
Abstract
Background
It is not well established to what extent medication-overuse occurs in cluster headache (CH), if medication-overuse headache exists in CH and whether the existing criteria for medication-overuse headache are a suitable diagnostic tool in CH. We aimed to examine the prevalence of medication-overuse and probable medication-overuse headache in a well characterized cohort of people with CH and describe associated factors and clinical impact.
Methods
Participants diagnosed with CH according to International Classification of Headache Disorders, 3rd edition (ICHD-3) beta and ICHD-3 were invited to participate in a semi-structured interview investigating medication-overuse and probable medication-overuse headache according to ICHD-3. To add nuance to the debate, we also included a more conservative definition, applying the ICHD-3 criteria for the medication-overuse but specified the headache phenotype to a daily bilateral headache.
Results
In total, 21% of 433 participants with CH had a medication-overuse according to ICHD-3. Of these, 16% fulfilled the criteria for probable medication-overuse headache according to the ICHD-3, and 12% if excluding isolated triptan overuse. The overused analgesics constituted simple analgesics (52.2%), triptans (37.3%), opioids (29.9%) and combination therapies (20.9%). Associated factors were having chronic CH (odds ratio = 11.4, p < 0.00001) and comorbid migraine (odds ratio = 2.35, p < 0.05). Participants with probable medication-overuse headache had longer attack duration (30.0 vs. 20.0 minutes, p < 0.01) and less effect of acute and preventive medication than those without (20.0 vs. 55.9%, p < 0.05 and 13.3 vs. 37.3%, p < 0.01, respectively). If applying the conservative definition with a daily bilateral headache along with a medication-overuse, the prevalence was reduced to 4%.
Conclusions
Probable medication-overuse headache was present in every sixth participant with CH in this large cross-sectional cohort study. Interestingly, only a smaller proportion was the result of isolated triptan overuse. In CH, where patients often suffer from daily attacks and may suffer from a daily bilateral inter-ictal pain, our very conservative definition noted a prevalence of 4%. While the existing ICHD-3 criteria for medication-overuse headache may not be directly applicable in CH, the applicability and validity of the very conservative definition warrant further investigation. Still, as in other cross-sectional populations with medication-overuse, we noted an association that acute and preventive treatments were less effective in participants with probable medication-overuse headache compared to those without. Altogether, future prospective studies are necessary to establish the exact extent and presentation of medication-overuse headache in CH and determine whether it is an aggravating factor for the disease. We do not recommend discontinuing triptans if suspecting MOH due to ethical concerns.
This is a visual representation of the abstract.
Introduction
Medication-overuse headache (MOH) is an acknowledged secondary headache in people with migraine and tension-type headache and is a major driver of chronification in these headaches (1). In cluster headache (CH), preventive treatments that are effective, well tolerated and fast acting remain limited, resulting in substantial burden for the individuals affected, their families and society (2). In contrast to migraine, the attack burden in episodic and chronic CH may vary greatly over time (3) and, consequently, the use of acute medication also varies. In people with episodic CH, for example, triptans are intuitively discontinued in the remission periods where they are attack-free. This may naturally prevent the development of MOH in some, but, if the bouts are long, if attacks occur continuously, as in chronic CH, or if analgesics are used daily for other pain disorders, it remains unknown whether a MOH can develop in people with CH. The transition of episodic to chronic CH is seen in 12% in a five-year period, and, so far, no reasons have been identified (3). Being a potential driver of chronification in other headache disorders, it is important to assess the role of medication-overuse in CH as well.
So far, only a few case series and one cohort study have investigated the effects of medication-overuse in CH; thus, the clinical characteristics of a MOH in CH is not well understood. In two of the prior case series with ergotamine overuse and sumatriptan overuse, a diffuse background headache was observed (4,5), which resolved after withdrawal of the overused medication. Other case series reported worsening of the CH itself due to overuse of sumatriptan (5–9), which also resolved in most cases after withdrawal (5,6,9). A declining effect of sumatriptan was described in people with several daily administrations of sumatriptan over a two-year period (10). Unfortunately, other headache symptoms were not reported because the focus was on adverse events related to daily sumatriptan overuse. Lastly, medication-overuse and a diffuse daily headache were observed in 4% of the CH population at a British headache clinic(11); notably, all had a comorbid migraine or a family disposition to migraine and improvement was seen in 13/17 participants.
In the present study, we hypothesized that chronic headache or a daily bilateral headache can occur in people with CH and an overuse of analgesics for more than three months, as indicators of a MOH, with a potential risk factor being comorbid migraine.
On this background, we aimed to assess the prevalence of medication-overuse along with firstly a probable MOH (pMOH) according to ICDH-3 and, secondly, a conservative definition of MOH with a daily bilateral headache (cMOH) in a large retrospective cohort of people diagnosed with CH. Additionally, we aimed to describe associated factors, and the types of medication most frequently overused.
Methods
Participants
The present study is an observational, retrospective, cross-sectional cohort study including people diagnosed with CH according to International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria (1). Patients were recruited from the Danish Headache Center, a tertiary headache facility from November 2022 to December 2023. All participants originally participated in a genetic study (H-2-2010-122) (12) but were contacted anew to follow up on the transition of CH phenotype.(3) On this occasion, questions on medication-overuse were included. Data were collected as a semi-structured interview by telephone. Inclusion criteria were a diagnosis of CH according to ICHD-3 beta or ICDH-3 (1,13), which was validated by a headache specialist or trained medical student in during the interview. In addition, patients were asked if they were known with comorbid primary headache disorders as tension-type headache and/or migraine. If they were, the diagnosis was validated according to ICHD-3 (1) and it was secured that patients could tell these attacks apart from their CH attacks. There were no other exclusion criteria. Study size was not calculated because patients were recruited consecutively from 2017–2021 with the purpose of including as many as possible.
Interview
The questionnaire was made by the investigators and is described in detail in a previous publication (3). For the section on MOH, one of the investigators who was a MOH expert (LNC) assisted with the design of the questionnaire. The semi-structured interview was divided into eight sectors: Verification of diagnosis, CH phenotype, phenotype transition, medical treatment, CH attack variants, CH background headache, MOH and selected comorbidities. It was estimated that people could complete the interview in 30 minutes. Interviews were performed by two of the investigators (MKS and ASP) and three trained medical students, with the possibility to consult ASP in case of ambiguities.
Outcomes
The primary outcome was prevalence of medication-overuse and pMOH. The medication-overuse could be of either simple analgesics ≥15 days per month, triptans ≥10 days per month, opioids ≥10 days per month, combination therapies ≥10 days per month or an overuse of a combination of these drug types not individually overused for ≥10 days per month (1). None of the participants was on ergotamine. pMOH was assessed according to its definition under the comments of MOH in the ICHD-3 criteria (1) as having a chronic headache (unspecified headache ≥15 days per month) and a regular medication-overuse longer than three months. Criterion C “not better accounted for by another ICHD-3 diagnosis” is limited by the fact that the patients may simply fulfil this criterion based on having CH attacks on ≥15 days per month. This has been discussed in more detail in the Discussion. To include a conservative approach, cMOH, comprising prevalence of a daily bilateral headache with a medication-overuse for longer than three months, was also calculated, from reports of a featureless, bilateral headache between CH attacks and subsequent reports that it occurred daily. Secondary outcomes included relevant clinical variables, and the type and frequency of the medications overused. To assess whether a family disposition to migraine was associated with having pMOH and cMOH, data from the original genetics study were assessed (12). We calculated the prevalence based on data solely for those participants that were also included in the current follow-up study.
Statistical analysis
Data were collected and managed using REDCap electronic data capture tools hosted by the Capital Region of Denmark (14,15). Analyses were performed using R software, version 4.3.0 (R Foundation, Vienna, Austria). Missing data were minimal because data were derived from structured interviews. The mean ± SD and median ± IQR were used as appropriate to describe the distribution of continuous variables and significance was evaluated by Student’s t-test or the Wilcoxon rank sum test. The chi-squared test was used to compare categorical variables, unless n < 5, where Fisher’s exact test was used. Lastly, pre-defined relevant variables were included in multiple logistic regression analyses (sex, age, CH phenotype and comorbid migraine). p < 0.05 (two-tailed) was considered statistically significant.
Patient consent and registration
All participants gave their verbal and written consent according to the Declaration of Helsinki. The study did not need formal ethics approval according to Danish law because it was a non-interventional study, but it was still reported to the ethics committee (F-22048470). The study was approved by the Danish Protection Agency (P-2022-607). Genetic disposition to migraine was merged from the original genetic study was approved by both the Capital Region of Denmark Ethical Committee (H-22010122) and by the Danish data protection agency
Results
In total, 546 people with CH were invited to participate in this cohort study. Of those invited, 433 participated in the semi-structured interview, resulting in a response rate of 79% (Figure 1). Most had episodic CH (n = 283; 65%), the male:female ratio was 2.1:1 and the mean ± SD age was 52 ± 21.0 years. The mean ± SD treated attack duration was 25.0 ± 30.0 minutes and the mean ± SD weekly attack frequency was 9.0 ± 17.0. For those with episodic CH, the mean ± SD bout length was 5.0 ± 5.0 weeks. Only 125 (29%) were on one/several types of preventive medication at the time of the interview. Most were on verapamil (n = 92; 21%), followed by gabapentin (n = 15; 3%), candesartan (n = 13; 3%), CGRP-antibodies (n = 12; 3%), indomethacin (n = 8; 2%), occipital nerve stimulation (n = 7; 2%), lithium (n = 6; 1%), topiramate (n = 6; 1%) and sphenopalatine ganglion stimulation (n = 4; 1%).

Flowchart of the study. CH = cluster headache.
Probable medication-overuse headache according to ICHD-3 criteria
Every fifth patient (21%) of the cohort fulfilled the criteria for having a medication-overuse. Of these, 67 (16%) fulfilled the ICHD-3 criteria of pMOH with a male:female ratio of 1:1 and 54 (81%) had chronic CH. The demographic and clinical characteristics of participants with and without pMOH according to ICHD-3 are presented in Tables 1 and 2.
Description of participants with cluster headache with and without probable medication-overuse headache (pMOH).
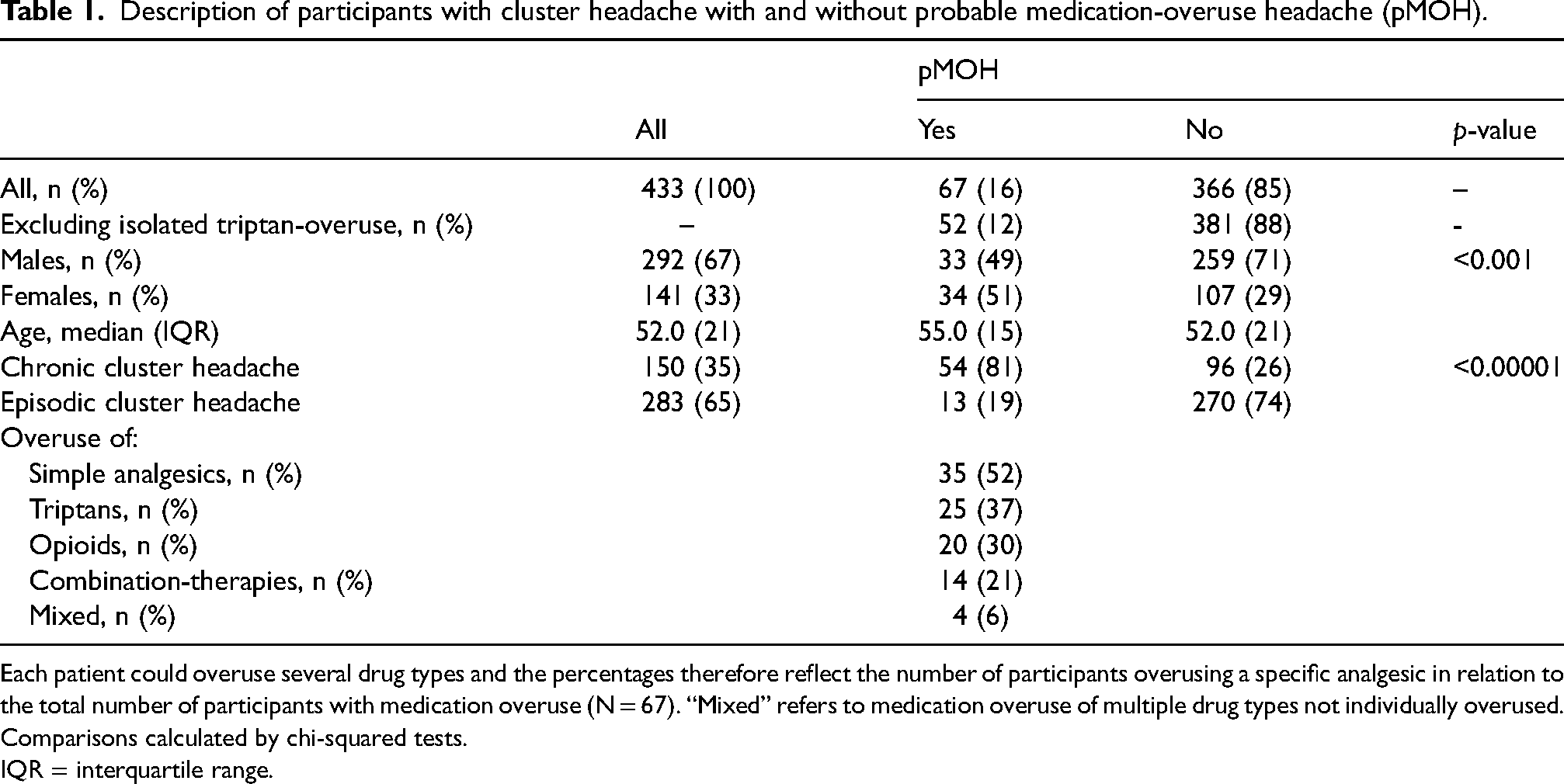
Each patient could overuse several drug types and the percentages therefore reflect the number of participants overusing a specific analgesic in relation to the total number of participants with medication overuse (N = 67). “Mixed” refers to medication overuse of multiple drug types not individually overused. Comparisons calculated by chi-squared tests.
IQR = interquartile range.
Clinical characteristics of participants with cluster headache with and without probable medication-overuse headache (pMOH).

1: defined as ≥75% reduction of pain intensity by preventive treatment. 2: defined as ≥75% reduction of attack frequency by preventive treatment. 3: defined as ≥75% reduction of pain intensity in more than 50% of attacks by acute medication. Significance was evaluated by Wilcoxon rask sum test. A chi-squared test was used to compare categorical variables.
IQR = interquartile range.
The most frequently overused types of analgesic were simple analgesics (n = 35; 52%) as paracetamol and non-steroidal anti-inflammatory drugs, followed by triptans (n = 25; 37%), opioids (n = 20; 29.9%), combination therapies (n = 14; 21%) and multiple drug types not individually overused (n = 4; 6%). As many as 27 (40%) with pMOH had an overuse of multiple types of analgesics. Isolated triptan overuse constituted 15 of the 67, equivalent to 3% of the entire cohort.
Of clinically relevant factors, participants with pMOH had a longer attack duration for treated attacks than participants without pMOH (30.0 vs. 20.0 minutes, p < 0.01), whereas the mean attack frequency and bout duration did not differ (10.5 vs. 7.0 attacks per week, not significant, and 4.0 vs. 5.0 weeks, not significant). In relation to treatment effect, fewer with pMOH reported a good efficacy on pain intensity by acute treatment (20 vs. 56%, p < 0.05) and on attack frequency by preventive medication (13 vs. 37%, p < 0.01). Reported efficacy on pain intensity by preventive medication did not differ among participants with and without pMOH (23 vs. 34%, not significant). The prevalence of oxygen-users did not differ significantly between groups (43% in pMOH vs. 53% in those without, not significant).
Comorbid migraine was present in twice as many with pMOH compared to those without pMOH (30% vs. 14%, p < 0.01), whereas the prevalence of tension-type headache did not differ between the groups (19% vs. 11%, not significant). In total, as many as 40 (60%) of those with pMOH did not have either a comorbid migraine or tension-type headache. If excluding those with chronic CH as well as migraine and tension-type headache, only five participants with pMOH remained (8%). In a logistic regression model, chronic CH was strongly associated with having pMOH (odds ratio = 11.4, 95% confidence interval = 6.0–23.1, p < 0.01), as was comorbid migraine (odds ratio = 2.35, 95% confidence interval = 1.1–5.0, p < 0.05), whereas the effect of age and sex did not predict the outcome (Table 3). A family disposition to migraine was present in 58% of participants with pMOH and only in 41% without (not significant).
Multivariable regression model of variables associated with probable medication-overuse headache (pMOH).
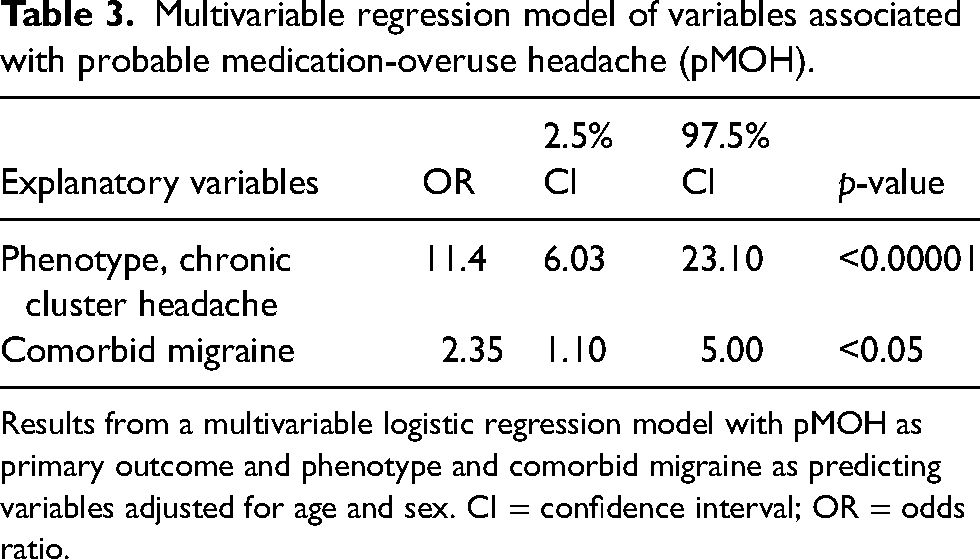
Results from a multivariable logistic regression model with pMOH as primary outcome and phenotype and comorbid migraine as predicting variables adjusted for age and sex. CI = confidence interval; OR = odds ratio.
Medication-overuse and a daily bilateral headache
To include a more conservative approach, we also investigated the combination of having a medication-overuse and a daily bilateral headache, cMOH. This was seen in 19 (4%) of participants, and in 17 (4%) if excluding an isolated triptan overuse. The male:female ratio for cMOH was 1:1.4 and 74% had chronic CH. A family disposition to migraine was present in 52% of participants with cMOH and only in 40% without. The prevalence of oxygen-users differed between groups with only 26% using oxygen among those with cMOH compared to 53% among those without (not significant). A daily bilateral headache was seen in 40 participants altogether.
Discussion
In this interview-based, cross-sectional cohort study of 433 participants with CH, we explored medication-overuse and pMOH in CH to obtain an impression of the clinical relevance, as existing literature in this area is extremely sparse. If applying the criteria directly from the ICHD-3, our findings suggest that a pMOH is present in 16% of people with CH, and that isolated triptan overuse only accounts for a smaller proportion of the overuse. Yet, as the “true” presentation of a MOH in CH remains unclear, we also investigated a more conservative definition being the presence of medication-overuse and a daily bilateral headache, cMOH, which occurred in 4%. Our data indicate a clinically relevant, lower subjective medication response in people with pMOH compared to those without and finally, chronic CH and comorbid migraine were identified as associated factors.
Why assess MOH in CH?
MOH is most well recognized in migraine and tension-type headache, whereas knowledge of MOH in CH is sparse. MOH is present in 2–3% of the general population,(16,17) but is diagnosed in 33% of people referred with chronic migraine to a tertiary headache clinic (18). Our understanding of what causes MOH is incomplete, but a pre-existing headache is necessary because people without such do not appear to develop MOH even if they overuse analgesics (19). Acute headache medications are considered to alter brain circuits, thereby increasing the vulnerability to attacks of the existing headache and, with time, result in MOH (20). Pre-clinical and neuroimaging studies have revealed changes in several brain structures, including the hippocampus, periaqueductal grey matter, posterior cingulate cortex, thalamus, cerebellum, orbitofrontal cortex and mesocorticolimbic system (20). Interestingly, the alterations normalized after withdrawal of the overused analgesic. Pre-clinical studies have also demonstrated that short- and long-term use of acute medication (e.g. opioids, triptans and ditans) resulted in altered pain perception (20) and, recently, a translational study has shown that over-the counter-analgesics repressed anti-Müllerian hormone levels (21). Despite none of these studies being performed in people with CH, the effect of analgesics on the brain would be expected to be comparable, considering the pathophysiological overlaps (22). Eventually, this would be interesting to explore further.
The limited data on medication-overuse and MOH in CH could be a concern because it would be ethically problematic to deprive patients from using triptans due to the extreme severity of the attacks. Therefore, it is important to emphasize that this was not the intention of the present study. Yet, MOH in migraine and tension-type headache is associated with increased disease burden and a higher rate of depression and anxiety (23,24). Because data on the consequences of a medication-overuse in CH are limited, a first step is to investigate whether MOH also exists in CH, if there could be a causal relation, and if it is associated with poorer clinical presentation. Thereafter, longitudinal studies and RCTs are needed to explore the relation further.
MOH in CH: Is it a problem?
To our knowledge, only one study deriving from a British tertiary headache clinic has reported a prevalence of possible MOH in CH. The ICHD criteria were not applied, but, instead, MOH was defined as the co-existence of a medication-overuse and a daily headache. The study found a prevalence of 17 (4%) of 430 people and most presented with a bilateral, dull headache (unilateral only in 3/17) (11). This prevalence is comparable to our cMOH in 4%. In line with MOH populations in migraine and tension-type headache (19), we observed a female disposition, and the male:female ratio among CH participants with a MOH was reduced to 1:1 from 2:1.
The reported characteristics of MOH in CH differ between the existing studies. Some have suggested a de novo headache (described as a diffuse bilateral headache or a chronic daily headache) (4,5,11) and others a worsening of the CH itself with increased attack frequency (5,6,8,9,25) and bout length (5). A poorer efficacy of acute medication with time was observed in 42% of 53 people with chronic CH using a minimum of two daily dosages of sumatriptan for at least two years (10). This relates well with our findings because subjectively rated acute and preventive treatment response was significantly worse in participants with pMOH. Furthermore, we also observed that fewer with cMOH used oxygen. This could either reflect a loss of efficacy among those with cMOH or that participants with an effect of oxygen are less prone to develop a medication-overuse. The same tendency was seen in participants with pMOH, although it did not reach significance. Overall, the findings are in line with the existing literature on MOH in general, where it is well documented that withdrawal not only significantly reduces the number of headache days per month and the use of acute medications, but also results in better treatment effect for the primary headache (26–30) In three case studies of people with CH and MOH, as well as in the British cohort study, withdrawal was described as successful, suggesting that withdrawal could also be beneficial in CH (5,6,9,11).
Due to the cross-sectional nature of the data, we cannot conclude on the causality of medication overuse in the present study. Taken together, prospective research is necessary for furthering our understanding of the effects of a medication-overuse in CH and of possible treatment strategies.
The role of comorbid migraine
A co-existing migraine or a family disposition to migraine have been speculated to be necessary for MOH to develop in CH (28,31), as this was the case for all 17 people with MOH in the British cohort (11). Importantly, we can confirm that migraine was a significant risk factor. However, as many as 60% of our patients with pMOH did not have a concurrent migraine or tension-type headache. Numerically, our findings support that half of these patients had a family disposition to migraine, but not all.
Overused analgesics
In the present study, simple analgesics, followed by triptans and opioids accounted for the highest use among those with pMOH, which was unexpected because simple analgesics and opioids are not effective for CH and therefore are not recommended (32,33). Indeed, the overused analgesics follow the well-known patterns seen in migraine and tension-type headache (19). In principle, they could be used for pain-related comorbid diseases that are also known to occur frequently in CH patients (34), although the overuse of simple analgesics and opioids could also reflect inappropriate treatment of the CH to minimize the daily amount of triptans, due to the recommended maximum of two daily dosages or high costs. Therefore, the present study adds to the growing evidence of an unmet need for proper preventive treatment for CH.
Are the ICHD-3 criteria suitable to assess MOH in CH?
The unpredictable nature of CH with its high variability of disease burden over time for both episodic and chronic patients (35,36) challenges the direct usage of the ICHD-3 MOH criteria for CH. An example could be a patient with episodic CH with four months with daily attacks and a daily use of triptans. If the bouts normally lasted two to three months or the attack frequency was higher than normal, a MOH diagnoses could be speculated based on the impression of a clinical worsening along with a medication-overuse. However, it is also possible that the worsening is simply due to the natural course of the disease. In addition, the fact that attacks often occur daily limits the applicability of the ICHD-3 MOH criteria for CH.
By contrast, the very conservative approach, addressing cMOH, expectedly, showed a much lower prevalence. This approach presumes that MOH in CH presents with a daily bilateral phenotype, which we found was only the case for 4%. However, our data and the existing literature suggest that a daily bilateral headache is not specific for MOH (36). On the other hand, a chronic or daily bilateral headache could also be due to stress and sleep disturbances such as sleep deprivation, insomnia or disturbances in circadian rhythm in addition to a milder inter-ictal pain. In the case of MOH in CH, conclusive evidence may only be provided by discontinuation of the overused analgesic in a randomized and prospective study. Again, one should consider allowing overuse of triptans for ethical reasons in such a study, whereas simple analgesics and opioids that are not indicated for the treatment of CH should be discontinued.
Strengths and limitations
The questionnaire was performed on a validated cohort of people with CH, which is a major strength of the present study along with the sample size and high response rate of 78%. The semi-structured interview allowed for clarification of insecurities that would not be possible in an internet-based questionnaire. The main limitation of the study is the cross-sectional design, which does not allow causality to be assessed. Therefore, we applied the terminology pMOH as suggested in the comments section of the ICHD-2 MOH criteria. Other limitations include selection bias in that the participants derived from a tertiary headache clinic, as well as the retrospective design of the study introducing a risk of recall bias. In addition, it was not systematically assessed whether people with episodic CH were in bout or in remission at the time of interview. Lastly, the study is limited by the lack of consensus concerning MOH in CH. We attempted to accommodate this by calculating the prevalence via application of the ICHD-3 criteria for pMOH and the conservative criteria with a daily, bilateral headache, the latter being more in line with the British cohort study, aiming to make the findings comparable (11). Still, we cannot exclude the possibility that participants with inter-ictal pain, or pain due to undiagnosed co-morbidities or side effects, may have been assessed as having pMOH or cMOH.
Conclusions
The present study finds that probable medication-overuse headache is present in every sixth person with CH and that isolated triptan overuse only accounts for a smaller proportion in this large, retrospectively investigated cohort deriving from a tertiary headache clinic. Our findings are interesting because, unexpectedly, simple analgesics were the most frequently overused medication, a treatment not indicated for CH. Chronic CH was strongly associated with pMOH, as was the previously suggested association with comorbid migraine. In line with other MOH populations, pMOH was also associated with a worse clinical presentation in relation to treated attack duration, pain reduction by acute medication and effect on frequency by preventives. Yet, the study also highlights that the ICHD-3 criteria may not be suitable for defining MOH in CH as a result of the often daily attack occurrence in CH. A conservative approach, with medication-overuse and a daily bilateral headache, cMOH, occurred in 4% of participants. This approach is limited by assuming that a MOH would present with bilateral headache, but includes the risk of including patients with inter-ictal pain or headache due to undiagnosed comorbidities. Overall, these findings urge further prospective research to establish the extent and presentation of MOH in CH. Importantly, we do not recommend the discontinuation on triptans if suspecting medication-overuse for ethical concerns.
Article highlights
Probable medication-overuse headache according to ICHD-3 was seen in 16% of people with CH, and if excluding isolated triptan overuse in 12%.
A more conservative definition requiring a daily bilateral headache was present in 4%.
Probable medication-overuse headache was associated with chronic CH and comorbid migraine, and with worse effect of acute and preventive treatment.
Footnotes
Data availability
The deidentified data supporting the findings are available from the corresponding author upon reasonable request.
Declaration of conflicts of interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: NL received a personal research grant from the Capital Regions Research Foundation and has received personal payment for lectures on headache for general practitioners from Pfizer and Dagens Medicin, and from teaching activities for Viatris. NL has participated in a two-day neurological symposium sponsored by Lundbeck Pharma and her institution received a restricted research grant from Lundbeck Pharma. MLKS’s institution received a restricted research grant from Lundbeck Pharma. LNC has nothing to declare. RHJ’s institution received a restricted research grant from Lundbeck Pharma and Novo Nordisk Foundation. She is principal investigator in clinical trials, and has given lectures to TEVA, Lundbeck Pharma, AbbVie, Pfizer and Eli Lilly. She is also Director of Danish Headache Center, Director in Lifting The Global Burden (unpaid), Chair of Master of Headache Disorders at University of Copenhagen (personal payment). ASP has received personal payment for lectures on headache for general practitioners from Pfizer, she has participated in a two-day neurological symposium sponsored by Lundbeck Pharma, and her institution received a restricted research grant from Lundbeck Pharma.
Ethical statement
All participants provided their verbal and written consent according to the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.