
Abstract
Abstract
Purpose
Congenital talipes equinovarus (CTEV) has a high incidence in the South Pacific, with New Zealand Maori and Polynesian rates of up to seven per 1000 live births, at least five times higher than the Caucasian population. A genetic component is suggested to explain this, however, there is little information regarding the difference of incidence between Polynesian and Melanesian ethnicity in the South Pacific. Our aim was to investigate the effects of ethnicity on the incidence of CTEV in the Solomon Islands, specifically comparing Melanesian and Polynesian ethnicity.
Methods
Between 2011 and 2017, data was collected in the Solomon Islands from over 40 clinics upon introduction of the Ponseti programme for treatment of CTEV. Records were kept using the validated Global Clubfoot Initiative data form. Ethnicity was documented, including family history.
Results
In total, 138 children presented during this period, with 215 affected feet reviewed and treated. In all, 74% of children had solely Melanesian parents and 6% Polynesian. Using the general population ethnic breakdown of 95.3% Melanesian and 3.1% Polynesian, the odds of CTEV in children of Melanesian parents were 0.41 times lower compared with the odds in children of Polynesian parents.
Conclusion
The results indicate that in the Solomon Islands, CTEV in Melanesian children was less than half as likely to occur in Polynesian children. Our findings also support the theories of minimal Polynesian genetic material persisting in the Solomon Islands and a different genetic risk of CTEV between Polynesians and Melanesians.
Level of Evidence
III
Introduction
Congenital talipes equinovarus (CTEV), also referred to as ‘clubfoot’, is the most common congenital abnormality affecting the foot, with approximately one in 1000 live births affected in the Caucasian population. 1 The incidence is known to be much higher in certain racial populations such as in the New Zealand Maori, Hawaiians and South Pacific Island nations with reported rates of six to seven per 1000 live births.2–4 This epidemiological finding is not explained by socioeconomic features alone, as similar developing countries have reported lower incidence rates than these results.5–8
A genetic component prevalent in the South Pacific group is suggested to explain the higher incidence. Previous studies have focused on Polynesian ethnicity in Maori, Hawaiian and Samoan societies. There is little information regarding the Melanesian populations who are located predominantly in the Solomon Islands, Fiji and Papua New Guinea. Whilst these South Pacific nations are nearby each other, there is evidence of limited common genetic material shared between the Polynesian and Melanesian populations. 9 The Solomon Islands have a demographic that is predominantly Melanesian, who comprise 95% of the population, whilst 3% of the population is Polynesian. 10 Our aim was to investigate the effects of ethnicity on CTEV in the Solomon Islands, specifically to compare the occurrence of CTEV in the Melanesian and Polynesian populations.
Materials and methods
In 2011, a group of paediatric orthopaedic surgeons from Australia conducted the first Ponseti Method Teaching Course for the Solomon Islanders to equip the local medical professionals with the knowledge and skills to treat their patients with CTEV. From the commencement of the programme, meticulous records were kept by the Solomon Islands team using the validated Global Clubfoot Initiative data form. 11 A total of 32 key data points were recorded for each patient, as well as Pirani scoring 12 at each cast change. Information regarding the ethnicity of the mothers and fathers of the affected children was collected either by direct personal reporting or through the experienced clinical staff local to the region who were familiar with the families and their ethnicities. The parents of each child were identified as either Polynesian, Melanesian, Micronesian, mixed or unknown ethnicity. The data was collected over a period of six years from 59 local health clinics across the Solomon Islands (Figs 1 and 2). 13 Statistical analysis was undertaken in Adelaide, South Australia using percentages and odd ratios. MedCalc online statistical calculator (version 19.2.6, MedCalc Softward Ltd, Ostend, Belgium) was used to generate odds ratio, p-value and 95% confidence intervals (CI), with statistical significance set at p < 0.05. Odds ratios were calculated using the study numbers and the Solomon Islands Census data for comparative population numbers of ethnicities. 10
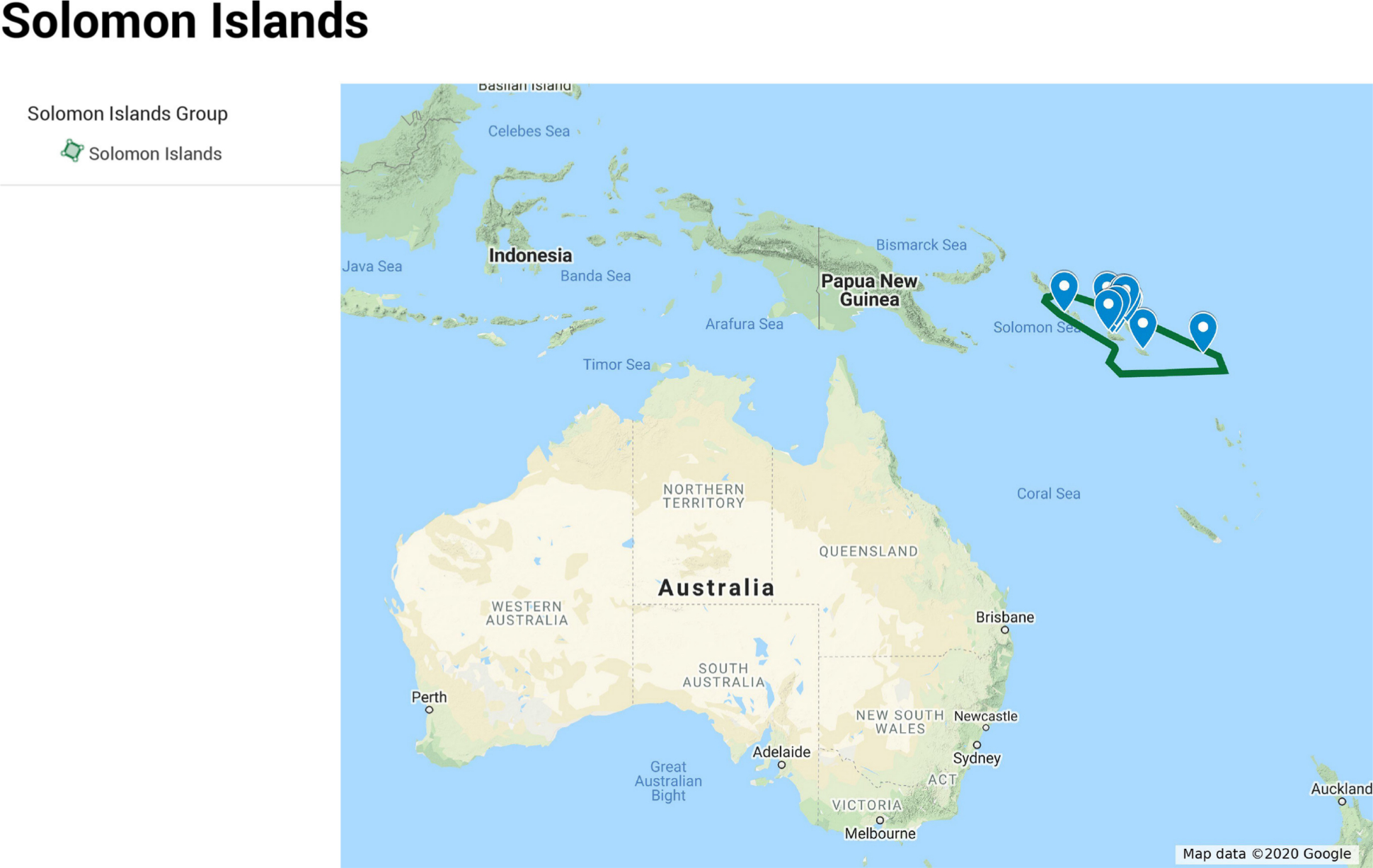
Extended map of the Solomon Islands. 11
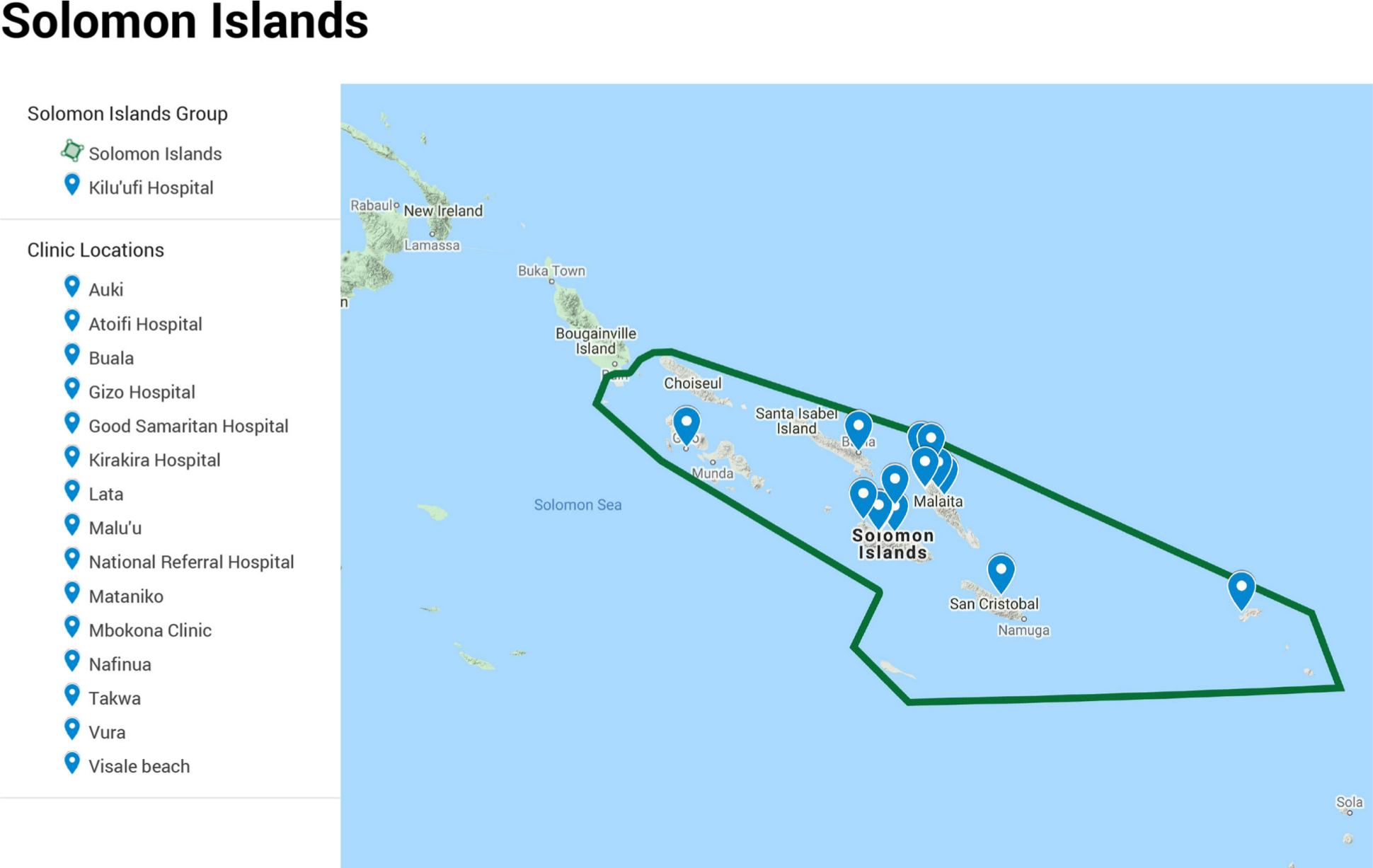
Focused map of some of the clinic locations in the Solomon Islands. 11
Results
Between 2011 and 2017, 138 children presented with CTEV and underwent treatment. There were 77 children with bilateral CTEV (55.8%), making a total of 215 affected feet reviewed and treated. In all, 18 children were suspected to have non-idiopathic CTEV due to clinical syndromal or neuromuscular disorder features on review in clinic.
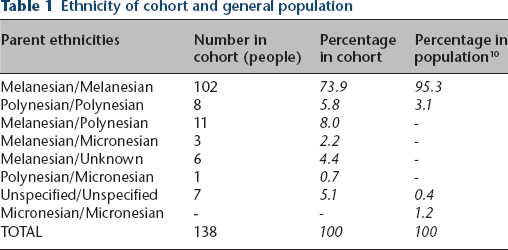
A total of 102 children had solely Melanesian parents (74%), eight children had parents who were both Polynesian (6%), 11 children (8%) were from mixed Melanesian/Polynesian parents and the remaining affected children were from other populations including Micronesian and unknown parent ethnicity (Table 1). Many of the Polynesian cases were from the island groups of Rennell and Bellona, which are known to have a high proportion of Polynesians.
Ethnicity of cohort and general population
Data analysis indicated that in the Solomon Islands, the odds of CTEV in children of Melanesian parents were 0.41-times lower compared with the odds in children of Polynesian parents (p = 0.016; 95% CI 0.20 to 0.85).
There were 49 females affected, with a ratio of approximately 2:1 male to female incidence across all ethnic groups. A positive family history of CTEV was reported in 41 cases (30%). From the cases with at least one Polynesian parent (20) there were seven cases with a known family history (35%).
Bilateral cases were more common in the Polynesian children (87.5%) than the Melanesian children (49%). In the Melanesian children there was slight predominance of right affected feet in unilateral cases; 53% right sided and 47% left sided. There were insufficient numbers in the Polynesian group for analysis of unilateral predominance (Table 2).
Features of cohort by ethnicity

Discussion
Our results show that in the Solomon Islands, there is a lower predominance of CTEV amongst the Melanesian population, compared with the Polynesian population. This supports the view that the Melanesian sub-groups of the Pacific Islands are genetically separate to the Polynesian groups in terms of risk and incidence of CTEV, consistent with evidence from ancestry migration patterns. 9 This is important, as previous research about CTEV demographic data has largely focused on the Polynesian populations in countries of the Pacific Islands, namely New Zealand and Hawaii, rather than other subgroup ethnicities. Furthermore, it supports the hypotheses of migration patterns of the people of the Pacific Islands that have attempted to explain differences between the major groups (Melanesian, Polynesian, Micronesian). Research into genetic material has suggested that the Polynesians may have migrated primarily from the region of Taiwan but progressed quickly through the Papua New Guinea and Solomon Islands groups to settle in the historically more remote regions (New Zealand and Hawaii), whilst Melanesians remained in the near-Oceanic and south-east Asian region. 14 This is consistent with the significant difference in the odds of CTEV we identified between the Polynesians and Melanesians, supporting the theory that a causative genetic variant exists for CTEV. 15
Whilst biological outcomes in research are recommended to be based on race and genetics, rather than ethnicity,16,17 our study highlights the importance of accurate and specific identification of ethnicities for epidemiological purposes. This offers guidance for further research as well as direction for healthcare resources to population groups at risk.
In support of previous literature, our study found that male children were more likely to be affected than female children. Furthermore, the rate of bilateral cases was much higher in the Polynesian children, possibly indicating differing gene penetrance. Of the unilateral cases of CTEV in the Melanesian population, we reported a slight predominance of right sided cases however it was lower than previously reported. 1 More numbers may be required for confirmation however the different side ratio is noted and could reflect some genetic influence.
The percentage of cases with a positive family history was lower than previously reported for the Polynesian populations. Our results were more consistent with reported rates in Caucasian studies with a positive family history of approximately 30%. 2 However, this may be reflective of limited family pedigree data available, or probably that our cases were predominantly Melanesian, which may indicate that their family history rate is similar to that of Caucasian populations, rather than Polynesian. From the cases of CTEV in our study with at least one Polynesian parent, there was a higher percentage of known family history compared with the cases of Melanesian parents alone. This is difficult to explain but could reflect an altered penetration of the presumed genetic defect which promotes the development of CTEV, a theory which has been explored in other studies.3,4,15
Limitations of this study include the biased selection of patients presenting to the Ponseti clinics, both geographically and culturally. The Solomon Islands comprises of over 900 islands and, as such, the Ponseti clinics were set up in areas on the main islands, but could not access every remote regional group. Many islands do not have air access and rely on three- to six-monthly boat trips for trade, often without medical support. Furthermore, our patient group does not reflect the families who chose to visit local ‘bone-setters’; an ancient cultural method of treating bone deformities. The ‘bone-setter’ practice remains commonplace in remote areas, however, community awareness of the Ponseti method is being actively pursued by healthcare providers.
We were unable to determine the national birth defect rates of CTEV due to non-existent government data. More than 80% of children born in the Solomon Islands do not receive formal postnatal newborn care, mostly due to scattered remote rural locations and the inherent limited ability to access appropriate timely healthcare. 18 As such, we were not able to accurately identify an incidence and our sample may show significant under-representation of the population affected with CTEV.
Lastly, the collection method of ethnicity was subjective and full pedigrees were not created. However, the identification of ethnicity was validated by local experts who were familiar with the families through personal knowledge, frequent clinic interactions and their Wantok culture. The study group was based solely in the Solomon Islands and did not include other regions in the South Pacific which have different migration patterns. A similar data collection process is underway in Samoa.
Conclusion
The results of this study indicate that in the Solomon Islands, CTEV is less than half as likely to occur in Melanesian children compared with Polynesian children. Our findings also support the theories of minimal Polynesian genetic material persisting in the Solomon Islands despite the migration of Polynesian ancestors through this region many millennia ago. We report a different genetic risk of CTEV between Polynesians and Melanesians.
Footnotes
Acknowledgements
Thank you to the team involved in the Ponseti programme in the Solomon Islands, including A/Professor Nicole Williams, Helen Burgan, Dr. Patrick Houasia, Dr. Alex Munamua and the excellent local staff. Thank you to the Solomon Islands government and the National Reference Hospital in Honiara. Thank you to the Orthopaedic Outreach of Australian Orthopaedic Association and to the Global Club Foot Initiative.
This study obtained ethics approval from the Solomon Islands Health Research and Ethics Review Board, Ministry of Health and Medical Services; project number HRE032/19.
SSK: Planned and collected the data with the assistance of local team members in the Solomon Islands.
GA: Prepared the data and statistics, Revised the manuscript.
PJC: Senior researcher, Planned and collected the data with the assistance of local team members in the Solomon Islands, Revised the manuscript.