
Abstract
Purpose:
Currently, the optimal time to initiate treatment among preterm infants with clubfoot is unknown. The aim of this study was to describe treatment outcomes up to 1 year post-correction following Ponseti management in infants who were born preterm but treated at term age.
Methods:
A retrospective chart audit was conducted at a major pediatric hospital on preterm infants with clubfoot who commenced Ponseti management at term age (≥37 weeks of gestation). Data are expressed as mean values (±standard deviation) or 95% confidence intervals (95% CIs).
Results:
Twenty-six participants (40 feet) born at 32.6/40 (±3.1) weeks of gestation were identified. Thirteen (50%) were male, 14 (54%) presented bilaterally, and 7 (27%) presented with syndromic clubfoot. Ponseti management was initiated at 41.4/40 (±2.8) weeks gestation. Baseline Pirani scores were 5.2 (95%CI: 4.8–5.6) in the idiopathic group and 5.7 (95%CI: 5.0–6.4) in the syndromic group. The number of casts to correction was 5.9 (95% CI: 5.1–6.6) for those with idiopathic clubfoot and 6.1 (95%CI: 5.0–7.3) for those with syndromic clubfoot. Achilles tenotomies were required in 13 (21 feet) with idiopathic clubfoot and five (7 feet) with syndromic clubfoot. Recurrence occurred in four infants (5 feet): 4 feet required further casting and bracing, and 1 foot required additional surgery.
Conclusion:
Ponseti management at term age in preterm-born infants yields comparable 1-year outcomes to term-born infants. Further research is required to determine whether outcomes beyond 1 year of age align with growth and development demonstrated by term-born infants who are managed with the Ponseti method.
Level of evidence:
Level IV.
Introduction
Congenital talipes equinovarus, or clubfoot, is an orthopedic condition of the foot characterized by equinus, hindfoot varus, forefoot adductus, and cavus deformities. 1 Clubfoot occurs in 1 per 1000 live births,2–4 50% of which present bilaterally.3,5 It affects males twice as often as females and the underlying etiology remains unknown.6,7 Clubfoot can be classified into idiopathic or syndromic subtypes, 1 with idiopathic clubfoot accounting for approximately 80% of all cases. 1 Syndromic presentations occur in conjunction with a multi-system syndrome, resulting in a deformity, which is often more resistant to treatment. 8
Based on the current best evidence, the Ponseti method is regarded as the gold standard of care for the management of clubfoot.2,9 This method involves weekly serial casting spanning an average of 6–8 weeks. 1 Once tarsal alignment is attained, 50%–90% of children require a percutaneous Achilles tenotomy to resolve residual equinus.10–12 Abduction bracing is subsequently applied for 23 h a day for the first 3 months, then during the night and naps until 4 years of age to maintain adequate foot abduction to prevent relapse. 2
Current clinical practice guidelines on the management of clubfoot are based on evidence related to infants born at term (≥37 weeks of gestation). 1 Evidence relevant to preterm infants is lacking. 11 In particular, the optimal age at which infants with clubfoot who are born preterm (< 37 weeks of gestation) should begin treatment remains unknown.3,13–17 The first European consensus meeting on Ponseti clubfoot treatment recommended that Ponseti casting is neither indicated nor well-tolerated in the preterm population until the infant is medically stable. 18 Furthermore, the consensus states that management of clubfoot in preterm infants should be delayed until discharge from the neonatal intensive care unit (NICU) to allow the infant’s foot to grow. 18
Another key concern with commencing Ponseti casting in the NICU is that it may interfere with acute medical and surgical management which are immediately pertinent to the survival and well-being of the infant.11,19 Serial casting may interfere with accurate weight management, venous access for lines and attachments, skin-to-skin care, infant-to-carer bonding, and overall comfort, all of which may complicate the infant’s clinical care in the NICU.11,14,20
A recent review on the initiation of Ponseti management in preterm infants in the NICU concluded that management can be undertaken in the inpatient setting without compromising medical treatment. 11 However, this conclusion was based on the findings of one study. 14 There is currently no research on the outcomes of preterm infants with clubfoot who are managed in the outpatient setting using the Ponseti method at term age following discharge from the NICU.11,21 Therefore, the aim of this study was to investigate the outcomes following Ponseti management in infants with clubfoot who were born preterm and who commenced treatment at term age in an outpatient setting.
Methods
A retrospective chart audit was undertaken to analyze outcomes among infants with clubfoot who were born preterm and referred to The Children’s Hospital at Westmead (CHW). 22 At CHW, all infants with clubfoot who are born prematurely, commence Ponseti management in the outpatient Clubfoot Clinic once they reach term age.
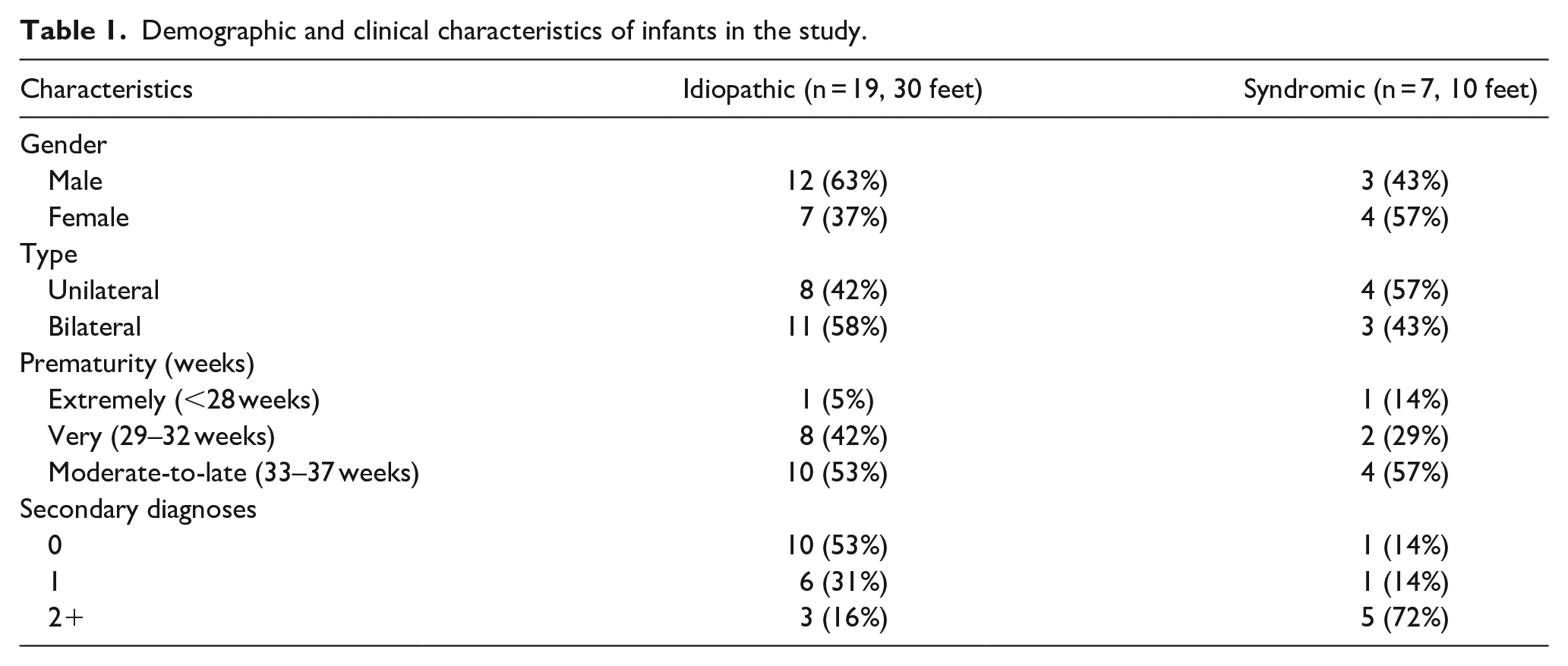
Infants born at less than 37 weeks of gestation and who presented with clubfoot between January 2008 to January 2020 were included. Infants with a diagnosis of atypical clubfoot, who received shared care or commenced treatment prior to term age (<37 weeks gestation) were excluded (Table 1).
Demographic and clinical characteristics of infants in the study.
The primary outcome measure examined was recurrence up to 1 year following initial correction. Recurrence was defined as the return of any components of the clubfoot deformity which required further treatment.11,23 Secondary outcome measures were the number of casts required to achieve initial correction, total time spent in casts, rate of Achilles tenotomy, and incidence of adverse events. The need for Achilles tenotomy was determined by the orthopedic surgeon as a foot which achieved less than 10° of dorsiflexion following initial Ponseti casting. In bilateral clubfoot, concurrent correction of both feet does not always occur, and one foot may remain in a holding cast while the other achieves correction. Correction, therefore, was defined as the point at which a foot achieved an ideal position during casting. 23
Data were analyzed in IBM SPSS Statistics for Macintosh, version 25 (IBM Corp., Armonk, NY, USA). Data were reported as mean values (±standard deviation) and 95% confidence intervals (95% CI) for continuous variables, and frequencies (percentages) for categorical variables. Given the high correlation between pairs of feet in bilateral clubfoot presentations, 10 statistical dependency was managed using generalized estimating equations to determine group estimates.
Compliance with ethics standards
Ethics approval for this retrospective chart audit was obtained through the Human Research Ethics Committee (2019/ETH08716) of the site at which this study was conducted, which granted access to medical records through a waiver of consent. The authors declare no conflicts of interest. The project did not receive any funding.
Results
Twenty-six infants (40 feet) were identified, 19 (30 feet) idiopathic and seven (10 feet) syndromic (Table 1). Of the idiopathic cases, 12 (63%) were male and 11 (58%) were bilateral. In those with syndromic clubfoot, three (43%) were male and three (43%) were bilateral. Associated conditions in those with syndromic clubfoot included arthrogryposis (n = 1), amniotic band syndrome (n = 2), nail patella syndrome (n = 1), rhizomelic bone shortening (n = 1). One infant had both rhizomelic bone shortening and Conradi syndrome, and one was unknown.
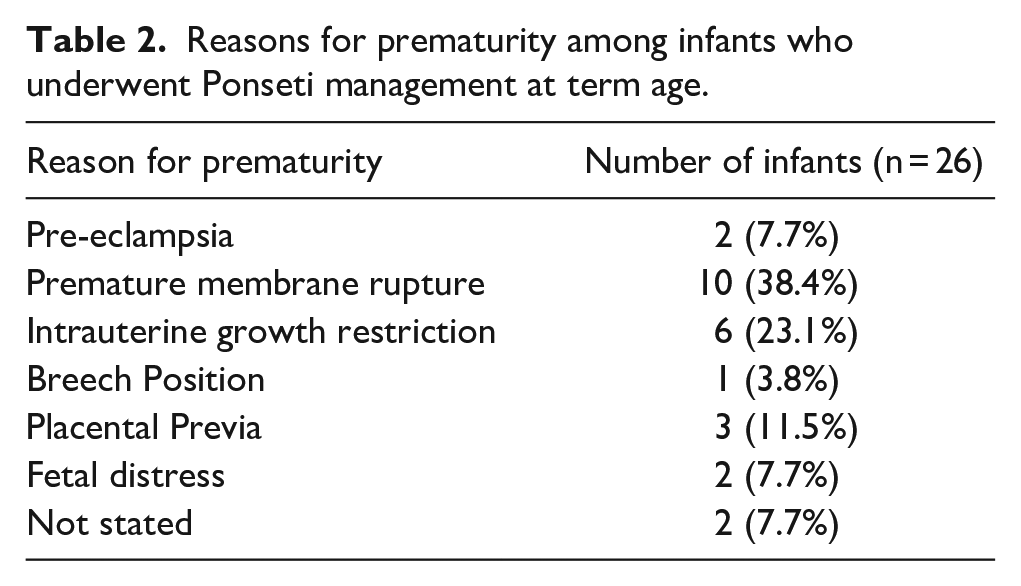
Participants were born on at an average of 32.7/40 (± 2.9) weeks gestation in the idiopathic group and 33.1/40 (± 3.5) weeks in the syndromic group (Table 1). The majority of cases were identified as late premature, having been born between 33 and 37 weeks gestation (Table 1). Reasons for prematurity were documented in 25/26 infants. The most common conditions associated with prematurity were premature rupture of membranes (n = 9) and intra-uterine growth restriction (n = 6) (Table 2).
Reasons for prematurity among infants who underwent Ponseti management at term age.
Commencement of Ponseti management occurred at an average of 41/40 (±3) weeks gestation in those with idiopathic clubfoot and 42/40 (±2) weeks gestation in those with syndromic clubfoot. All participants had 1 year data follow-up.
The average Pirani score prior to application of the first cast was 5.2 (95% CI: 4.8–5.6) in the idiopathic group and 5.7 (95% CI: 5.0–6.4) in the syndromic group. The average number of casts required for correction was 5.9 (95% CI: 5.1–6.6) in the idiopathic group and 6.1 (95% CI: 5.0–7.3) in the syndromic group. The average time spent in casts was 6.0 (95% CI: 5.2–6.9) weeks in those with idiopathic clubfoot, and 6.8 (95% CI: 5.4–8.1) weeks in those with syndromic clubfoot.
Achilles tenotomies were required in 13 participants (21 feet) of the idiopathic clubfoot feet, of which 8/9 infants with bilateral clubfoot required Achilles tenotomies in both feet. In those with syndromic clubfoot, Achilles tenotomies were required in five infants (seven feet), of which two infants had bilateral clubfoot that required tenotomies in both feet.
Following initial correction, all infants were placed into abduction bracing. In those with idiopathic clubfoot bracing included boots and bars (n = 17), knee-ankle-foot orthosis (n = 1), and clubfoot ADM (adduction dorsiflexion mechanism) brace (n = 1). In those with syndromic clubfoot, bracing included boots and bars (n = 5) and knee-ankle-foot orthosis (n = 2).
Within the first year following treatment, recurrence occurred in three infants (three feet) (10%) in the idiopathic group. One infant with bilateral idiopathic clubfoot had a recurrence in only one foot. Recurrences occurred at 3 days, 21 days and 91 days and were managed with repeat Ponseti casts and return to bracing. In those with syndromic clubfoot, recurrence occurred in one infant (two feet) (20%). This occurred at 205 days and was managed with repeat Ponseti casting on one foot and Ponseti casting, tenotomy, and talonavicular stabilization on the other foot.
Adverse events were documented during the initial casting period in four infants (four feet). These included blister formations of the unaffected foot (n = 1) skin irritation of the affected foot (n = 1), skin breakdown of the affected foot (n = 1), and a complex combination of lower limb oedema, cast slippage and eczema of the affected foot (n = 1). These were managed by immediate cast removal until healing allowed the recommencement of regular casting. Adverse events were documented in the recurrence period in one infant who experienced poor brace compliance resulting in a period of casting (1 week) until alternative brace options could be explored.
Discussion
This study demonstrates that 1-year outcomes following treatment of clubfoot in infants born at preterm age but who were managed at term age in the outpatient setting were comparable to outcomes seen in infants with clubfoot born at term age.1,11 Our recurrence rate of 10% (three infants, three feet) in the idiopathic cohort was comparable to Zionts et al. 24 who found that in 176 infants with idiopathic clubfoot, 11% had a recurrence within one year. We found a 20% (one infant, two feet) recurrence rate in infants with syndromal clubfoot after one year, which was lower compared to a systematic review by De Mulder et al. 25 demonstrating a highly variable rate of recurrence (25%–68%); however, their review covered a longer follow-up period of between two and six years following initial treatment.
Infants in this study required a similar number of casts to infants born at term-age, who typically require between three to nine casts in idiopathic clubfoot and four to nine casts in syndromic clubfoot.11,21,26,27 Our study also demonstrated that days in casts were comparable to research that indicated that the Ponseti method required a median 42 days in casts. 28 Finally, the rate of Achilles tenotomy reported in this study, a rate of 63% in idiopathic clubfoot and 70% in syndromic clubfoot, were similar to rates reported in the literature of 50% to 95% and 83% to 100%, respectively, in infants born at term-age.10,12,25,28
The rate of tenotomy in our study was higher compared to Lebel et al., 14 who reported a rate of 13% after commencing Ponseti management during NICU admission in preterm infants. This lower rate may have been due to the biological advantages seen in preterm infants such as ease in tissue manipulation with serial casting alongside rapid growth 11 and increased ligamentous laxity which may contribute to a reduction in need for Achilles tenotomy. 21 The majority of our cohort presented with high baseline Pirani scores (≥ 5) which are correlated with higher rates of Achilles tenotomy. 29 We were unable to determine baseline severity of clubfoot in Lebel et al.’s 14 study which precluded comparison of the baseline characteristics associated with higher rates of Achilles tenotomy. Further research is required to examine the prevalence of Achilles tenotomies in the preterm population.
While rate of recurrence was comparable to the literature, our cohort demonstrated cases where recurrence occurred shortly after initiation of bracing. In two cases, only one cast was required for recurrence, with one infant having a documented change in abduction bracing due to intolerance. Therefore, these may not represent true recurrences of the deformity however either an intolerance of the initial bracing system applied or insufficient initial correction.
Given that outcomes for infants born preterm are comparable to those born at term age, the risks associated with early Ponseti management in the NICU must be weighed against any potential benefit. Early serial casting in infants at preterm age may compromise the integrity of fragile skin and lead to pressure sores, thus increasing their risk of infection in NICU.11,14 A foot length less than 8 cm, at the start of casting, has been associated with additional casting and cast slippage. 30 Furthermore, a smaller foot at the conclusion of casting may not be large enough to fit in widely available abduction bracing. Lebel et al. 14 noted cases of skin irritation and limb oedema in their NICU study, which required emergency cast removal in some cases. Even in our study, which commenced management of preterm infants at term age, adverse events were documented in four cases, all of whom had idiopathic clubfoot. This indicates the need to not only consider the risk of adverse events but the greater consequences of such events in the preterm population by virtue of their developmental fragility.
Preterm infants present with complex and life-threatening acute comorbidities more often compared to infants born at term-age.31–33 In our cohort, greater than 50% of infants were, in addition to their clubfoot diagnosis, identified to have one or more secondary diagnoses. Facilitating skin-to-skin care, accessing venous attachments to monitor vital signs, and monitoring bodyweight have been recognized as additional practical challenges to early Ponseti management in the neonatal setting.11,14 In neonatal infants with unilateral clubfoot, regular casting in the NICU may result in repeated heel lancing on the same (unaffected) heel, which has been shown to cause increased sensitivity to pain during other medical procedures such as venepuncture. 34 Furthermore, concerns around futile care must be closely considered by clinicians when evaluating patients’ holistic and individualized circumstances should infants with life-threatening or significantly life-shortening conditions be treated with Ponseti casting in the premature stages of life.
We hypothesize that early Ponseti management may also interfere with neurodevelopmental care practices and parent-to-infant bonding, all of which are important in promoting optimal neurodevelopment during a significant period of growth and brain development.35,36 Application of casts prevents spontaneous and developmentally appropriate movements in the foot, ankle, and knees of a rapidly growing infant, which may have detrimental effects on neurodevelopment. 35 Furthermore, application of joint-restricting casts and braces may also prevent neurological assessments in the NICU such as the General Movements Assessment 37 and Hammersmith Infant Neurological Examination, 38 both of which are pivotal in the detection of neurological impairments that may lead to the early diagnosis of cerebral palsy. Added benefits of early commencement of Ponseti management in preterm infants needs to be considered against the potential risks. This is particularly pertinent if delayed commencement produces similar treatment outcomes compared to infants with clubfoot who are born at term. Further research is required to determine the impact of Ponseti management on neurodevelopmental care in the neonatal period.
There are limitations to this study. First, this study is limited by a small sample size, larger trials will improve the precision of findings. Second, the 1-year follow-up may not have captured all recurrences. Within syndromic subtypes, large baseline Pirani scores are speculated to “potentiate” recurrence.11,14 Higher Pirani scores were seen across both of our cohorts, suggestive of greater severity of clubfoot which may result in higher rates of recurrence. Longer follow-up is necessary to assess the risk of recurrence beyond one year. Third, the retrospective nature of this study resulted in some missing data. Further prospective studies are needed. Finally, this study did not have a comparison group. Controlled trials will more accurately control for any within study bias.
Conclusion
Pre-term infants who were treated at term required a comparable number of casts and need for tenotomy to achieve initial correction compared to term infants reported in the literature. Similarly, the rate of relapse observed in the present study was also comparable to previous reports of the incidence of relapse in term infants at 1 year of age. As data on preterm infants remain limited, further research is required to determine whether treatment initiation in preterm infants at birth alters outcomes compared to those in which treatment is initiated at corrected term age.
Footnotes
Author contributions
E.S. and K.G.F. collected data and drafted the first manuscript. E.I. analyzed and interpreted the data and contributed to the manuscript. P.G. and K.G. developed the study, interpreted data, and contributed to the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethics approval was obtained through The Sydney Children’s Hospital Ethics Committee (2019/ETH08716).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.