
Abstract
Objective:
To identify factors associated with early angiographic reperfusion improvement (EARI) following intra-arterial fibrinolytics (IAF) after failed or incomplete mechanical thrombectomy (MT).
Methods:
A subset of patients treated with MT and IAF rescue after incomplete reperfusion included in the INFINITY (INtra-arterial FIbriNolytics In ThrombectomY) multicenter observational registry was analyzed. Multivariable logistic regression was used to identify factors associated with EARI. Heterogeneity of the clinical effect of EARI on functional independence (defined as modified Rankin Score ≤2) was tested with interaction terms.
Results:
A total of 228 patients (median age: 72 years, 44.1% female) received IAF as rescue for failed or incomplete MT and had a post-fibrinolytic angiographic control run available (50.9% EARI). A cardioembolic stroke origin (adjusted odds ratio (aOR) 3.72, 95% confidence interval (CI) 1.39–10.0) and shorter groin puncture to IAF intervals (aOR 0.82, 95% CI 0.71–0.95 per 15-min delay) were associated with EARI, while pre-interventional thrombolysis showed no association (aOR 1.15, 95% CI 0.59–2.26). The clinical benefit of EARI after IAF seemed more pronounced in patients without or only minor early ischemic changes (Alberta Stroke Program Early Computed Tomography Score (ASPECTS) ≥9, aOR 4.00, 95% CI 1.37–11.61) and was absent in patients with moderate to severe ischemic changes (ASPECTS ≤8, aOR 0.94, 95% CI 0.27–3.27, p for interaction: 0.095).
Conclusion:
Early rescue and a cardioembolic stroke origin were associated with more frequent EARI after IAF. The clinical effect of EARI seemed reduced in patients with already established infarcts. If confirmed, these findings can help to inform patient selection and inclusion criteria for randomized-controlled trials evaluating IAF as rescue after MT.
Introduction
Incomplete or failed reperfusion reduces the clinical benefit of mechanical thrombectomy (MT). 1– 5 One bailout strategy to improve reperfusion after failed or incomplete MT is the intra-arterial administration of fibrinolytics (IAF). 6 –8
Current guidelines state that it is reasonable to use salvageable technical adjuncts to achieve successful or complete reperfusion 9,10 and according to recent survey results, IAF is used by a considerable number of interventionalists. 11 Previous studies have shown that IAF may be a safe rescue approach after MT 6,8,12 –15 and recently published data from the INtra-arterial FIbriNolytics In ThrombectomY (INFINITY) registry suggested that early angiographic reperfusion after IAF is associated with better clinical outcomes. 16 While recent reports were generally positive, it is unknown which patients are more likely to respond to IAF rescue and in which patients’ early angiographic reperfusion improvement (EARI) translates into clinical benefit. For the deciding physicians in charge, it would be useful to know which patients are more likely to benefit from additional reperfusion improvement, because in these patients additional rescue therapies seem more justified. 17
Aim of this subanalysis of the multicenter INFINITY registry was to report on factors associated with early reperfusion improvement after IAF as rescue for MT. Moreover, we evaluated if the clinical benefit of early reperfusion improvement was heterogenous across predefined strata of patient characteristics in order to find subpopulations less or more likely to benefit from IAF rescue.
Methods
Patients
Details of the INFINITY registry have been published before. 16 In short, 10 European tertiary care centers provided individual patient data of consecutive patients treated with MT and received additional IAF (Supplementary Table I). Inclusion criteria were patients presenting with an internal carotid artery or middle cerebral artery (first or second segment) occlusion, who were treated with second-generation MT and intra-arterial (IA) urokinase or alteplase. A total of 311 patients were included in the registry. Consent was waived according to the retrospective nature of the work, or patients gave their written or oral consent, depending on the centers ethical and institutional guidelines. All centers obtained ethical approval from the respective local ethics committee. Functional outcome was assessed at 3 months using the modified Rankin Scale, with functional independence defined as modified Rankin Scale ≤2. In this subanalysis, only patients who received IAF with the intention to improve reperfusion of the target territory after MT (250/311) and available early angiographic follow-up were included (228/250).
Image analysis
Image analysis was performed locally at each participating site by a neurointerventionalist. After administration of IAF after MT, angiographic reperfusion improvement was defined as a reduction of capillary phase deficit by newly established antegrade flow in the new target territory (i.e. the residual hypoperfused area after MT). By definition, any angiographic reperfusion improvement could, therefore, include cases with and without a thrombolysis in cerebral infarction (TICI) grade change according to the initial target territory. These angiographic data were available in N = 228/250 patients with attempted rescue of a failed or incomplete reperfusion (TICI 0-2b), because in some patients no early angiography runs after IAF had been performed (N = 22). Symptomatic intracranial hemorrhage (sICH) was defined as any intracranial hemorrhage on follow-up imaging and an increase in the National Institute of Health Stroke Severity Scale (NIHSS) score of ≥4 according to the European Cooperative Acute Stroke StudyII criteria. 18
Statistical analysis
Data are presented as median (interquartile range (IQR)) or % (n/N). Frequency comparisons were performed using Fisher’s exact test. Non-normally distributed continuous or ordinally scaled variables were compared using Whitney–Mann U-test. For assessing associations between baseline variables and occurrence of early angiographic improvement, a multivariable logistic regression model was built, including age, sex, site of occlusion, and center together with all variables with p < 0.20 in univariable comparison. Clinical regression models were generally adjusted for age, sex, admission NIHSS, Alberta Stroke Program Early Computed Tomography Score (ASPECTS), symptom onset to reperfusion, and occlusion site, according to clinical importance. For assessing the heterogeneity of the clinical effect of EARI on the rate of functional independence, logistic regressions were ran in subgroups and interaction terms were calculated in the complete cohort. The following subgroups were predefined: Symptom onset to administration of IAF ≤4.5 h versus >4.5 h, patients with no or minimal early ischemic signs (ASPECTS 8–10) versus patients with moderate to severe early ischemic changes (ASPECTS <8), and patients with versus without pre-interventional intravenous (IV) alteplase and patients ≥70 years of age versus <70 years of age. Interaction terms were calculated as the variable EARI multiplied with the respective subgroup assigned to the value 1. Results are displayed as adjusted odds ratio (aOR) and corresponding 95% confidence intervals (95% CIs). Patients with missing follow-up were excluded from the analysis regarding functional outcome. No imputation methods were performed. Statistical analyses were carried out in SPSS (SPSS Statistics version 25, IBM, Armonk, NY, USA) and STATA (Stata, version 15.1; StataCorp, College Station, Texas 77845 USA).
Results
After exclusion of patients without available angiographic control runs after administration of IAF (N = 22), 228 patients met the studies’ inclusion criteria for this subanalysis (median age 75, 43.9% female). Patients presented with severe symptoms (median NIHSS 14) and received IAF at a median delay of 225 min (IQR 206–313 min) after symptom onset. Angiographic reperfusion improvement occurred in 116/228 patients after a median dose of 10 mg tissue plasminogen activator (tPA) (IQR 5–10 mg) or 250 000 IU urokinase (IQR 250,000–500,000) had been applied. Rate of sICH was 8.4% (21/255).
Patients who showed early angiographic improvement more often had a cardioembolic stroke origin (51.7 vs. 42.0%, p = 0.013, Table 1). Among patients with early angiographic improvement, the relative frequency of urokinase was higher (41.4% vs. 30.4%) and the rate of preceding IV tPA tended to be higher. On logistic regression analysis, a cardioembolic stroke origin (aOR 3.72, 95% CI 1.39–10.0) and shorter groin puncture to IAF intervals (aOR 0.82, 95% CI 0.71–0.95 per 15-min delay) were the only factors independently associated with EARI. Neither IV tPA (aOR 1.15, 95% CI 0.59–2.26) nor the type of fibrinolytic (urokinase vs. alteplase aOR 0.41, 95% CI 0.04–3.76) were associated with the occurrence of EARI (see Table 2 for full model details). In the subcohort under study, the rate of sICH did not differ between patients pretreated with IV tPA and those not receiving IV tPA (9.6% vs. 7.0%, p = 0.63).
Baseline characteristics with strata of patients with and without EARI.

NIHSS: National Institute of Health Stroke Severity Scale; IA: intra-arterial; iICA: intracranial internal carotid artery; carotid-T: T-type internal carotid artery occlusion; M1: first segment of the middle cerebral artery; M2: second segment of the middle cerebral artery; ASPECTS: Alberta Stroke Program Early Computed Tomography Score; IV: intravenous; EARI: early angiographic reperfusion improvement; sICH: symptomatic intracranial hemorrhage.
Results of the logistic regression model regarding association of baseline characteristics with the occurrence of EARI.
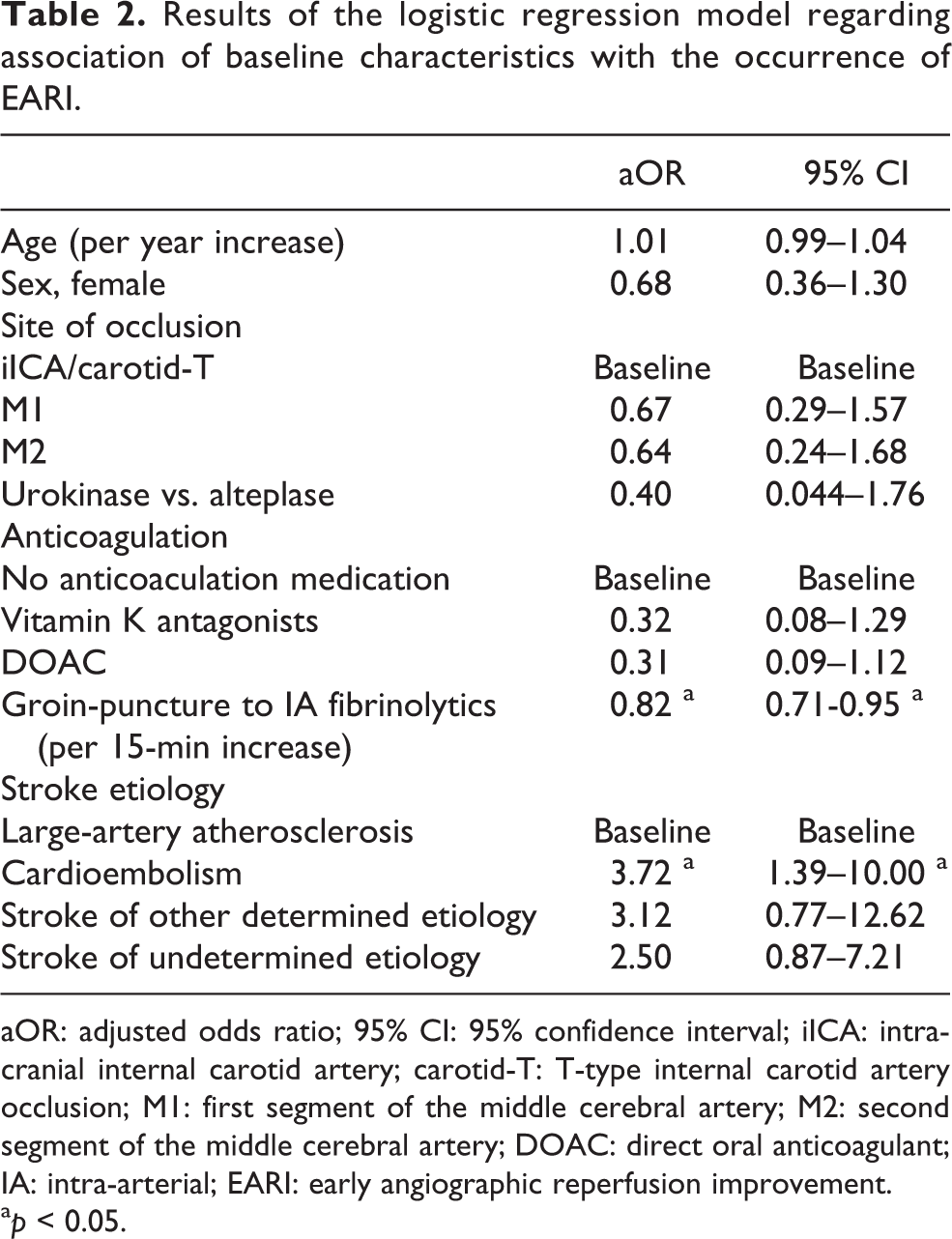
aOR: adjusted odds ratio; 95% CI: 95% confidence interval; iICA: intracranial internal carotid artery; carotid-T: T-type internal carotid artery occlusion; M1: first segment of the middle cerebral artery; M2: second segment of the middle cerebral artery; DOAC: direct oral anticoagulant; IA: intra-arterial; EARI: early angiographic reperfusion improvement.
a p < 0.05.
EARI was associated with higher rates of functional independence after adjustment for confounders (aOR 2.38, 95% CI 1.16–4.89). Point estimates suggested a decreased clinical effect in patients presenting with moderate to severe ischemic changes (ASPECTS ≤8, aOR 0.94, 95% CI 0.27–3.27) as opposed to patient without or minimal ischemic changes (ASPECTS ≥9, aOR 4.00, 95% CI 1.37–11.61, p for interaction: 0.095, Figure 1). There was no similar trend in the subgroups of receiving IAF before and after 4.5 h (aOR 2.76, 95% CI 1.00–7.61 and aOR 1.98, 95% CI 0.58–6.74 for symptom onset to IA ≤270 and >270 min, respectively, p for interaction 0.58). Also, among age subgroups and across strata of pretreatment with IV tPA, no relevant heterogeneity of the association between EARI and rates of functional independence was observed (see Figure 1).

Association of early angiographic improvement and functional independence in subgroups.
Discussion
This study has the following main findings: (1) Early administration of IAF and a cardioembolic stroke origin were associated with higher rates of early angiographic reperfusion after IAF when applied as rescue following MT. (2) Subgroup analysis suggested that the clinical benefit of EARI may be increased in patients presenting without or only minimal early ischemic changes, while being absent or diminished in those with moderate to severe early ischemic changes.
Recanalization rates after MT 19,20 and IV thrombolysis 21,22 have been shown to be time-dependent with decreasing recanalization rates with elapsed time from admission to treatment or symptom onset to treatment. In the current study, EARI after IAF as rescue for MT occurred less often in patients with longer groin-puncture to IAF intervals. A potential causal nature of this association is to be questioned as later rescues with IAF may also correspond to more mechanical maneuvers performed before IAF rescue was considered and hence may constitute a population group of more resistant thrombi in general.
There is conflicting data on the recanalization rates of IV thrombolysis across different stroke etiologies. 23 Within this study, we found that patients with a cardioembolic stroke origin showed higher responsiveness to rescue IAF after MT, with higher rates of EARI observed in these patients. Cardiac thrombi are considered fibrin/platelet dominant clots, making it a potentially better target for the therapeutic effects of fibrinolytics. 24 A comparison of IV thrombolysis to the setting of rescue IAF is, however, limited by the fact that dislodged thrombus fragments or new in situ thrombosis before or behind the initial clot may change thrombus characteristics and respective histology of the residual thrombi after MT. Further research should elucidate if pre-interventional imaging findings are associated with responsiveness to IAF, which can be used for more refined patient selection.
If one attempts to improve, for example, a TICI 2b reperfusion to TICI 2c/3 many unknowns surround the decision-making process and there is paucity of evidence helping to decide in which patients more aggressive treatment escalation is needed and in which patient unnecessary risk are being taken. 25 Improving a TICI 2b to a TICI 2c/3 reperfusion inherently comes with interventional risk or possible excess risk of sICH in the case of IAF. 26 While the earlier a good reperfusion status is achieved, the better the clinical outcomes 27 ; recent evidence suggests that reperfusion status is also important beyond the first maneuvers. 28,29 Hence, also delayed reperfusion improvements may be clinical important. 28,29 On the other hand, recent analyses from the RESCUE-Japan 2 Registry suggested that mTICI 3 versus mTICI 2b was associated with favorable outcomes only when puncture to reperfusion time was <80 min. 30 In this analysis, the association of EARI with higher rates of functional independence was relatively homogenous across subgroups (including different time intervals from symptom onset to IAF) with one exception. Although not significant on interaction analyses, there was a tendency of the association being attenuated in patients with moderate to severe ischemia as opposed to those without or only minor ischemic changes on admission. Likely, the relative benefits of more complete reperfusion are decreased in patients with already established infarcts, because reperfusion improvements in target territories where the infarct has already occurred do not translate into clinical benefits.
The currently running CHemical OptImization of Cerebral Embolectomy trial will randomize patients with incomplete reperfusion after MT to receive either a 30-min IA infusion of weight-adapted tPA or IA placebo. 31 Maximal delay to rescue IAF will be 24 h after symptom onset and patients will be included if admission ASPECTS ≥6 and presentation is <4.5 h or ASPECTS ≥6 on DWI MRI or CT perfusion and if presentation is later than 4.5 h. 31 Post hoc analyses of this trial may shed further light onto a possible reduction of the benefits of IAF in patients with prolonged groin-puncture to rescue intervals or patients presenting with already established moderate to severe early ischemic signs. Until then, the extend of early ischemic changes may be taken into consideration when evaluating if patients should receive rescue IAF after failed or incomplete MT.
Lastly, the registry included only patients with residual distal occlusions after MT, but distal occlusions may also be encountered as primary or secondary occlusions after spontaneous or lysis-induced clot migration. 32 –37 The potential role of IAF in these scenarios cannot be deduced from the presented data, because these thrombi may represent with distinct histopathological and/or mechanical features. 38,39
Limitations
This is a retrospective single-arm observational study with its associated limitations. First, this is a descriptive study without a control group not allowing for an estimation of a potential effect size of added IAF. Second, angiographic efficacy analyses were performed by a neuroradiologists at each center and were not core-lab adjudicated. Third, angiographic control runs after IAF were not timed homogenously across participating centers; neither was the technical approach or choice and dose of the thrombolytic drug standardized. While we have included center as a covariate in our logistic regression models potentially mitigating some of this heterogeneity, presumably this cannot entirely account for differences across centers. Moreover interoperator variability may further add uncertainty, as the exact time point of the angiographic control run after IA tPA administration was not recorded in the registry. The explorative analysis regarding the homogeneity of the association of early angiographic improvement and clinical outcomes was not powered to detect significant heterogeneity between subgroups and CIs in subgroups were wide.
Conclusions
Early rescue and a cardioembolic stroke origin were associated with higher chances of EARI after IAF. The clinical effect of EARI on functional independence was generally homogenous but seemed reduced in patients with already established infarcts. If confirmed, these findings can help to inform patient selection and inclusion criteria for upcoming randomized-controlled trials evaluating IAF as rescue after failed or incomplete MT.
Supplemental material
Supplemental Material, sj-docx-1-ctn-10.1177_2514183X211017363 - Factors associated with early reperfusion improvement after intra-arterial fibrinolytics as rescue for mechanical thrombectomy
Supplemental Material, sj-docx-1-ctn-10.1177_2514183X211017363 for Factors associated with early reperfusion improvement after intra-arterial fibrinolytics as rescue for mechanical thrombectomy by Johannes Kaesmacher, Giovanni Peschi, Nuran Abdullayev, Basel Maamari, Tomas Dobrocky, Jan Vynckier, Eike Piechowiak, Raoul Pop, Daniel Behme, Peter B Sporns, Hanna Styczen, Pekka Virtanen, Lukas Meyer, Thomas R Meinel, Daniel Cantré, Christoph Kabbasch, Volker Maus, Johanna Pekkola, Sebastian Fischer, Anca Hasiu, Alexander Schwarz, Moritz Wildgruber, David J Seiffge, Sönke Langner, Nicolas Martinez-Majander, Alexander Radbruch, Marc Schlamann, Dan Mihoc, Rémy Beaujeux, Daniel Strbian, Jens Fiehler, Pasquale Mordasini, Jan Gralla and Urs Fischer in Clinical and Translational Neuroscience
Footnotes
Author contributions
JG and UF are contributed equally to this work. All authors made substantial contributions to conception and design, and/or acquisition of data, and/or analysis and interpretation of data and participated in drafting the article or revising it critically for important intellectual content.
Availability of data and materials
Data presented in this article are available from the corresponding author upon reasonable request and after clearance by the coinvestigators and their local ethics committees.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the local ethics committees of the included centers.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Schweizerische Hirnschlag Gesellschaft, SAMW.
Informed consent
Written informed consent was obtained from all subjects before the study or written informed consent was obtained from legally authorized representatives before the study, depending on institutional and national guideline and time point of patient inclusion.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.