class alone. As a consequence of the diagnostic critera for MOH, we were also able to diagnose CDH, defined as ≥15 headache days/month during the past 3 months. This definition is part of the criteria for several CDH entities in the International Classification of Headache Disorders, 2nd edition (ICHD-2) (15). The primary headaches were diagnosed according to the ICHD-2 (15).
Statistical analysis
SPSS version 17.0 for Windows was used for all statistical analyses. Prevalences are presented as percentages with 95% confidence intervals (95% CI). The overall prevalence was standardized according to age (nine age groups), sex and working status (working/not working). The Swedish population aged ≥15 years in 2009 (7.8 million people) was used as the standard population. For the overall prevalence, both crude and standardized figures are presented. All other results in this article are based on crude data. Means are presented with standard deviations (SD) or 95% CI. Differences between means were tested using the independent samples t-test. Percentages were compared using the Pearson chi square or odds ratios (ORs). The significance level was set to p < 0.05. A multivariate logistic regression was performed, with MOH diagnosis as the dependent variable, socioeconomic factors (educational level, employment status, occupation, household income and Swedish citizenship) as independent variables and background variables (age and sex) as potential confounders. In the regression analysis, the occupation variable was split into two variables: employment status (working, pensioner, student, on sick leave, unemployed and other) and occupation (blue collar job, white collar job or other). The logistic regression was performed according to the procedures described by Hosmer and Lemeshow (16).
Results
Sample size and response rate
The sampling was performed by the method of substitution (the interviewer took a new number if there was no reply) and the total number of telephone calls was not documented. The dropout rate, defined as individuals who agreed to answer the overall interview but who declined answering the section regarding headache and medication use, was 1.6% (n = 700). In total, 44,300 people (24,195 women and 20,105 men) aged ≥15 years were interviewed. The mean age was 52.6 years.
Prevalences
Prevalence of MOH by sex and age

Mean ages in a sample of n = 799 (190 men and 609 women) individuals with MOH, aged ≥15 years

Significant at the 0.01 level between the sexes.
Headache history
Men were generally older than women at onset of primary headache as well as CDH (p < 0.001) (Table 2). A total of 12 individuals (1.5%) reported that the CDH had started at the age of 10 years or earlier (Figure 1). More than half (58.5%, n = 394) of those with MOH were classified as having had migraine as primary headache and 27.8% (n = 187) had originally had TTH. The mean time span between the onset of primary headache and chronification was 7.2 years (SD 11.1) and the respondents had suffered from CDH for an average of 14.3 years (SD 12.3). The time span between the onset of primary headache and chronification did not differ significantly between those with migraine versus those with TTH as primary headache (p = 0.07). However, those with TTH as primary headache were significantly older at onset of both primary and secondary headache (34.7 years and 41.1 years old) than those who had migraine as primary headache (23.5 years and 32.0 years old) (p < 0.001) (Figure 1).
Age of onset for primary and secondary headache in a cross-sectional sample of Swedes (n = 799, ≥15 years old) with MOH.
Medication overuse
The most commonly overused type of medication was simple analgesics. More than half (64.7%) of the participants reported simple analgesics as their main acute medication and the second largest group was combination analgesics (22.0%), followed by triptans (8.3%), opioids (4.1%) and ergotamine (0.9%). The most commonly used specific compound was paracetamol (n = 335, 41.9%), followed by the combination of acetylsalicylic acid and caffeine (n = 119, 14.9%) and ibuprofen (n = 106, 13.3%).
Socioeconomic distribution
Prevalence of MOH in different socioeconomic groups

The columns show the distribution throughout the entire sample (N = 44,300), among those with MOH (n = 799), and among men and women with MOH. *Significant difference at the 0.05 level between the sexes; **significant difference at the 0.01 level between the sexes.
Final model of logistic regression with MOH diagnosis as dependent variable, socioeconomic parameters as independent variables and background variables (sex and age) as possible confounders (n = 35,416)
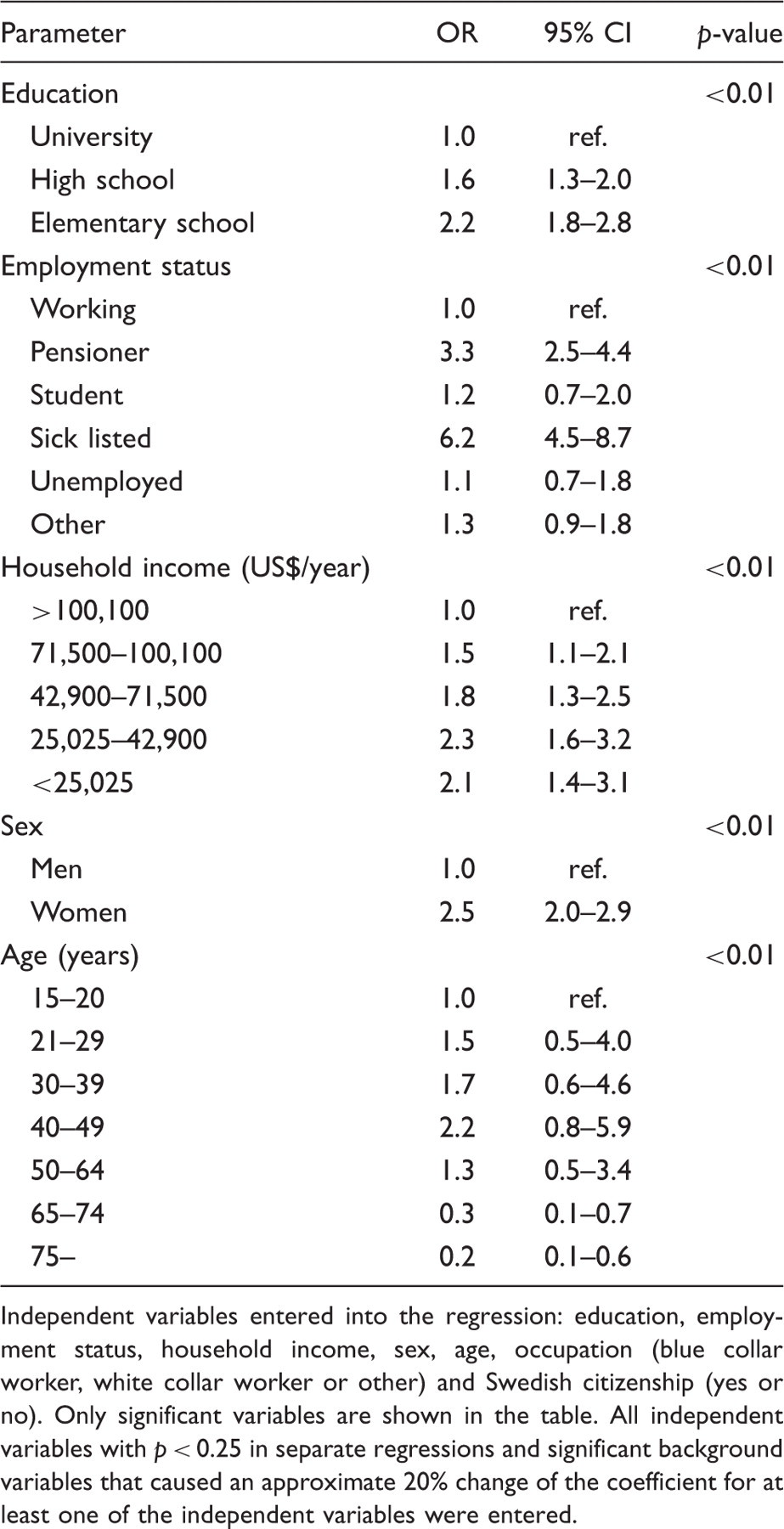
Independent variables entered into the regression: education, employment status, household income, sex, age, occupation (blue collar worker, white collar worker or other) and Swedish citizenship (yes or no). Only significant variables are shown in the table. All independent variables with p < 0.25 in separate regressions and significant background variables that caused an approximate 20% change of the coefficient for at least one of the independent variables were entered.
Discussion
This is the first Swedish population-based study of MOH. The prevalence of MOH is 1.8%, which represents approximately 140,000 Swedes. A multivariate analysis showed that socioeconomic factors such as having a low educational level, a low household income and another employment status than working are associated with MOH.
Results discussion
The prevalence of MOH in Sweden (1.8%) was similar to that found in a recent Norwegian population-based study (1.7%), which also applied the IHS 2006 appendix diagnostic criteria (2). However, that study included only 30–44 year olds, a group in which the prevalence is high. An even more recent Norwegian study that included all ages ≥20 years found a prevalence of 1.0% (17). It is, however, possible that this study slightly underestimated the prevalence because it did not include triptan-induced MOH (17). Other recent studies have shown a somewhat lower prevalence, for example 0.9% in Georgia and 1% in Germany (4,5). In the present study, the prevalence of CDH (3.2%) was slightly lower than in several other studies. The mean prevalence in Europe was recently calculated as 4% (18). The difference may, at least partly, be explained by the application of more strict diagnostic criteria in our study. We classified headache ≥15 days per month for ≥3 months as CDH, whereas most other studies defined it as headache ≥15 days per month regardless of the duration (18). Studies on CDH have shown that MOH occurs in 30–66% of those with CDH (3,19–21). This is in accordance with our finding (56%). Given that CDH is a major burden, it is remarkable that in among half of the sufferers, the disease may be an effect of medication overuse and thus both preventable and treatable. This calls for greater attention among health planners and improved information provision to patients at risk.
Retrospectively, 59% had migraine and 28% had TTH in our sample. These figures are in line with previous studies, for example a meta-analysis in which 56% had migraine and 27% had TTH (6). We used the ICHD-2 criteria and it should be noted that individuals who fulfilled the diagnosis for migraine were not investigated further for a TTH diagnosis. It is likely that several individuals with migraine had coexisting TTH, but our questionnaire could distinguish only one diagnosis in the same individual. The ICHD-2-criteria were adhered to, with the one exception that we did not ask for the duration of untreated attacks. Because of this, it is possible that individuals with cluster headache were classified as either migraine or TTH.
We made some interesting findings regarding the age of onset for primary and secondary headache. Firstly, men with MOH were significantly older than women with MOH at onset of both primary and secondary headache. This difference could not be explained simply by selection bias because the mean age was slightly higher for women than men in the entire sample (men: 52 years old, women: 53 years old). Secondly, those who had originally suffered from TTH were older at onset of both primary and secondary headaches than those who had originally suffered from migraine. The discrepancy between different primary headaches in the age of transformation to CDH has been noted previously in a Spanish study (3). The present findings of an earlier transformation among women and among migraineurs are logical given the overrepresentation of women and of migraineurs in the MOH population.
The use of medications that lead to MOH varies from country to country and is influenced by cultural factors (22). Paracetamol seems to be the most commonly overused substance among individuals with MOH in Scandinavia (1,23), which is further supported by the results of our study. The current situation in Sweden regarding the deregulation of the pharmacy market makes it even more urgent to establish a picture of the distribution of overuse. The fact that simple analgesics were most frequently overused clearly points to the importance of including pharmacies and other traders that sell OTC drugs in the preventive work against MOH.
The multivariate analysis included individuals with valid data on relevant variables. The analysis showed that socioeconomic factors such as having a low level of education, a low household income and another employment status than working were associated with MOH. There were interaction effects between some of the socioeconomic variables. This is not surprising because they all illustrate socioeconomic status, albeit in slightly different ways. This was a cross-sectional study and therefore it is not possible to draw conclusions about the direction of causality. We can only observe that the aforementioned associations exist. A relationship between MOH and low socioeconomic status has been suggested previously. Atasoy et al. found that low education was more common among those with MOH than among migraineurs in Turkey (8). Sweden is a country with rather modest socioeconomic inequalities. The Gini coefficient, which measures national income distribution, is 25, which is one of the lowest figures in the world (24). Despite this, the association between low socioeconomic status and increased risk of MOH was strong.
The prevalence of MOH was almost twice as high among women without Swedish citizenship as in women with Swedish citizenship. This difference could not be detected among men, probably owing to the limited sample size. In a previous German study, Kavuk et al. found that medication overuse was significantly more frequent among first generation Turkish immigrants than among German natives (10). In our study, the association between MOH and not having a Swedish citizenship was not significant after controlling for other socioeconomic factors (education, employment status and household income). Furthermore, the proportion of those with MOH who reported that they were born outside of Sweden was 11.8%, which is below the 16.0% that is normally reported for the general Swedish population (25). Thus, it is difficult to draw firm conclusions regarding immigrant status and MOH from our study.
Methodological considerations
A major methodological strength was the large sample size, which was based on the entire Swedish population aged ≥15 years. It is the first nationwide study of MOH in Scandinavia. The sample was somewhat skewed towards a larger proportion of women and elderly people compared with the general population. Therefore, an attempt was made to standardize the data according to age, sex and work status. However, as the adjustment had almost no effect on the over all prevalence of MOH, it was assumed that the survey sample could be considered representative of the general population. Thus, only crude figures are presented for all other analyses.
The response rate is unknown. The fact that the survey contained questions from other organizations and surveys as well as questions of the present study makes it less likely that potential non-response was specifically related to issues regarding headache or medication use. Having frequent headaches could affect the tendency to answer telephone surveys in two directions. On the one hand, one may have more time by the phone, but on the other, one may have phonophobia or be unable to leave bed. We can only speculate that this did not affect the conclusions.
A limitation of the present study was that the interviewers were not headache specialists. They were, however, experienced interviewers, a factor that has proven to be of importance for reliable prevalence estimates of migraine (26). We used the most recent diagnostic criteria for MOH, the IHS 2006 appendix criteria from 2006 (14). In a recent German study, which applied the same criteria (14), structured interviews performed by lay interviewers were validated against headache specialist ratings. The agreement between the classifications was found to be excellent. The kappa statistic which measures inter-rater agreement, was 0.945 (5). Similar validations were made in the Norwegian HUNT study, also using questionnaires based on the IHS 2006 appendix criteria (14). In comparison with headache specialist ratings, a specificity of ≥99% and a kappa statistic of ≥0.73 were found (27).
Conclusion
This is the first population-based study of MOH in Sweden and we conclude that MOH is a significant public health problem that is particularly prevalent among those with a low socioeconomic status. Information about the distribution of MOH in different sociodemographic and clinically distinct groups is important when planning preventive measures and identifying individuals at risk of developing MOH. We hope that the results presented here will be useful for future measures aimed at improving the situation for MOH sufferers in Sweden and elsewhere.
Footnotes
Funding
The work was supported by The National Corporation of Swedish Pharmacies’ fund for research and studies in health economics and social pharmacy.
Conflict of interest
ML is a member of an Allergan international advisory board and receives honoraria in connection with that work. PJ and TH declare that they have no conflict of interest.