
Abstract
Background:
Naviculectomy was originally described for resistant congenital vertical talus deformity but was later expanded to use in rigid cavus deformity. This study reviews the operative outcomes of complete excision of the navicular for recurrent deformity in the talipes equinovarus (TEV) population.
Methods:
After institutional review board approval, all patients undergoing naviculectomy at a single institution were identified. Clinical, radiographic, and pedobarographic data (minimum 2 years’ follow-up) were reviewed.
Results:
Twelve patients (14 feet) with TEV from 1984 to 2019 were included. All feet had minimum 1 prior operative intervention on the affected foot (mean age = 4.0 years, range 0.2-14.5), with 8/14 having at least 3 prior operative procedures. Complete navicular excision with concomitant procedures was performed in all patients (mean age = 11.7 years, range 5.5-16.1). Mean clinical follow-up from naviculectomy was 5.1 years (range, 2.2-11.2). During follow-up, 6 patients required subsequent surgery, most often secondary to pain and progressive deformity. One patient underwent elective below-knee amputation of the affected extremity. Of the remaining 11 patients, 7 of 11 reported continued pain and 8 of 11 maintained adequate range of motion at the ankle at the most recent follow-up.
Conclusion:
Clinical follow-up demonstrated deteriorating results in a large percentage of patients. The high rate of additional procedures and continued pain in the current series suggests that even as a salvage procedure, naviculectomy may not provide adequate results for patients.
Level of Evidence:
Level IV, case series.
Introduction
Talipes equinovarus (TEV), or clubfoot, is a complex 3-dimensional foot deformity occurring in approximately 1 out of 1000 births. The current standard for treatment of clubfoot deformity is the Ponseti technique, which includes serial casting, heel cord tenotomy, and abduction bracing to reduce recurrence risk. 13,15 Prior to the acceptance of the Ponseti technique, clubfoot deformity was managed with early soft tissue release, often complicated by cases of undercorrection, overcorrection, need for revision surgery, and poor long-term outcomes. 6,8,11,17 Feet requiring multiple surgeries often present with persistent deformity requiring salvage procedures for correction including osteotomy or arthrodesis. The results of salvage strategies, such as triple arthrodesis, can often be problematic, with poor long-term outcomes including pain, arthritis, and poor foot function. 1,7,17
Historically, combined medial and lateral column procedures were often employed to correct resistant foot deformities secondary to TEV or congenital vertical talus. 7,9 Naviculectomy was originally described as a salvage procedure primarily for cases of resistant congenital vertical talus deformity. 2,3 Mubarak and Dimeglio expanded the use of this procedure in children with rigid cavus deformity. 14 At our center, we have employed the use of naviculectomy for correction of the recurrent or recalcitrant equino-cavovarus deformities associated with clubfoot in order to provide adequate medial column shortening and restoration of a plantigrade position of the foot. In this review, we report the results of complete excision of the navicular for recurrent deformity in the clubfoot population.
Materials and Methods
After obtaining institutional review board approval, we performed a retrospective review of all patients who had naviculectomy performed at our institution. Patients with an operative history of naviculectomy and a minimum of 2 years follow-up were identified through the medical record database. Patients with concomitant talectomy or nonidiopathic TEV were excluded from the study.
From the medical record, clinical data points included prior treatment methods of the TEV deformity, age at surgery, procedures performed concomitantly with naviculectomy, need for additional operative treatment after naviculectomy, and patient-reported clinical outcomes.
Standing anteroposterior (AP) and lateral radiographs of the foot and ankle obtained before operative intervention and at the most recent follow-up visit were compared. Radiographic data points included the AP talo–first metatarsal angle, tibiotalar angle, lateral calcaneal pitch angle, lateral tibiocalcaneal angle, lateral talo–first metatarsal angle, and lateral talocalcaneal angle. An orthopedic resident, senior research assistant, and lead author independently performed measurements for all radiographs to determine interrater reliability.
Foot pressure analyses using pedobarographic data to evaluate foot loading patterns were obtained pre- and postoperatively. The relative movement of the center of pressure during stance phase is represented by the center of pressure progression in defined regions (hindfoot, midfoot, and forefoot) and partitions (medial and lateral) of the foot. Changes in the fore-aft and medial-lateral position of the center of pressure progression were used to evaluate perioperative change. 10
Statistical Methods
The average interrater reliability of radiographic measurements was determined by calculating the intraclass correlation coefficient (ICC) as described by Shrout and Fleiss. 16 The pre- and postoperative radiographs of 13 extremities were available for review and were measured by the resident, lead author, and a senior research assistant to evaluate interrater reliability. Results were interpreted based on the scale suggested by Koo and Li where values <0.50 indicate poor reliability, values between 0.50 and 0.75 indicate moderate reliability, values between 0.75 and 0.90 have good reliability, and values >0.90 indicate excellent reliability. 12 The ICC for these measures was 0.98, indicating excellent reliability.
The means and ranges for the age at operative intervention, radiographic measures, and pedobarographic parameters were collected for all subjects. Paired t tests were used to determine significant differences with the numbers available between radiographic and pedobarographic measures preoperatively and at most recent follow-up. Statistical significance was set at P < .05.
Results
From 1984 to 2019, naviculectomy was performed in 20 patients (24 feet) for recurrent clubfoot deformity. Of these, 6 patients (9 feet) had concomitant talectomy with naviculectomy, and 2 patients (2 feet) had an underlying diagnosis of myelodysplasia. These were excluded from the study, leaving 12 patients (14 feet) in the study cohort. Of these 12 patients, 7 were male and 5 were female. All patients had a diagnosis of idiopathic talipes equinovarus (Table 1). Prior to naviculectomy, all feet had at least 1 prior operative intervention on the affected foot (Table 2) at an average age of 2.5 (range, 0.2-8.9) years, with more than half (8/14) of the cohort having had at least 3 prior operative procedures for foot deformity.
Summary of Patient Demographics, General Surgical Data, and Clinical Follow-up.

Surgical Timeline of Cohort.a

Abbreviations: AFO, ankle foot orthosis; CC, calcaneocuboid; LCS, lateral column shortening; LLD, limb-length discrepancy; MM, medial malleolus; MTP, metatarsophalangeal; NC, no complaints; Ost, osteotomy; PMR, posterior medial release; ROM, range of motion; TAL, tendo-Achilles lengthening; TN, talonavicular.
a Operative history before naviculectomy, concomitant procedures at time of naviculectomy, and postnaviculectomy operative treatment are included. Clinical follow-up notes and status of talocuneiform fusion at final radiograph are also listed.
The mean age at naviculectomy was 11.7 (range, 5.5-16.1) years. Complete excision of the navicular was performed. Additional procedures performed at the time of naviculectomy are listed in Table 2. Lateral column shortening, with or without calcaneocuboid arthrodesis, was performed in 11 feet. Additional soft tissue procedures (posteromedial release, anterior tibialis transfer, tendo-Achilles lengthening) were performed in 3 feet. Four feet underwent fusion of the subtalar joint. Mean clinical follow-up from naviculectomy was 5.1 (range, 2.2-11.2) years for the cohort.
During the follow-up period, subsequent operative procedures were required in 6 patients at an average of 3.6 (range, 1.2-11.8) years following naviculectomy. Five of these patients (5/6) underwent a single additional procedure, with 2 additional procedures required in 1 patient (Table 2). Progressive deformity was the most frequent indication for additional surgery and was reported in 3 of the 6 patients requiring operative intervention. Medial column procedures (osteotomy or fusion) were performed in 5 feet. Because of persistent pain, 1 patient underwent below-knee amputation of the affected extremity 1.2 years after naviculectomy.
Radiographic Outcomes
Preoperative and postoperative radiographs were available for 13 feet, including 1 foot that later underwent elective amputation (Table 3). Of these 13 radiographic examinations, plantar wedging of the navicular was present in 9. Two were morphologically normal in appearance, 1 was flattened, and 1 was hypoplastic. Evidence for avascular changes in the navicular was seen in 4 cases. Dorsal subluxation of the navicular occurred in 8 cases, with neutral positioning in 4, and plantar subluxation in 1. Talonavicular joint arthrosis was present in 6 of the 14 feet. Preoperative radiographs demonstrated hindfoot varus (decreased lateral talocalcaneal angle), cavus (increased lateral talo–first metatarsal angle), and forefoot adduction (increased AP talo–first metatarsal angle). 4 Postoperatively, radiographic improvement of the cavus deformity was noted with normalization of the lateral talo–first metatarsal angle. For the hindfoot, there was a significant difference in the measure of the calcaneal pitch postoperatively, indicating mild worsening of the equinus deformity. The remaining radiographic measures did not demonstrate any significant change when comparing pre- to postoperative values.
Pre- and Postoperative Radiographic Data Compared for 13 feet With Available Radiographs.a

Abbreviation: AP, anteroposterior.
a Comparison to a group (n=60) of previously reported norms demonstrates the severe deformity encountered in these feet.4 All measures are in degrees. Bold values indicate statistical significance using paired t tests at P < .05.
b Indicates significant difference from normal values4 at P < .05.
c n for tibiotalar angle was 11 preoperative, 8 postoperative, and 8 for paired t tests.
Fusion of the talus to the cuneiforms occurred in 7 of 13 feet after naviculectomy. Two of these patients required additional medial column procedures (midfoot osteotomy in 1 patient and talocuneiform arthrodesis in 1) during follow-up. Fusion of the talus to the cuneiforms did not occur in 6 feet (Figure 1). Three of these required additional surgery after naviculectomy, including talocuneiform arthrodesis in 1 patient, midfoot osteotomy in 1 patient, and a double arthrodesis in 1 patient (Figure 2).

(A) Preoperative AP and lateral radiographs of a 14.9-year-old male (Table 2, case 3) with residual talipes equinovarus deformity after previous soft tissue release during early childhood. Naviculectomy with talocalcaneal and CC fusion of the right foot is performed. (B) AP and lateral radiographs 1.2 years after naviculectomy. Despite lack of fusion between the talus and cuneiforms, the patient had no complaints of continued pain and require no additional surgery. AP, anteroposterior.
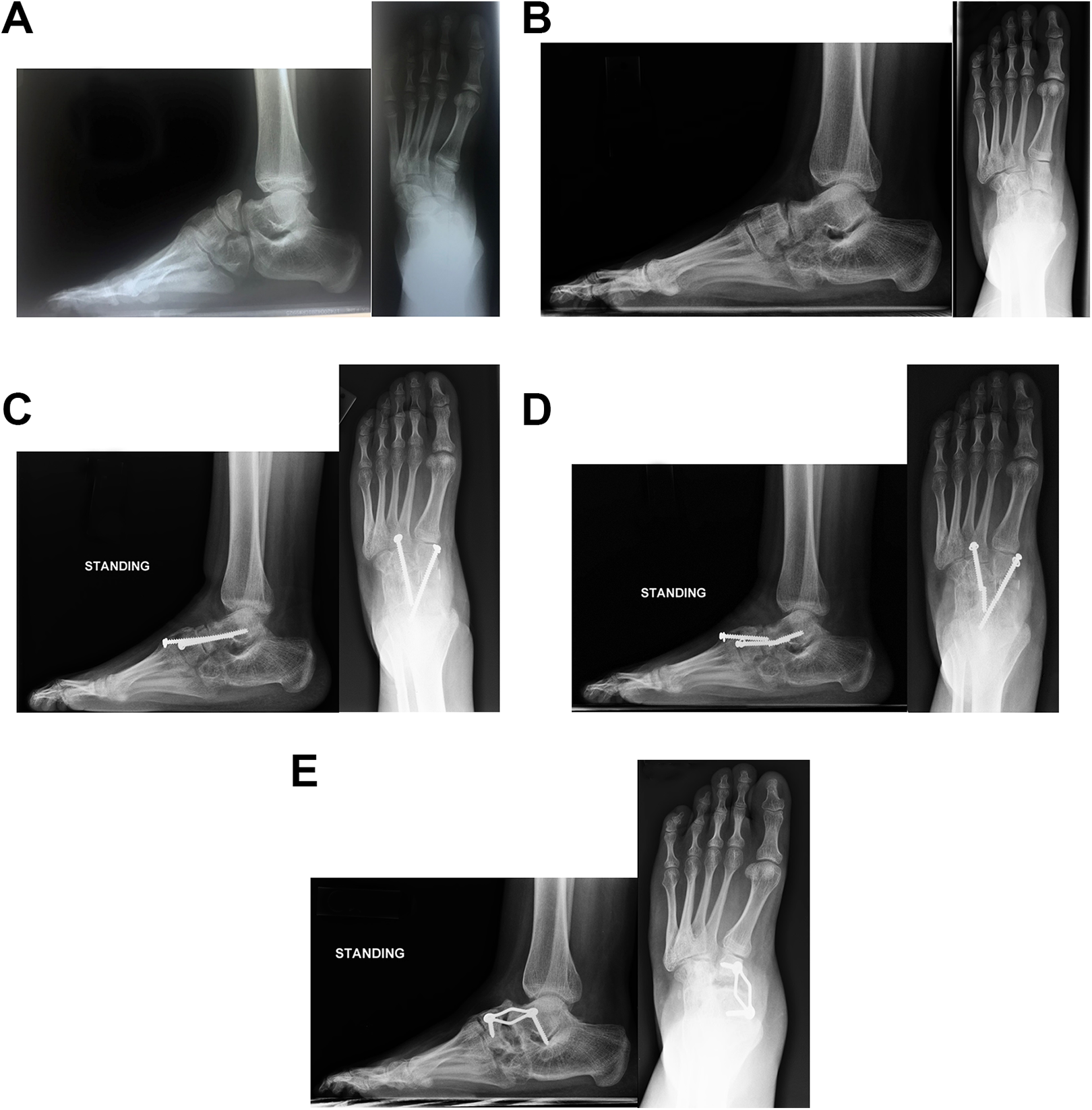
(A) Preoperative AP and lateral radiographs of 13.3-year-old female (Table 2, case 8) with residual talipes equinovarus deformity after previous soft tissue release performed during early childhood. Naviculectomy of the left foot is performed 2.4 months later at 13.5 years of age. (B) AP and lateral radiographs 2.5 years after naviculectomy for recurrent deformity and onset of pain post treatment with 2-stage PMR and serial casting. (C) Owing to increasing midfoot pain, a talocuneiform arthrodesis was performed at age 16.2 years with use of screws and allograft. (D) Nonunion occurred with breakage of screws. (E) Radiographs after revision procedure with use of plate and screw fixation. persistent nonunion is present between the talus and cuneiforms and patient continues to complain of pain and foot/ankle swelling. AP, anteroposterior; PMR, posterior medial release.
Pedobarographic Outcomes
Seven patients (9 feet) had both pre- and postoperative pedobarographic data available for analysis (Table 4). Of the 5 patients not included in the pedobarographic outcomes, 2 patients had postoperative data only, 1 patient had preoperative data only, and 2 patients were treated prior to the implementation of pedobarographic analysis at our hospital.
Pre- and Postoperative Pedobarographic Data for 9 Feet With Available Data.a

a Comparison with a group of previously reported norms (n=46) shows the improper loading pattern with increased forefoot, hindfoot, and lateral pressures preoperatively. 10 Improvement toward central loading in the mediolateral direction is noted postoperatively. Bold values indicate statistical significance using paired t tests at P <.05.
b Significant difference from normal values 10 at P < .05.
Preoperative assessment demonstrated an improper loading pattern with increased midfoot pressure, normal forefoot pressure, and decreased hindfoot pressure. From medial to lateral, increased lateral loading was also noted. 10 Postoperative assessments taken an average 3.8 (range, 1.2-6.8) years from surgery demonstrated significant changes in the fore-aft loading pattern, with a significantly improved and normalized hindfoot loading time, comparable midfoot loading, and significantly decreased forefoot loading. In the mediolateral direction, there was a trend toward improved central loading, with mild residual increased lateral loading of the foot.
Clinical Outcomes
In their final year of follow-up, 7 of 12 patients reported ongoing pain. Of the 11 patients (13 feet) who did not undergo elective amputation, 8 patients (9 feet) were observed to have a range of motion at the ankle that was “acceptable” for the procedures they had undergone. The remaining 3 patients (4 feet) were noted to have restricted ankle range of motion. Three patients continued to wear AFO’s. Of these 3 patients, 1 preferred continuation of their AFO for comfort, 1 had a 1-cm limb length discrepancy resulting from foot deformity and preferred an AFO to a shoe lift, and 1 had a shortened foot resulting from treatment and used the AFO to maintain a toe-filler in place for shoe wear.
Discussion
Naviculectomy is a procedure previously reported as a salvage procedure for congenital vertical talus in which the navicular is dislocated dorsally on the talus. 2,3 In these cases, shortening of the medial column aides in reducing the forefoot to the hindfoot. 3,5 Clark 3 reviewed 16 feet with congenital vertical talus in 12 patients, all managed with complete excision of the navicular. Procedures were performed between ages 5 months and 6½ years. Only 1 patient required a subsequent procedure. Clinical outcomes were better when the procedure was performed before 18 months of age.
In patients with recurrent equinovarus deformity after operative treatment for clubfoot, the medial column is short relative to the lateral column, and often stiff secondary to scarring from previous soft tissue release. Aggressive soft tissue release of the medial column can result in scarring of the talonavicular joint with occasional dorsal subluxation or wedging of the navicular. It may be counterintuitive to recognize the need for medial column shortening in the resistant equinovarus deformity. Rigid cavus deformity typically requires shortening of both the medial and lateral column to achieve a plantigrade position of the foot. The dorsally subluxated or dislocated navicular can present as a mechanical block to reducing and aligning the foot. In these case, combined medial column release with lateral column shortening procedures are utilized to restore the alignment of the foot. 14,18 When medial soft tissue release is inadequate, naviculectomy provides sufficient skeletal shortening of the medial column to allow for restoration of foot alignment.
Naviculectomy has been described in the correction of rigid cavovarus deformity. Mubarak and Dimeglio performed a retrospective review from 2 centers of navicular excision and cuboid closing wedge osteotomy for severe cavovarus foot deformities in 11 patients (16 feet). Patients included those with prior clubfoot correction (5 feet), as well as foot deformity associated with arthrogryposis (6 feet) or deformity associated with neurogenic etiology (5 feet). 14 All of the severe clubfoot patients had fusion of the cuneiforms to the talus at a reported mean age of 9.3 years. In this small series, none of the clubfoot patients required additional surgery, and all reported no pain at their most recent follow-up (mean 4.9 years).
In the current study, we identified 14 feet in 12 patients that had a similar approach to the resistant and rigid cavovarus deformity associated with recurrent clubfoot. All of these feet presented after prior operative management for clubfoot, with 8 of 14 having undergone 3 or more procedures during their treatment course. Concomitant procedures including lateral column shortening procedures and additional soft tissue releases were required in all of these feet. Although a plantigrade foot was achieved initially with this procedure, subsequent follow-up demonstrated deteriorating results in a large percentage of patients. One patient elected to have amputation of the affected limb secondary to chronic pain and residual foot deformity. Additional surgery to correct deformity and pain was required in 6 feet. Seven patients (8 feet) reported continued pain.
The significant difference in radiographic measures from normal values pre- and postoperatively highlights the severe deformity encountered in these feet. An expected improvement in the amount of radiographic cavus deformity was found. Fusion of the talus to the cuneiforms occurred in approximately half of the cohort. Mubarak and Dimeglio 14 suggested the use of temporary pins to secure the position of the foot with an attempt to preserve motion between the talus and the cuneiforms. In our series, pins were used in all cases, with fusion occurring in approximately half of the cases. It is possible that the success of naviculectomy is dependent on successful fusion of the talus to the cuneiforms. Of the 13 feet with postoperative radiographs, fusion occurred in 7. However, 3 of the 7 feet with radiographic evidence of fusion experienced continued pain, and 1 of the remaining 4 underwent elective amputation. We were unable to identify a difference in the clinical or radiographic outcome in feet that fused vs those that did not.
Preoperative pedobarographic analysis of 9 feet showed an improper loading pattern with increased pressure in the forefoot and hindfoot, as well as increased lateral loading of the foot. Reduced loading of the forefoot as well as a trend toward improved central loading in the mediolateral direction was found postoperatively. 10 These findings correspond with the overall change in segmental and radiographic alignment of the foot.
Weaknesses of the current study include the retrospective nature of the study and the small number of cases identified over a 35-year period. Clinical, radiographic, and pedobarographic follow-up data were based on chart review at the most recent visit for all subjects as opposed to formal questionnaires or surveys. Our site did not begin collecting patient-reported outcome data regularly until 2016; therefore, more nuanced patient-reported outcomes were unavailable for review in the cohort. Multiple procedures, in addition to the naviculectomy, were performed in all cases and the outcomes discussed could have been secondary to factors other than the naviculectomy. Additionally, the poor results noted in this patient population may have been related to the known challenges of the multiply-operated foot as opposed to naviculectomy alone. Not all patients were followed until skeletal maturity and it is possible that improvement or worsening of condition could still occur. A larger, multi-center study may provide a more detailed outlook on the long-term results of this procedure as a salvage operation in patients with severe talipes equinovarus.
Conclusion
Naviculectomy is an uncommon salvage procedure that is typically reserved for cases of congenital vertical talus. Few reports have been made on its utility as a salvage procedure for the recalcitrant clubfoot. Although short-term results were positive, the high rate of additional procedures and continued pain in the current series suggests that even as a salvage procedure, naviculectomy does not provide optimal results in these conditions. Patients and their families should be advised of the variable outcomes that are possible if considering this procedure and other treatment options should be explored. Fortunately, with the advent and acceptance of the Ponseti method for clubfoot, the indications for salvage procedures such as naviculectomy in the recalcitrant clubfoot population will be limited.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211008155 - Outcomes of Naviculectomy for Severe Recurrent Clubfoot Deformity
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211008155 for Outcomes of Naviculectomy for Severe Recurrent Clubfoot Deformity by David E. Westberry, Ashley M. Carpenter, Katherine Brown and Samuel B. Hilton in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval for this study was waived by the Western Institutional Review Board (WIRB) (now WCG) because: We believe the study is exempt under 45 CFR § 46.104(d)(4) because the research involves a retrospective evaluation of pre- and postop assessments (including radiographs) of patients with severe, rigid equinovarus who underwent a naviculectomy to examine the functional outcomes of the procedure. The data will be recorded in a deidentified manner. The research is not classified, is not regulated by the FDA, and does not involve prisoners.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.