
Abstract
Objectives
To study chronic headache and medication-overuse headache (MOH) prevalence; to identify groups with high prevalence of these conditions; and to identify the most frequently used pain medications among respondents with chronic headache.
Background
Chronic headache and MOH prevalence in Denmark were last estimated in 2010.
Methods
In this cross-sectional study, 104,950 individuals aged ≥16 years were randomly sampled for the 2017 Danish Capital Region Health Survey. Responses to questions about headache and use of acute pain medications were linked to demographic registries. MOH was defined as headache ≥15 days/month plus self-report of use of pain medications ≥10 or 15 days/month, in the last three months. Weighted prevalence proportions were calculated.
Results
Among 55,185 respondents, chronic headache prevalence was 3.0% (95% CI: 2.3–3.2) and MOH prevalence was 2.0% (95% CI: 1.8–2.1). Both conditions were more common among females and the middle-aged. Respondents on social welfare or receiving early retirement pensions had the highest prevalences. Among those with chronic headache, 44.7% overused over-the-counter analgesics for headache; paracetamol 41.5%; a combination of different pain relievers 25.3%; ibuprofen 21.9%; opioids 17.0%; combination preparations 14.3%; and triptans 9.1%.
Conclusions
The highest prevalence of chronic headache and MOH was seen among people with low socioeconomic position. Overuse of paracetamol was most common. Reported opioid use was higher than expected. Groups with high prevalence of MOH should be the focus of public health interventions on rational use of OTC and prescription pain medications.
Abbreviations
CPR: Central Person Registry; CRS: Civil Registration System; DK-CRHS: Danish Capital Region Health Survey; DNHS: The Danish National Health Survey; DNPR: Danish National Prescription Registry; GBD: Global Burden of Disease; LTB: Lifting The Burden: The Global Campaign against Headache; MOH: Medication-overuse headache; OTC: Over-the-counter; SEP: Socioeconomic position; TTH: Tension-type headache; YLDs: Years of life lost due to disability.
Introduction
The Global Burden of Disease (GBD) studies show that headaches are among the top causes of disability, calculated from an estimate of degree of disability, and years of life lived with short- or long-term health loss (1,2). One form of headache, medication-overuse headache (MOH) was ranked 18th in 2013, and 20th in 2015 (3,4). In the GBD analyses published in 2017–2018, MOH was not listed as a separate condition but as a contributor to the burden of migraine and tension-type headache (TTH). Adding on the disability attributed to MOH, migraine now ranks second highest in terms of years of life lost due to disability (YLDs) (5–7).
Despite the high prevalence, substantial morbidity, and cost of headache disorders (8), only 12% of countries include headache in their annual national health reports (9). MOH is a particularly difficult headache to study epidemiologically because data gathering fulfills only two of three diagnostic criteria: Frequency of headache (15 or more days per month in the last three months) and frequent intake of pain medications (10 or 15 days per month, depending on type or combination). The third criterion – exclusion of other causes of headache – requires gold standard methods of neurological evaluation and possibly ancillary examinations that are seldom done during surveys. There are, nonetheless, efforts to gather international data on MOH prevalence despite these challenges (10–36). Several of these studies conducted neurological evaluations (10–12,18,21). So far, only one population-based study has been able to estimate MOH incidence (0.72 per 1000 person-years) (23).
The latest estimate is that MOH afflicts about 60 million people worldwide (3,4). While MOH is not as prevalent as TTH or migraine, it is costlier both to the individual and to health care systems (8).
In Denmark, a large-scale study on chronic headache and MOH prevalence was first published in 2014 based on data from The Danish Capital Region Health Survey (DK-CRHS) and the Region Zealand Health Survey of 2010, two of five regions included in The Danish National Health Survey (DNHS). Data were linked to respondents' medication purchases recorded in the Danish National Prescription Registry (30). Estimated prevalence was 3.3% (95% CI: 3.2–3.5) for chronic headache and 1.8% (95% CI: 1.7–1.9) for MOH. The study identified groups with high prevalence of the condition; examined associations with possible determinants; supported local public health education efforts (37); and continues to guide health policy towards rational use of acute pain medications.
The primary objectives of this project were to study chronic headache and MOH prevalence in 2017; and to identify demographic groups with high prevalence of these conditions. The secondary objective was to identify the most frequently used pain medications among respondents with chronic headache.
Methods
The Capital Region Health Survey
This study is based on data from the DK-CRHS of 2017, a cross-sectional health survey conducted in 29 municipalities in the Capital Region of Denmark. The survey was conducted from February to May 2017 and was part of the DNHS (38). Both the DK-CRHS and the DNHS used uniform data collection methods and a random sampling design stratified by municipalities. A core of 53 questions was used in all five regions of Denmark. In 2017, questions on chronic headache were refined and questions on use of medication were added to the DK-CRHS. The main results of the DNHS are publicly available online www.danskernessundhed.dk (in Danish).
The sampling frame for the DK-CRHS included all adults in the Civil Registration System (CRS) aged ≥16 years residing in the Capital Region of Denmark as of 1 January 2017. Random samples of all these citizens were drawn from the CRS. During the sampling, participants' 10-digit Central Person Registry (CPR) numbers (39) were encrypted and replaced with 12-digit personal identification numbers. These 12-digit numbers were used consistently to link data from the DK-CRHS to national registers with information on age, sex, ethnicity, educational attainment, work status, and income (40).
Selected individuals received a mailed invitation and were invited to answer a self-administered questionnaire online, or a printed version. There were questions on socio-demography, health-related behaviour, physical and mental health status, chronic diseases including headache, and intake of over-the-counter (OTC) medications.
The sample size was 2450 persons per municipality except for Frederiksberg Municipality (4500 persons) and four other municipalities (4900 each from Gentofte, Gribskov, Høje Taastrup, and Rødovre). Copenhagen Municipality was divided into 10 areas treated as individual municipalities. A total of 104,950 questionnaires were sent. The response rate was 52.6% (55,185 respondents).
Definition of chronic headache and case ascertainment of MOH
The DK-CRHS monitored several common health complaints, and to what degree these were experienced by respondents. These common symptoms included headache, pain in different areas of the body, fatigue, sleep problems, depression, and anxiety. The current study focused only on headache symptoms in the last 14 days, to which the response options were “Yes, very disabling,” “Yes, slightly disabling,” and “No”. This question was used to gauge severity of headache.
Participants were asked how many days they experienced headache, on average, in the last three months. The options were: 0 days, 1–7 days, 8–14 days, and 15–30 days. Those who responded “15–30 days” were classified as having chronic headache. “Chronic headache” is not an independent diagnosis listed in the International Classification of Headache Disorders version 3 (ICHD-3). It is used in this paper as a descriptive term that corresponds to Criterion A for MOH (41).
Participants were then asked about their intake of pain medications per month in the last three months: OTC medications for any pain condition (headache, back pain, muscle/bone/joint pains, or other pains), specific medications (paracetamol, ibuprofen, combination preparations, opioids, triptans), and pain medications in general. Several commonly purchased brand names were listed with the generic names. The options were 0 days, 1–9 days, 10–14 days, and 15–30 days/month.
A case of MOH was defined as a respondent with chronic headache who also reported intake of paracetamol or ibuprofen ≥15 days per month, or combination preparations/opioids/triptans/unspecified pain medications ≥10 days per month; or any OTC medication for pain ≥15 days per month. This case definition approximates Criteria A and B of the ICHD-3 diagnostic criteria for MOH (41).
Demographic variables
Data from respondents were linked at the individual level to national registers with information on sex, age, civil status (married or registered partnership; separated or divorced; widow or widower; single), partnership status (living alone or living with partner), with/without children 15 years or younger living at home, and ethnicity (Danish; non-Danish western; non-Danish non-western).
Socioeconomic variables
Socioeconomic position (SEP) is a term that describes social and economic factors that “influence what positions individuals or groups hold within the structure of a society” and describes a range of “exposures, resources, and susceptibilities that may affect health” (42). Three measures of SEP – highest educational attainment, work status, and income – were retrieved from national registers. These specific aspects of SEP were considered as having independent and related effects as determinants of health (43).
Statistical analyses
Survey design weights were used to adjust for stratified sampling. Weights for possible differential non-response were applied based on age, sex, ethnicity, SEP factors (education, income, employment, civil status, and homeownership), and health factors (number of family physician and hospital visits). Weights were computed by Statistics Denmark (38,44).
For the primary objective, prevalence proportions for chronic headache, chronic headache without medication overuse (CHnoO), and MOH were calculated and weighted for stratified sampling and non-response. Chi-square tests were used to compare differences among demographic groups. p-values < 0.0007 were deemed significant, considering that 72 tests were done (i.e. Bonferroni correction 0.05/72).
For the secondary objective, data on pain medication use were summarized as proportions reporting intake of any OTC medication for pain (specifically for headache, back pain, muscle/bone/joint pains or other pains), paracetamol, ibuprofen, combination preparations, opioids, triptans, and other unspecified pain relievers. Cut-off points for overuse were either ≥15 days per month or ≥10 days per month depending on medication, in accordance with diagnostic criteria (41). Weighted proportions were calculated.
SAS software (version 9.4; SAS Institute, Cary, NC) was used. Proc surveyfreq was used for calculating prevalence proportions.
Ethical aspects
The goal of the DK-CRHS was stated on the questionnaire: To gather information on residents' health status to guide ongoing public health improvement efforts. Respondents were informed that supplementary information may be accessed from national registries. Participation was voluntary. Informed consent for use of data was given upon return of the questionnaire.
Researchers did not have access to the reference database containing individual identities (39,40).
The study was approved by the Danish Data Protection Agency according to the Danish Act on Processing of Personal Data (j.nr. 2012-58-0004, CSU-FCFS-2016-016). Approval from the Danish Health Research Ethics Committee System was not required because the project was based on data from questionnaires and registers and did not collect human biological samples.
Results
Prevalence of chronic headache and MOH
Of 55,185 respondents, 54,318 answered the question related to frequency of headache and 54,202 answered the question related to severity of headache. Among the latter respondents, 7.4% (95% CI: 7.1–7.7%) reported very disabling headache in the last 14 days, more commonly among females (10.1%; 95% CI: 9.7–10.5%) compared to males (4.5%; 95% CI: 4.2–4.9%) (p < 0.0001).
Chronic headache prevalence was estimated as 3.0% (95% CI: 2.8–3.2) and MOH prevalence 2.0% (95% CI: 1.8–2.1). Among the 1491 participants with chronic headache, 65.7% had MOH and 69.9% (95% CI: 67.1–72.8%) reported very disabling headache. Among the 991 participants with MOH, 74.1% (95% CI: 70.7–77.5%) reported very disabling headache.
Crude and weighted prevalence (95% CI) of chronic headache with and without medication overuse, by age and sex.

Note: Crude prevalence proportions were computed from cases divided by number of respondents. All other prevalence proportions were weighted for stratified sampling and non-response.
95% CI: 95% confidence intervals for weighted prevalence estimates (females + males); CHnoO: chronic headache without medication overuse; MOH: medication-overuse headache. p-values refer to results of chi-square tests. Prevalence proportions were weighted for stratified sampling and non-response.
Weighted prevalence (95% CI) of chronic headache with and without medication overuse, by demographic categories and socioeconomic position.

95% CI: confidence intervals for prevalence estimates (females + males); CHnoO: chronic headache without medication overuse; MOH: medication-overuse headache; USD: US dollars (1USD = 6.5DKK). All prevalence proportions were weighted for stratified sampling and non–response. p-values refer to results of chi-square tests comparing proportions across categories in each sociodemographic variable.
Chronic headache and MOH prevalences differed according to SEP; and were clearly more prevalent among those with low SEP (Table 2, all comparisons for these variables, p < 0.0001). The prevalence of CHnoO was not significantly different across the educational and income groups. It should be noted that the lowest gross annual income category (under USD 15,500) also included students receiving scholarships or working part-time.
Respondents on social welfare and early pensioners had the highest prevalence of both chronic headache and MOH. For chronic headache, prevalence among those on social welfare was 14.0% (95% CI: 11.7–16.3) and among early pensioners, 9.6% (95% CI: 7.7–11.5). For MOH, the highest prevalence was seen among people receiving social welfare benefits, 11.5% (95% CI: 9.4–13.6); and among those, prevalence was twice as high for women as men (14.6% and 7.7%, respectively). In contrast, CHnoO was most prevalent among women receiving sickness benefits (4.3%, Table 2).
In terms of civil status categories, there were no significant differences in chronic headache prevalence, but there was a significant difference for MOH prevalence among women (p < 0.0001), with the highest proportion among the separated or divorced in both sexes. There was no clear difference in MOH prevalence among either men or women who lived alone or with others, or whether they lived with children (Table 2).
Pain medications used by people with chronic headache
People with chronic headache had a markedly higher use of OTC pain medications compared to those without this condition. While it can be expected that they took more of these medications for headache, the data show that a much higher proportion of people with chronic headache also reported frequent use of OTC medications for other types of pain. A total of 44.7% (95% CI: 41.7–47.8) of respondents with chronic headache reported taking OTC analgesics 15–30 days/month for headache. They also reported frequent OTC analgesic use for other pain conditions (23.9%, 95% CI: 21.3–26.6), muscle/joint pains (22.6%, 95% CI: 20.0–25.1) and back pain (21.5%, 95% CI: 19.0–24.0).
Reported use of over-the-counter analgesics and specific medications among respondents with and without chronic headache and among those with MOH.
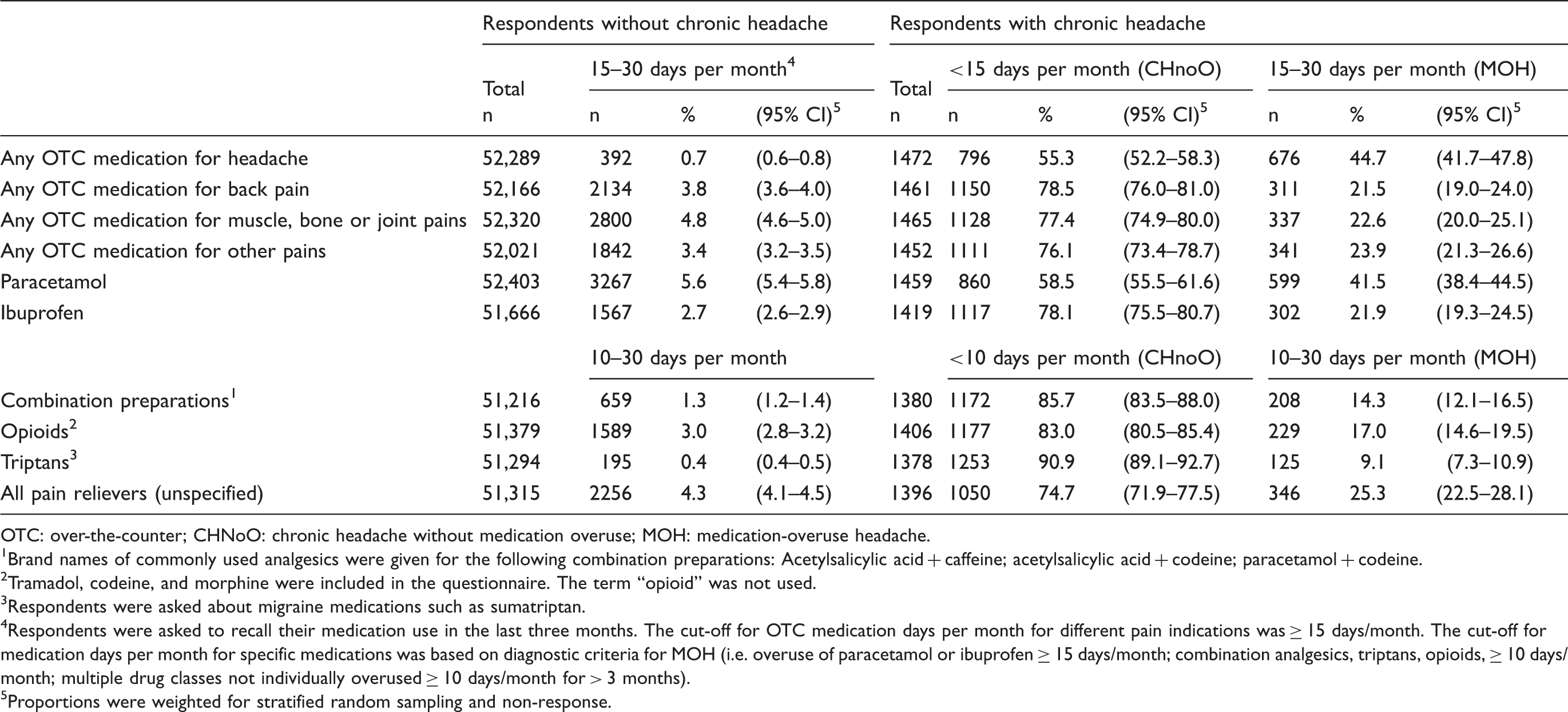
OTC: over-the-counter; CHNoO: chronic headache without medication overuse; MOH: medication-overuse headache.
Brand names of commonly used analgesics were given for the following combination preparations: Acetylsalicylic acid + caffeine; acetylsalicylic acid + codeine; paracetamol + codeine.
Tramadol, codeine, and morphine were included in the questionnaire. The term “opioid” was not used.
Respondents were asked about migraine medications such as sumatriptan.
Respondents were asked to recall their medication use in the last three months. The cut-off for OTC medication days per month for different pain indications was ≥ 15 days/month. The cut-off for medication days per month for specific medications was based on diagnostic criteria for MOH (i.e. overuse of paracetamol or ibuprofen ≥ 15 days/month; combination analgesics, triptans, opioids, ≥ 10 days/month; multiple drug classes not individually overused ≥ 10 days/month for > 3 months).
Proportions were weighted for stratified random sampling and non-response.
Discussion
Main findings
Our study presents updated estimates of chronic headache and MOH prevalence, and self-reported pain medication use among chronic headache sufferers in Denmark. Chronic headache was reported by 3.0% (95% CI: 2.8–3.2) and MOH by 2.0% (95% CI: 1.8–2.1), most frequently among women, the middle aged, non-ethnic Danes, and people with low SEP. Among those with chronic headache, the most commonly overused medication was paracetamol. There was a higher than expected use of opioids, considering that opioids are not recommended in the national treatment guidelines for headache (45).
These results should alert clinicians to high prevalence of headache and medication overuse in vulnerable groups, and the need to support strategies for appropriate public health messaging (37).
Current and previous prevalence estimates
The current prevalence estimates do not differ markedly from estimates based on 2010 survey data (chronic headache 3.3%; 95% CI: 3.2–3.5 and MOH 1.8%; 95% CI: 1.7–1.9) (30). However, the 2010 and 2017 surveys cannot be directly compared because the 2010 data were taken from respondents from two regions (The Capital Region and Region Zealand) and new questions or response categories were added to the 2017 questionnaire. Data on prescription medications were based on self-reports in 2017 but were accessed from the Danish National Prescription Registry (DNPR) (46) in the 2010 analysis, with overuse based on a cut-off for Defined Daily Doses.
Despite methodological differences, high prevalence of chronic headache and MOH among women, the middle aged, non-ethnic Danes and people with low SEP was consistently seen in both 2010 and 2017 surveys.
Those receiving social welfare benefits had the highest prevalence (for MOH, 11.0%, 95% CI: 8.1–13.9 in 2010 and 11.5%, 95% CI: 9.4–13.6 in 2017). The group with the next highest prevalence was early pensioners (for MOH, 7.5%, 95% CI: 6.3–8.8% in 2010 and 8.6%, 95% CI: 6.7–10.4 in 2017).
In both surveys, there was a clear income gradient starting from the second income category. The lowest income level included demographic groups with lower MOH prevalence: Young people 16–24 years (1.5% prevalence) and students (1.2% prevalence).
Neither survey showed differences according to partnership status, or whether the respondent had children living at home. Both surveys showed a higher prevalence of MOH among those who were divorced or separated (though differences according to civil status were not significant for both sexes in 2010 and for males in 2017).
A public health education campaign was carried out in Denmark based on the results of the earlier prevalence study (37). The campaign had a broad audience and was supported by the Association of Danish Pharmacies. All pharmacies displayed and distributed information about MOH during the campaign period, an important strategy for curbing prescription medication overuse, particularly opioids and triptans. The current study can guide the future targeting of groups with the highest burden of MOH, possibly focusing on ethnic minorities and those with unstable employment. There is evidence for the need to start prevention efforts among the young. Medication use for headache seems to track from adolescence into adulthood (50). Young Danes with low SEP and high perceived stress seem to be at higher risk (51).
Main findings compared to other studies
There are very few studies on MOH epidemiology worldwide, and many areas of the world do not have population-based data. Most MOH epidemiology studies report prevalence between 0.6 to 2.0% (10–36) The highest three reports are from Russia (7.2%) (27), Zambia (7.1%) (32), and Iran (4.9%) (28). With the exception of Nord-Trondelag in Norway, there are no attempts to track prevalence over time. Lifting the Burden: The Global Campaign against Headache has led efforts to gather new epidemiologic data. However, systems are not yet in place to conduct regular monitoring.
MOH prevalence in Denmark is higher than in Sweden (1.8%) (25) and Norway (0.8 to 1.0%) (23). The differences might be due to methodology. The Swedish survey was done using telephone interviews. The Norwegian survey was part of a longitudinal study and used interviews, questionnaires and prescription registry data.
As in several other studies, MOH prevalence was highest among women and the middle-aged (13,18,23,25,26). However, age distributions of MOH differ across countries. A study from India showed the opposite trend, with the lowest prevalence among the middle-aged (31). In Nepal (33) and Pakistan (35), the oldest age group had the highest prevalence. In Zambia, prevalence increased with age to as high as 23.8% among the oldest respondents (32). Whether these differences are due to study design, life expectancy, the nature of prevalent comorbid illnesses, patterns of medication consumption, types of medications used, availability of treatment for primary headaches, or biological differences remains unexplored.
In the current study, the prevalence of chronic headache and MOH was twice as high among female non-Danish non-western respondents compared to ethnic Danes; and four times as high among males. Similar findings have been described among migrants to other European countries – Sweden (25), the Netherlands (16), and Germany (47) – compared to the local population. It is not known whether the reasons for the differences are genetic, psychosocial or behavioral.
The most commonly overused medication is paracetamol, likely because it is readily available and inexpensive. The proportion of respondents with MOH who overused paracetamol (599 of 991 cases, 60.4%) is much higher than the 2011 report from Sweden (41.9%) (25). Triptan overuse among those with MOH (302 of 991 cases, 12.6%) is similar to the 2012 report from Norway (12%) (23). The proportion who overused opioids among those with MOH (229 of 991 cases, 23.1%) is high compared to Norway (16%) (23).
General differences in opioid use in Denmark, Sweden, and Norway are attributed to several factors. Norway has established national guidelines for the use of opioids to treat chronic non-cancer-related pain, which includes both pharmacological and non-pharmacological interventions. Furthermore, Norway has stricter criteria that must be met before a patient can receive reimbursement for opioids. Denmark's total consumption of opioids is higher but more stable over the years, whereas the other countries' consumption is slightly increasing. Tramadol use is higher in Denmark, while buprenorphine use is much lower (52). New guidelines on opioid prescription for non-cancer-related pain were published by the Danish Ministry of Health in 2018; that is, after the survey was conducted. It is possible that this will have an effect on opioid use in the future. It is not known whether these general trends in opioid use also apply to the subset of the population with chronic headache.
Implications for prevention and policy making
MOH is preventable and largely treatable. In the latest GBD analyses, MOH is not listed as a separate cause of disability. The burden of MOH has been added to the estimates for migraine and TTH based on a meta-analysis of studies reporting the proportions of MOH resulting from these two primary headaches (7). The authors explained that the main reason migraine climbed from the seventh largest cause of YLDs in GBD 2015 to the second in GBD 2016 was the reattribution of 70% of MOH burden as migraine burden; that is, a large portion of the disease burden attributable to MOH was shifted to migraine. GBD now describes migraine disability as being comprised of the ictal state, the interictal state, and MOH (7). The approach makes clinical sense because MOH, by definition, develops in people with a pre-existing headache disorder. It remains essential, however, that the medication overuse aspect of headache burden is highlighted. A significant proportion of the headache burden can be resolved by preventing and treating MOH.
The latest GBD analyses for migraine and TTH also found that a country's social development index (a compound measure based on income per capita, education, and fertility) is not a major determinant of the size of headache burden (7). Developed and developing nations all rank headaches among the top causes of disability. However, we found that even in a developed country such as Denmark with universal access to health care, there are socioeconomic determinants associated with chronic headache and MOH prevalence. The burden is highest among people with low income, low education, and unstable employment.
This cross-sectional study cannot show whether MOH leads to lower productivity, or whether the stress of unstable income leads to MOH. Our results support the findings of the Eurolight studies (8,36), which showed that useful time lost was substantial for those with probable MOH. Half (44.7% of males, 53.7% of females) reported loss of 20 days in the previous three months (8). These were days when work, household chores or family and social activities were lost completely, or with productivity reduced to <50% of expected.
Strengths and weaknesses
MOH is challenging to study epidemiologically. In surveys such as the current study, the case definition fulfills only two of three diagnostic criteria: Frequent headache and frequent intake of medications for acute relief of pain, but not the criterion regarding exclusion of other headache diagnoses. No gold-standard neurologic assessments or ancillary examinations were done to exclude other diagnoses. This might lead to an overestimation of prevalence.
Cross-sectional studies cannot show causation or rule out confounding by indication. Hence, the relationship between frequent headache and high medication use could be interpreted as ineffective therapy, where respondents, despite almost daily intake of pain medication, still suffer from headaches.
Causation in MOH is probably best illustrated by the early work of clinicians who described patients increasingly disabled by headaches despite aggressive use of pain medications, but who improved when these medications were discontinued (53). In this large-scale population-based study on headache, the purpose is neither diagnosis nor treatment. Rather, the focus is on needs assessment, improvement of health-care policy, and resource allocation (54). Without an attempt to estimate MOH prevalence, particularly the high burden of illness in certain segments of the population, it will be difficult to estimate resources required for improved headache care, including health education.
Non-response analysis for the DK-CRHS 2017 showed that women, people aged 55–79 years, with education beyond primary or secondary school, employed people, people living with a partner, with Danish ethnic background or high income, were more likely to participate in the survey. Furthermore, there were differences in response rate between municipalities, ranging from 41.9% to 62.9% (45). Possible differential non-response was adjusted for by using weights calculated by Statistics Denmark based on SEP variables and health factors (55).
Another limitation is that the current study does not include questions about headache characteristics that can be used to identify specific headache forms such as migraine and TTH (56).
Despite limitations, integrating headache epidemiological research in the DK-CRHS had several advantages: Large sample size, representative sampling, links to national registers, and the existence of a data gathering, management, and analysis infrastructure that could help ensure regular monitoring in the future.
Further research
Chronic headache and MOH epidemiology have been studied in few countries, and very little data are available on its prevalence among children (57). Future research should explore differences between countries in access to, and marketing of analgesics, attitudes towards taking pain medication for headache, and consumer/health care provider knowledge about MOH.
One possible focus for MOH prevention is reduction of opioid use among people reporting chronic headache. The prevalence of opioid use in the general Danish population is 4.5% overall, and 13.2% among individuals with chronic pain (48). The current study shows that among people with chronic headache, 17.0% reported overuse of opioids. Are opioids being prescribed inappropriately for headache, similar to trends for other chronic non-cancer pain conditions? Are opioids worsening the condition of people prone to headache who are being treated with opioids for other forms of chronic pain (58,59)?
The proportion of the sample population who reported triptan use is low (under 5%) considering that the estimated prevalence of migraine is 15% (60). The data point toward underutilization in the general population, but a tendency toward overuse among some triptan users. Further studies on patterns of triptan use are needed.
Large-scale epidemiologic studies on comorbidity or multimorbidity often leave out chronic headache as a unique disease state. Analysis of data on multiple co-occurring causes of morbidity could very easily miss associations with headache. In studies that used specific headache disorders as the index condition, associations between chronic headache and a range of disorders were shown (61,62). Comorbidity and multimorbidity are important to explore because of the problems of polypharmacy and drug interactions (63,64).
Conclusions
Chronic headache prevalence was estimated as 3.0% and MOH prevalence as 2.0%. The highest prevalence was seen among people with low SEP. Among those with chronic headache, overuse of paracetamol was most common. Reported opioid use among people with chronic headache was higher than expected. Groups with high prevalence of MOH should be the focus of public health interventions on rational use of OTC and prescription medications.
Footnotes
Public health relevance
The prevalence of medication-overuse headache (MOH) worldwide is 1 to 2%, although reports go as high as 7%.
In Denmark, MOH is more prevalent among women, the middle-aged, non-ethnic Danes, and people with low socio-economic position (short education, low income, receiving social benefits, or early pensioners).
Health education campaigns on the rational use of over-the-counter and prescription medications for pain should aim for a better understanding of the socioeconomic factors associated with medication overuse.
MOH is preventable. Preventing MOH reduces the burden of chronic headache.
Acknowledgements
Thanks to Anne Helms Andreasen, statistician at the Center for Clinical Research and Prevention, for checking the raw data and providing supplementary analyses.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MLW, CJL, KA and STG declare no conflict of interest. RJ has received honoraria as a speaker and/or conducted clinical trials for Allergan, ATI, Electrocore, and Pfizer.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Danish Capital Region Health Survey 2017 was funded by The Capital Region of Denmark. The analysis and report were funded by TRYG foundation.