
Abstract
Introduction:
Combined intravenous thrombolysis (IVT) and mechanical thrombectomy (MT) are the recommended treatment options for acute ischemic stroke (AIS). It is unclear whether earlier IVT and MT management can predict complete vessel recanalization.
Methods:
In this single-center retrospective observational study, we included 81 consecutive subjects with proximal middle cerebral artery AIS (age 70.5 ± 14.2 years, 53% female) who had both IVT and MT. We assessed recanalization after mechanical procedure according to modified thrombolysis in cerebral infarction (TICI) score as well as the National Institute of Health Stroke Scale (NIHSS) score at 24 h. Outcomes were modified Rankin Scale (mRS) at discharge, mRS at 3 months, death at 3 months, and prevalence of intracerebral hemorrhage during hospitalization.
Results:
Multinomial logistic regression (χ 2 = 49.4, p = 0.0075, pseudo-R 2 = 0.26) showed that complete recanalization (TICI score = 3) was predicted by lower door-to-MT time (p = 0.014, 95% confidence interval (CI) = −0.09 to −0.01) and lower symptoms-to-IVT time (p = 0.045, 95% CI = −0.038 to −0.0004). An NIHSS score ≥10 at 24 h was predicted by higher baseline NIHSS (p < 0.0001) and lower TICI score (p = 0.009). Lower NIHSS at 24 h predicted a good outcome according to mRS at 3 months (p = 0.006). Similarly, higher NIHSS at 24 h was a predictor of death at 3 months (p = 0.013).
Conclusions:
The present study suggests that bridging therapy may improve vascular recanalization when both IVT and MT are performed earlier.
Introduction
Stroke is a leading cause of death and disability. 1 –3 Intravenous thrombolysis (IVT) with recombinant tissue plasminogen activator (rt-PA) is the only approved medical therapy for acute ischemic stroke (AIS), 4,5 and most patients benefit from its administration until 4.5 h after symptom onset. 6 Unfortunately, only a small proportion of patients (10–15%) with AIS are eligible for IVT. 7 As clinical outcome is better when thrombolysis is administered earlier, 8,9 current strategies have included informing the population of seeking medical care urgently in the case of acute neurological impairment 10,11 and creating dedicated stroke units. 12,13
Cerebral imaging has permitted to better delineate patients with AIS who would benefit from IVT. This was considered safe and efficient for patients with AIS within 3 h, considering there was no intracerebral hemorrhage (ICH) on non-enhanced computed tomography (NECT). Since this seminal study in 1995, 14 evaluation of early signs of ischemic stroke was improved, thanks to angiographic sequences, 15 perfusion CT sequences, 16 and the widened use of brain magnetic resonance imaging (MRI). 17,18 Although these modalities are increasingly available in the emergency setting, brain NECT is sufficient to rule out contraindications for thrombolysis, 19,20 which, according to the American Heart Association (AHA) recommendations, should be debuted within 25 min of patient’s arrival in the emergency department. 21
Combining IVT and mechanical thrombectomy (MT) is the recommended treatment option for patients with large-vessel occlusion AIS according to class I level A evidence. 22 –24 However, bridging therapy has been a subject of debate in recent years. In fact, results from a post hoc pooled analysis of the STAR 25 and SWIFT 26 studies have shown no clinical benefit of combining IVT and MT over MT alone regarding vascular recanalization as well as mortality and low (i.e. 0–2) modified Rankin Scale (mRS) at 3 months. 27 However, IVT has been shown as a predictor of good clinical outcome in a retrospective study. 28 In addition, a single-center prospective study suggests that bridging therapy seems to confer a beneficial effect on long-term outcome (favorable mRS = 0–2 at 90 days and 1 year). 29
In the present work, we designed a single-center retrospective observational study to assess whether an earlier IVT and MT management (door-to- and symptoms-to-IVT/MT time) was a predictor of complete vascular recanalization after MT in a single-center consecutive AIS with proximal middle cerebral artery (MCA) occlusion. We also assessed which parameters predicted a better clinical outcome (mRS and death at 3 months).
Materials and methods
Patients
The study took place in Geneva University Hospitals, Geneva, Switzerland. We retrospectively collected clinical data from all subjects with proximal MCA occlusion AIS from July 3, 2012 to January 17, 2017 and benefiting from combined rt-PA IVT and MT. From July 2012 to October 2013, participants received rt-PA injection after the complete brain CT scan (including angiographic sequences). From October 2013, we implemented an earlier IVT directly after NECT, as the patient was still lying in the CT table. All included patients later had brain MRI which confirmed the presence of AIS.
Thrombolysis inclusion criteria
Eligibility criteria for IVT are as follows: any patient aged 18- to 80-year-old with suspected stroke onset of less than 4.5 h and National Institute of Health Stroke Scale (NIHSS) score ≥5 (or lower in the case of severe aphasia), or greater than 80-year-old with an NIHSS score ≥8. As part of the general AIS management, patients were informed orally about the procedure by a physician working in the emergency department. In case the patient was not capable of giving an answer (e.g. because of aphasia), the procedure was explained to a member of the family, if present.
After reviewing the images with the emergency radiologist, clinical and radiological exclusion criteria according to ECASS-III 6 and 2007 AHA Guidelines 30 were assessed, including the absence of ICH and of an hypodensity larger than one-third of the MCA area. Early rt-PA IVT bolus was prepared (10% of the 0.9 mg/kg of weight total dose, maximal 9 mg) by the neurology resident and administered to the patient, as he was still lying on the CT table. Brain CT acquisition was then resumed, including angiographic and perfusion sequences. Thereafter, the patient was carried back to his emergency box, and the remaining dose of IVT was administered (90% of 0.9 mg/kg during 60 min). For subjects included from July 2012 to September 2013, the whole rt-PA IVT was administered after the whole CT sequences (NECT and perfusion sequences) were performed.
As a retrospective observational analysis of clinical data, our local ethics committee waived the need for consent from subjects (reuse of biological data, protocol CCER 2016-0910). The study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
The following clinical data were collected: symptoms-to-IVT, symptoms-to-MT, door-to-imaging time, door-to-IVT, and door-to-MT time. Door-to-IVT time was considered as the time from the admission in the emergency department to the first administration of IVT bolus. We also assessed NIHSS score at admission, NIHSS score at 24 h, modified Rankin score (mRS) at discharge from the Neurology Department, and mRS at 3 months from stroke onset. Prevalence of any ICH and death at 3 months were also assessed. Baseline characteristics included age, male/female ratio, initial NIHSS, and site of occlusion (internal carotid artery, M1 or M2 portion of the MCA). All cases were MRI-confirmed AIS.
Short-term outcomes were thrombolysis in cerebral infarction (TICI) score after mechanical procedure and NIHSS score at 24 h. Other outcomes included mRS at discharge, mRS at 3 months, death at 3 months, and prevalence of any ICH during hospitalization.
Statistical analysis
Stata 14.2. (College Station, Texas, USA) software was used for statistical analysis. Distributions of the continuous variables were assessed for normality with Shapiro–Wilk test. Regression analysis with the determination of the variance inflation factor (VIF) was performed to assess whether independent variables showed multicollinearity (redundancy) and variables with VIF > 10 were removed from the analysis. 31 Dependent variables were converted as categorical variables, so we performed multinomial logistic regression analysis using clinical outcomes as independent variables. For short-term outcomes (TICI score after recanalization procedure), we assessed predicting parameters among the following independent variables: age, gender, NIHSS score at stroke presentation, symptoms-to-IVT time, symptoms-to-MT time, door-to-IVT time, door-to-imaging time, and door-to-MT time. NIHSS score at 24 h was dichotomized as <10 and ≥10, and we used the same independent variables as earlier and added TICI score after MT. For other outcomes (mRS at discharge and at 3 months, death at 3 months, and any ICH during hospitalization), we used the same independent variables and added NIHSS score at 24 h. We hypothesized that a shorter time between symptoms onset and IVT/MT would correlate with a better recanalization according to TICI score. In addition, we expected a better 3-month outcome (mRS score) for patients with shorter time between symptoms onset and IVT/MT procedure.
Values are usually mentioned as mean ± standard deviation (range). The values of p < 0.05 were considered as statistically significant.
Results
Eighty-one subjects were included in the present observational study. Table 1 presents the baseline characteristics of patients. Stroke syndrome according to Bamford classification was mainly partial anterior circulation stroke (49.4%, 40 of 81) and total anterior circulation stroke (40.7%, 33 of 81). Lacunar syndrome was present in 8 of 81 (9.9%) patients. Etiology of stroke according to Trial of Org 10172 Acute Stroke Treatment classification 32 was cardiac embolization (56.8%, 46 of 81), large artery atherosclerosis (19.8%, 16 of 81), cervical artery dissection (6.2%, 5 of 81), other determined causes (11.1%, 9 of 81), or unknown despite complete evaluation (6.2%, 5 of 81). Previous ischemic stroke and transient ischemic attack was experienced by 6 of 81 (7.4%) and 2 of 81 (2.5%) subjects, respectively. Cardiovascular risk factors included hypertension (65.4%, 53 of 81), diabetes (16%, 13 of 81), dyslipidemia (19.8%, 16 of 81), tobacco smoking (14.8%, 12 of 81), and atrial fibrillation (13.6%, 11 of 81).
Baseline characteristics of included subjects.a

NIHSS: National Institute of Health Stroke Scale; IVT: intravenous thrombolysis; MT: mechanical thrombectomy.
aTime values are expressed in minutes. Results are mean ± SD (range).
Device used for MT was mainly Stent Retriever (65.4%, 53 of 81), the other devices being Solitaire (13.6%, 11 of 81) and Penumbra (2.5%, 2 of 81). Aspiration only was performed for 15 cases (18.5%).
Outcomes of subjects (TICI score after MT, NIHSS at 24 h, mRS at discharge and at 3 months, prevalence of ICH, and death at 3 months) are available in Table 2.
Summary of outcomes.a

TICI: thrombolysis in cerebral infarction; MT: mechanical thrombectomy; NIHSS: National Institute of Health Stroke Scale; ICH: intracerebral hemorrhage.
aTime values are expressed in minutes. Results are mean ± SD (range).
Among the independent variables, symptoms-to-MT time showed multicollinearity as its VIF was high (71.1). It has therefore been removed from further analyses.
Regarding TICI score, multinomial logistic regression (χ 2 = 49.4, p = 0.0075, pseudo-R 2 = 0.26) showed that complete recanalization (TICI score = 3) was predicted by lower door-to-MT time (p = 0.014, 95% confidence interval (CI) = −0.09 to −0.01) and lower symptoms-to-IVT time (p = 0.045, 95% CI = −0.038 to −0.0004). Successful recanalization, however, was not predicted by age (p = 0.75), gender (p = 0.73), initial NIHSS score (p = 0.42), door-to-imaging time (p = 0.79), or door-to-IVT time (p = 0.64). In addition, TICI score was strongly correlated with symptoms-to-IVT time (Spearman rank correlation ρ = −0.26, p = 0.01; Figure 1) and door-to-MT (ρ = −0.38, p = 0.0007; Figure 2).

Spearman rank-order correlation coefficient showing a negative correlation between TICI score and symptom-to-IVT time (p = 0.01, ρ = −0.27). TICI: thrombolysis in cerebral infarction; IVT: intravenous thrombolysis.
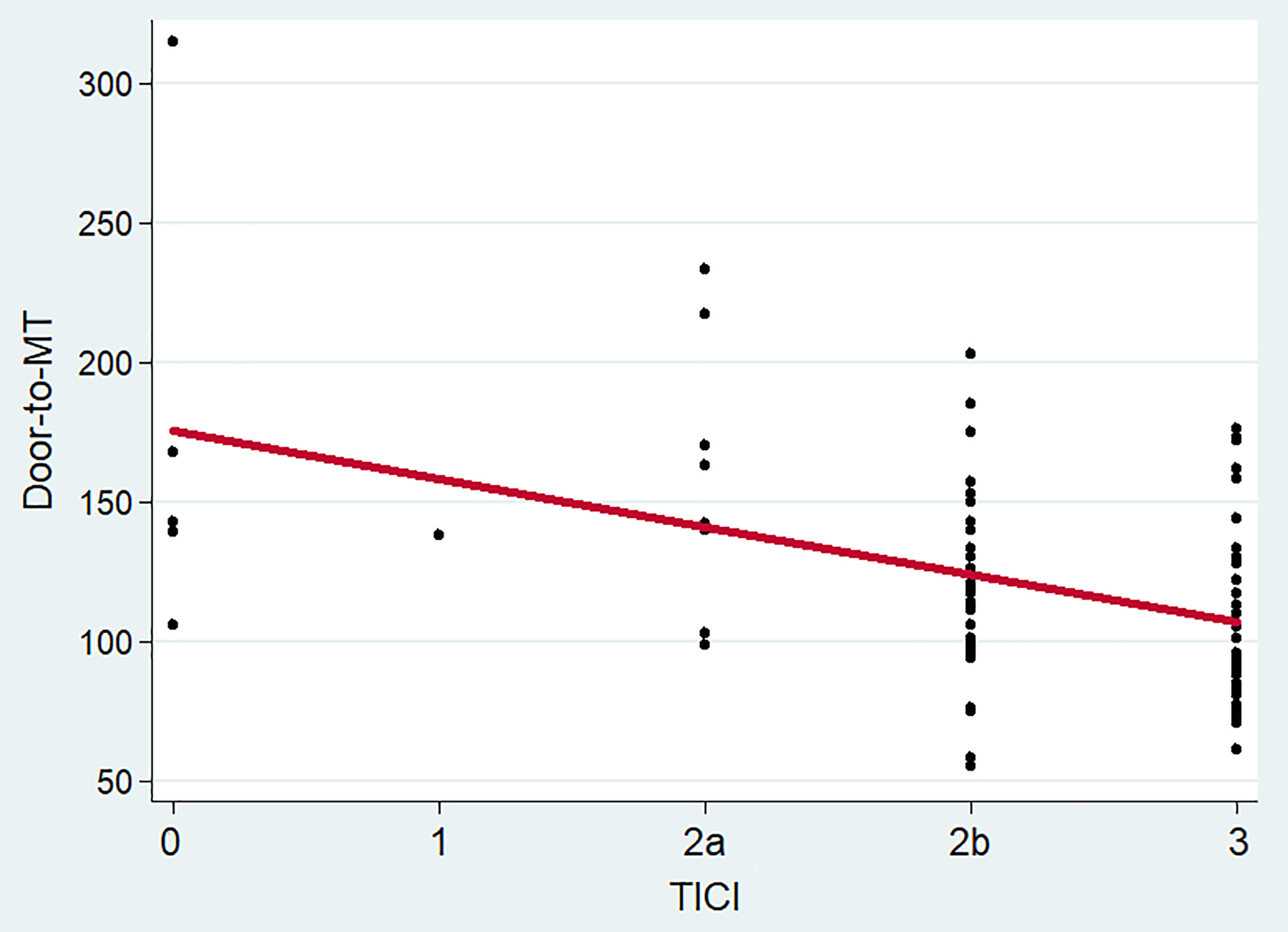
Spearman rank-order correlation coefficient showing a negative correlation between TICI score and door-to-MT time (p = 0.0007, ρ = −0.38). TICI: thrombolysis in cerebral infarction; MT: mechanical thrombectomy.
An NIHSS score ≥10 at 24 h (χ 2 = 41.5, p < 0.0001, pseudo-R 2 = 0.41) was predicted by higher baseline NIHSS (p < 0.0001, 95% CI = 0.165 to 0.496) and lower TICI score (p = 0.009, 95% CI −1.98 to −0.279).
Regarding mRS at discharge (χ 2 = 141.6, p < 0.0001, pseudo-R 2 = 0.496), younger age (p = 0.018, 95% CI = −0.23 to −0.021), and lower NIHSS at 24 h (p = 0.009, 95% CI = −1.15 to −0.16) were significant predictors for a complete clinical recovery (mRS = 0). For mRS at 3 months (χ 2 = 108.1, p < 0.0001, pseudo-R 2 = 0.501), there was a trend for NIHSS at 24 h (p = 0.17). When dichotomizing mRS score as good outcome (mRS = 0–2) and poor outcome (mRS = 3–6; χ 2 = 34.6, p = 0.0001, pseudo-R 2 = 0.42), lower NIHSS at 24 h (p = 0.006, 95% CI = −0.416 to −0.068) and lower age (p = 0.044, 95% CI = −0.11 to −0.0014) were found as significant predictors of good outcome for mRS at 3 months. Older age (p = 0.047, 95% CI = 0.001 to 0.179) and higher NIHSS at 24 h (p = 0.013, 95% CI = 0.054 to 0.47) were also significant predictors of death at 3 months. Higher NIHSS at 24 h was also a significant predictor for ICH (p = 0.029, 95% CI = 0.015 to 0.281).
Discussion
In the present single-center retrospective observational study, we showed that both IVT and MT proxy (symptoms-to-IVT and door-to-MT) were significant predictors of a complete recanalization (TICI score = 3) in proximal MCA AIS. These findings are contrasting with recent studies showing the benefit of IVT prior to MT only for distal occlusions. 33 This is also in contradiction with recent reports arguing that IVT does not influence vascular recanalization. 34,35
Secondly, we have been able to demonstrate that complete recovery (i.e. mRS at discharge = 0) was predicted by younger age and lower NIHSS at 24 h. Regarding other outcomes, we observed that lower NIHSS at 24 h predicted a good outcome according to mRS at 3 months, lower death prevalence at 3 months, and lower prevalence of ICH.
This original finding shows that irrespective of the severity of stroke, an early IVT is crucial before considering MT and that synergistic treatment definitely has its place in patients with AIS.
Recent major trials have shown that MT in large-vessel anterior occlusion led to a significant reduction of 3-month disability when combined with best medical treatment, including subgroups of older patients (>80 years old), those with MT performed after 5 h from symptom onset or those not eligible for IVT. 24 Based on class I level A evidence, bridging therapy with IVT and Stent Retriever MT is the recommended treatment for patients with large-vessel occlusion AIS. 22–24 Combining IVT and MT is based on the following observations: There is evidence that early recanalization directly after IVT is observed in up to 21% of subjects with M1 occlusion and up to 38% for M2 occlusions, 36 although pooled analyses of the major trials regarding MT do show lower rates (7–14%). 26,37,38 Second, we can postulate that IVT may promote clot softening and an easier thrombus extraction during MT. These observations are mainly derived from retrospective single-center cohort studies, and pooled data from MT pivotal trials have not confirmed this assumption. 27 Lastly, IVT may improve collateral microcirculation 39 and help reperfusion of distal arteries that are not accessible to MT devices, 40 thereby improving TICI score and 3-month outcome. In fact, it has been repeatedly shown that earlier IVT is associated with a better clinical and radiological outcome. 41 –44 However, as only proximal MCA AIS has been included in the present study, this specific hypothesis cannot be taken into account.
Limitations of the study include its retrospective design as well as the relatively small sample size, so our encouraging results need to be confirmed in a multicentric study. In addition, door-to-IVT and door-to-MT time are slightly higher than in many stroke centers. Since we implemented a fast-track management of AIS in October 2013 (with IVT started in the scanner), door-to-IVT was reduced from a mean time of 58 min to 44 min. A similar reduction for door-to-MT time was observed.
Conclusion
Both earlier IVT (according to symptoms-to-IVT time) and MT (door-to-MT time) are positive predictors of a complete vascular recanalization according to the modified TICI score. IVT before MT in eligible patients presenting with proximal MCA AIS should be pursued according to the international recommendations for the management of AIS. Multicenter randomized controlled trials are therefore warranted to confirm the superiority of MT alone compared to bridging therapy.
Footnotes
Acknowledgements
The authors would like to thank all the neurology residents for their thoroughness in documenting the patient’s thrombolysis data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.