
Abstract
Objectives:
To investigate maternal psychological status of children with congenital talipes equinovarus in different periods, and to clarify the influence on maternal psychological status of congenital talipes equinovarus treated with the Ponseti method.
Methods:
Sixty-seven mothers of children with congenital talipes equinovarus were investigated. Self-rating Depression Scale and Self-rating Anxiety Scale were used to evaluate the psychological stress of the mothers at different periods. Paired-samples t-test was used to analyze the results.
Results:
The mothers of 67 children with congenital talipes equinovarus ranged from 25 to 38 years old, with an average of 33.5 years old. Before prenatal diagnosis of congenital talipes equinovarus, the average score of Self-rating Anxiety Scale was 42.537 ± 10.476, and the average score of Self-rating Depression Scale was 47.254 ± 12.846; after prenatal diagnosis of congenital talipes equinovarus, the average score of Self-rating Anxiety Scale was 54.224 ± 13.050, and the average score of Self-rating Depression Scale was 57.403 ± 13.649 points. Before the postpartum treatment of congenital talipes equinovarus, the average score of Self-rating Anxiety Scale was 53.388 ± 12.716, the average score of Self-rating Depression Scale was 56.284 ± 13.617; after the treatment of congenital talipes equinovarus with the Ponseti method, the average score of Self-rating Anxiety Scale was 47.731 ± 12.259, and the average score of Self-rating Depression Scale was 51.910 ± 13.878 points. The above differences were statistically significant (P < 0.001).
Conclusion:
The prenatal diagnosis of congenital talipes equinovarus will increase the maternal psychological stress, and the maternal psychological status will be significantly improved after the deformity of congenital talipes equinovarus is corrected effectively by the Ponseti method.
Level of evidence:
level III, retrospective study.
Introduction
The congenital talipes equinovarus (CTEV) is one of the most common musculoskeletal malformations at birth, and the main malformations at birth can be divided into four parts: forefoot adduction, hindfoot varus, equinus, and cavus.1–3 Delayed treatment of CTEV can eventually lead to significant disability and seriously affect the quality of life in adulthood, so early identification and treatment are keys to preventing later disability. At present, the development of ultrasonic examination technology has greatly improved the prenatal diagnosis rate of CTEV, and the detection rate of malformation is about 60%.1,4,5 At the same time, the initial correction rate of Ponseti method, the most widely used method in the treatment of CTEV, is close to 100%.6–9
However, in the clinical diagnosis and treatment of CTEV, we should also pay equal attention to the psychological condition of the mother. Relevant studies have shown that due to the significant changes in steroids and polypeptide hormones 10 and other factors, mental health problems of women during pregnancy and postpartum are currently considered to be the most common pregnancy complications, 11 among which depression and anxiety are the most common mental diseases during pregnancy and postpartum. 12 These mental diseases have negative effects on mothers, children, and families.10,11,13–16 Some common congenital diseases—such as cleft lip and palate, heart malformation, and Down’s syndrome—have been confirmed to induce anxiety or depression in mothers,17,18 but there has been no report on the effect of CTEV on the maternal psychological mood. Therefore, this study intends to evaluate the psychological stress level of mothers of children with CTEV in different periods through Self-rating Depression Scale (SDS) and Self-rating Anxiety Scale (SAS), so as to provide a basis for ensuring the clinical diagnosis and treatment effect of CTEV and improving the maternal psychological status.
Patients and methods
In this study, the mothers of 67 children with CTEV were selected. The depression and anxiety of their mothers in the four periods before prenatal diagnosis of CTEV, after prenatal diagnosis of CTEV, before treatment of CTEV, and after treatment of CTEV were evaluated. In order to objectively evaluate the maternal psychological status and effectively analyze the influencing factors of psychological problems, all cases in this group met the following criteria: (1) first pregnancy; (2) prenatal ultrasound examination showed isolated CTEV; (3) single pregnancy; (4) pregnant women aged from 25 to 38 years old; (5) no physical and mental illnesses of the pregnant women before delivery examination; (6) all fetuses were diagnosed with idiopathic CTEV after birth; (7) the Ponseti method was used for treatment after birth; (8) the Pirani score of abnormal foot was 0 after the Ponseti treatment.
In the diagnosis of CTEV, all subjects were diagnosed by prenatal ultrasound diagnosis and postpartum clinical diagnosis, and we took the postpartum clinical diagnosis of CTEV as the final result. All patients were treated by the Ponseti method. First, the forefoot adduction, hindfoot varus, and cavus were corrected by manipulation therapy and a series of casts, and then the residual equinus was corrected by percutaneous Achilles tenotomy. After the operation, the affected limb was fixed in a cast over the knee position. After 3 weeks, the cast was removed and the Dennis-Brown splint was worn to maintain the abduction of the affected foot at 60° and the normal foot abduction at 30°. It was worn all day for the first 3 months and only at night after 3 months, no less than 16 h a day until the child was 4 years old to maintain the correction effect.
In this study, the SDS was used to evaluate the depression of the children’s mothers in four periods. The children’s mothers filled in independently according to their personal feelings on the premise of clarifying the meaning of the problem. SDS consists of 20 questions, each of which has four levels. For forward scoring questions, A, B, C, and D are scored as 1, 2, 3, and 4; for reverse scoring questions, 4, 3, 2, and 1 are scored. Add the scores of 20 questions to get rough total score, multiply the rough total score by 1.25, and take the integer part to get the standard score. The reference value of the upper limit of normal for the standard score is 52 points, 53–62 points for mild depression, 63–72 points for moderate depression, and 72 points or more for severe depression.
In this study, the SAS was used to evaluate the anxiety of children’s mothers in four periods. SAS also consists of 20 questions, all of which are graded according to four levels. The method of scoring and obtaining standard scores is the same as SDS. The dividing value of the standard score is 50, below 50 is normal, 50–59 is mild anxiety, 60–69 is moderate anxiety, and 70 or above is severe anxiety. Statistical analysis was done using SPSS 10.0 software package (SPSS, Chicago, IL, USA), and paired-samples t-test method was used to analyze the difference of SAS and SDS evaluation results in four periods: before prenatal diagnosis of CTEV, after prenatal diagnosis of CTEV, before treatment of CTEV, and after treatment of CTEV.
Results
Overview of maternal psychological status
First, the score data were processed to get a preliminary impression of the maternal psychological pressure in each period. As shown in Table 1, the maternal psychological pressure was at a normal level before the prenatal diagnosis of CTEV, and changed to a mild state of depression and anxiety after the prenatal diagnosis of CTEV. There was no change in the period before the treatment of CTEV, and it returned to the normal level after the treatment of CTEV.
Mean and standard deviation of SAS and SDS scores of mothers in different periods.
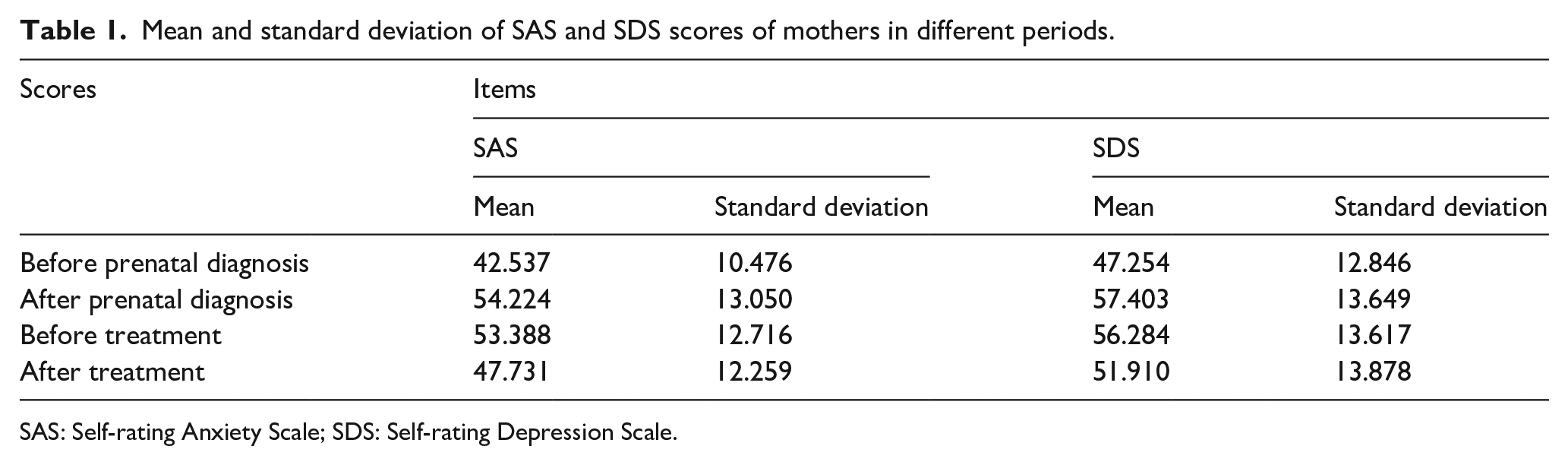
SAS: Self-rating Anxiety Scale; SDS: Self-rating Depression Scale.
Then, we calculated the SAS and SDS standard scores of each case, and constructed four coordinate systems corresponding to the four periods with SAS standard score as the horizontal axis and SDS standard score as the vertical axis. In this way, each case corresponded to a data pair in each period, and the data pairs of each case in the corresponding period were placed in the coordinate system. Thus, four dot graphs as shown in Figure 1 were obtained. In the coordinate system, eight dividing lines of “normal, mild, moderate and severe” were made according to SAS and SDS grading standards, and the whole coordinate system was divided into 16 regions. The data distribution in each region is shown in Table 2.
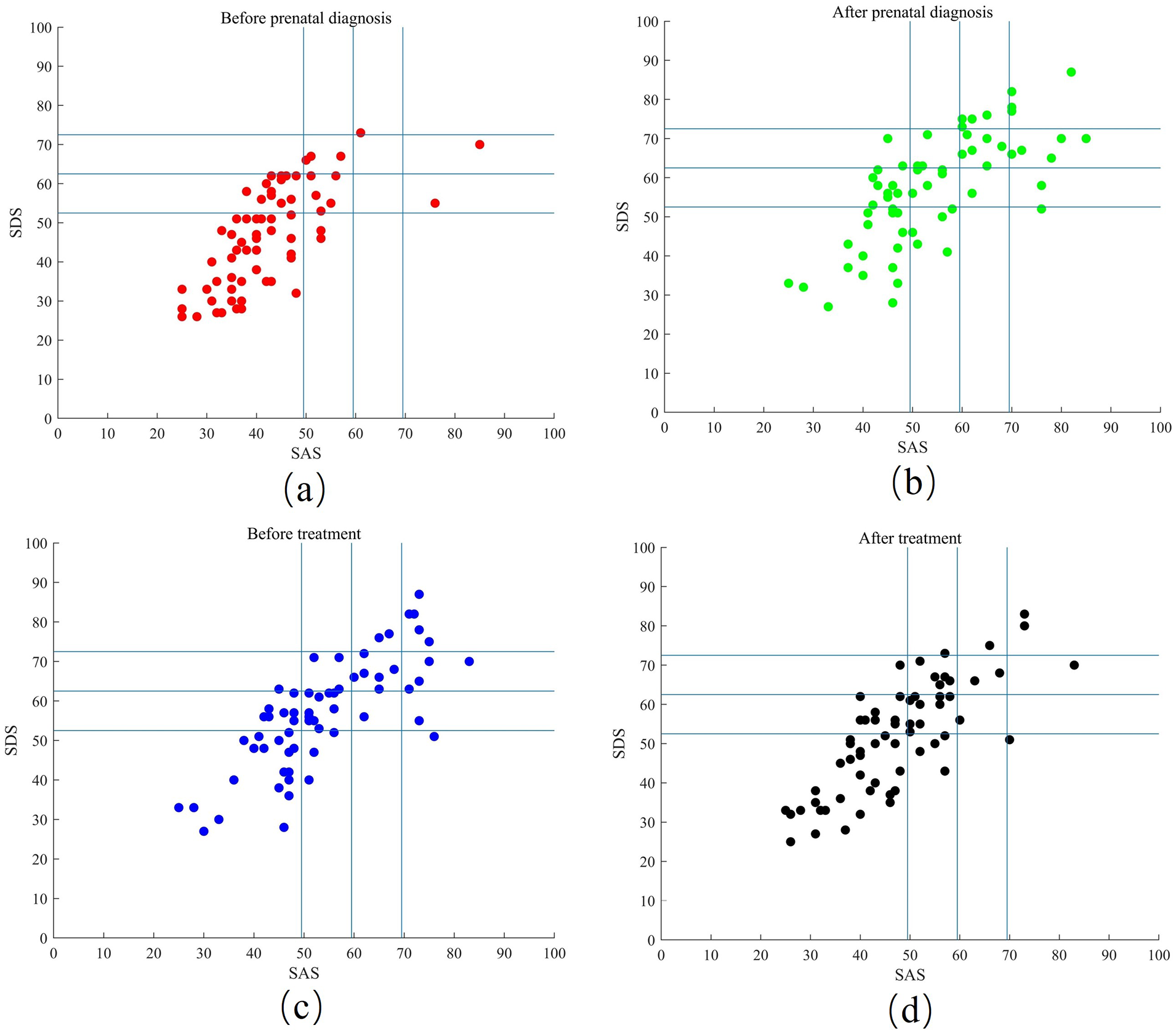
Scatter plot of results of depression and anxiety of mothers in different periods. (a) Before the prenatal diagnosis of CTEV, most of mothers have normal psychological state, only six mothers have moderate or severe psychological stress. (b) After prenatal diagnosis of CTEV, most of mothers had mild to severe psychological pressure and only 19 mothers were in normal psychological state; (c) before treatment of CTEV, there are 11 mothers with moderate psychological stress and 13 mothers with severe psychological stress. (d) After treatment of CTEV, most of mothers have normal psychological state, and only 16 mothers have moderate or severe psychological stress.
Results of depression and anxiety of mothers in different periods.
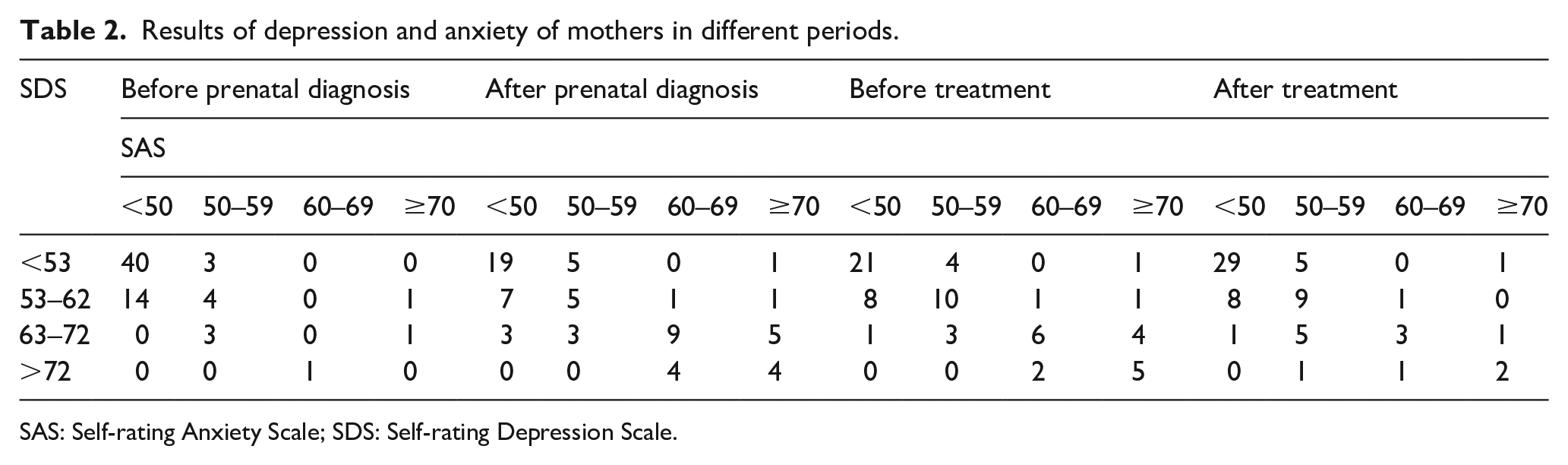
SAS: Self-rating Anxiety Scale; SDS: Self-rating Depression Scale.
In this study, we used SAS and SDS to evaluate the maternal psychological state. It is stipulated that meeting SAS standard score <50 and SDS standard score <53 is “normal psychological state,” meeting the SAS or SDS highest grade is mild is “mild psychological stress,” and meeting the SAS or SDS highest grade is moderate is “moderate psychological stress.” If the highest rating of SAS or SDS is severe, it is defined as “severe psychological stress.”
As shown in Figure 1(a), before prenatal diagnosis of CTEV, 59.7% of the mothers were in normal psychological state, 31.3% had mild psychological pressure, and 4.5% had moderate and severe psychological pressure. As shown in Figure 1(b), after prenatal diagnosis of CTEV, 28.3% were in normal psychological state, 25.4% had mild psychological pressure, 23.9% had moderate psychological pressure, and 22.4% had severe psychological pressure; As shown in Figure 1(c), before postpartum treatment of CTEV, 31.4% were in normal psychological state, 32.8% had mild psychological pressure, 16.4% had moderate psychological pressure, and 19.4% had severe psychological pressure. As shown in Figure 1(d), after postpartum treatment of CTEV, 43.3% were in normal psychological state, 32.8% had mild psychological pressure, 14.9% had moderate psychological pressure, and 9.0% had severe psychological pressure.
Combined with the results in Figure 1 and Table 2, we can get the change trend of the maternal psychological status in four periods: the maternal psychological status was normal before the prenatal diagnosis of CTEV, while after the prenatal diagnosis of CTEV, 50% of the children’s mothers had abnormal psychological status, and the mothers with moderate to severe psychological pressure increased greatly. This showed that the diagnosis of CTEV had a great negative impact on the maternal psychological status. After the treatment of CTEV with the Ponseti method, the number of mothers with normal psychological status and the maternal psychological status with different degrees of psychological pressure were significantly improved, which showed that the psychological pressure of the mothers was also significantly improved after the Ponseti method treatment.
Changes in the psychological status of the mothers in different periods
As shown in Table 3, the average SAS score difference of 67 mothers before and after the diagnosis during pregnancy was −9.299, and the difference was statistically significant (P < 0.001), indicating that the SAS score after the diagnosis during pregnancy was significantly higher than that before the diagnosis during pregnancy. The average difference of SAS scores between those diagnosed during pregnancy and those before postpartum treatment was 0.597, which was not significant, indicating that the SAS scores before postpartum treatment were slightly higher than those diagnosed during pregnancy, but there was little statistical significance. The average difference between before and after postpartum treatment was 4.522 (P < 0.001), indicating that the SAS score after postpartum treatment was significantly lower than that before postpartum treatment.
Analysis of the maternal psychological stress in different periods with SAS.
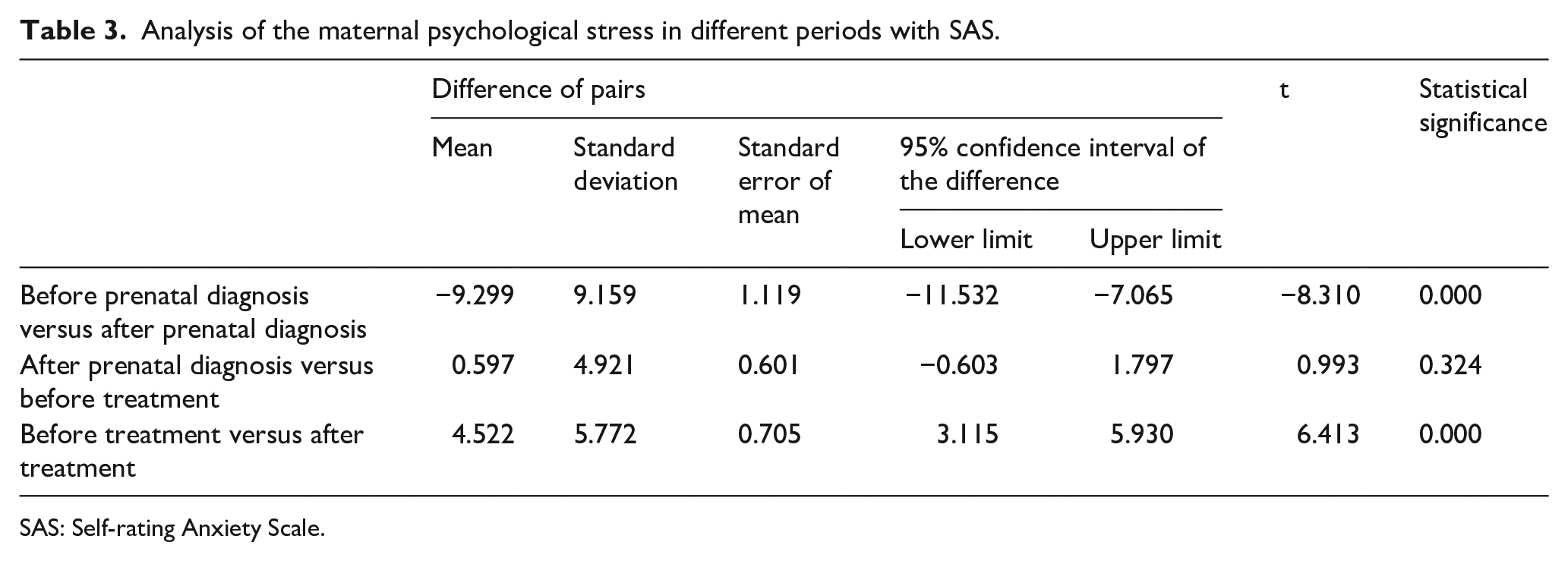
SAS: Self-rating Anxiety Scale.
As shown in Table 4, the average SDS score difference of 67 mothers before and after the diagnosis during pregnancy was −8.143, which was statistically significant (P < 0.001), indicating that the SDS score after the diagnosis during pregnancy was significantly higher than that before the diagnosis during pregnancy. The average difference of SDS scores between those diagnosed during pregnancy and those before postpartum treatment was 0.896, which was not significant, indicating that the SDS score before postpartum treatment was slightly higher than that after prenatal diagnosis, but there was little statistical significance. The average difference between before and after postpartum treatment was 3.537 (P < 0.001), indicating that the SDS score after postpartum treatment was significantly lower than that before postpartum treatment.
Analysis of the maternal psychological stress in different periods with SDS.
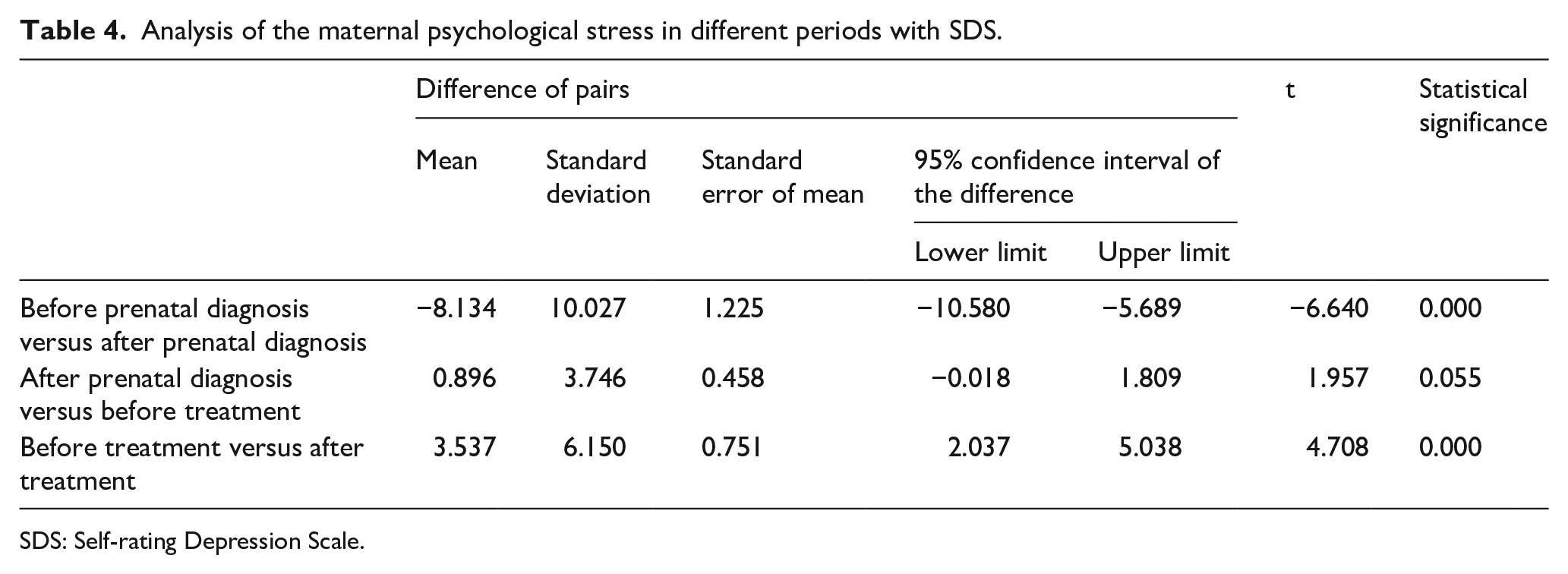
SDS: Self-rating Depression Scale.
The psychological changes of mothers were analyzed by paired-samples t-test between the four different periods as showed in Table 3. The results indicate that the diagnosis of CTEV significantly aggravates the anxiety and depression of the mothers, indicating that the diagnosis of CTEV will have a certain negative impact on the maternal psychology, and the treatment of CTEV with the Ponseti method can significantly improve the anxiety and depression of the mothers, which shows that after the treatment of the Ponseti method, not only can the deformity of the child be corrected but also the maternal psychological pressure can be obviously alleviated, and it has a dual therapeutic effect of physiology and psychology.
Discussion
The CTEV is one of the most common foot deformities in children. The initial treatment methods include extensive soft tissue releases and bone surgery, but most of these methods will lead to foot stiffness, arthritis problems, poor quality of life, recurrence of deformity, and other adverse consequences, which once made the treatment of CTEV a problem.19–21 In 1963, the Ponseti method completely changed the treatment concept of CTEV. Numerous studies show that the Ponseti method has shorter correction time, less cost, lower recurrence rate, and fewer complications than other methods, and its treatment success rate is close to 100%.1,20,21 With its advantages of simple operation, easy popularization, low economic cost, and excellent treatment effect, the Ponseti method has now become the recognized first choice for the treatment of CTEV.
Prenatal diagnosis of fetal clubfoot is very important for the early detection and treatment of CTEV. Accurate prenatal diagnosis can enable pregnant women to carry out prenatal consultation in advance, know the treatment, and prognosis of CTEV. Given the considerable number of malformations associated with clubfoot, such as cleft lip and palate, micrognathia, congenital heart defects, hydrocephalus, myelomeningocele, and other structural abnormalities, prenatal diagnosis can also inform treatment planning for clinicians.22–25 This study found that the diagnosis of CTEV in children will increase the degree of anxiety and depression of mothers. First, the appearance of deformed children violates the expectations of parents who want to have a healthy child. Second, the current treatment process of CTEV is very long, which is a long-term restriction on the activities of legs and feet of infants. There is evidence that the activities of infants’ legs and feet play a core role in exploring the environment. This treatment process is undoubtedly painful for children and parents, especially when children are disapproving. In addition, not all medical institutions have the ability to implement corrective treatment, which means that families need to go to distant places for treatment many times, which is also one of the sources of psychological pressure. 16 In addition, there is also evidence that excessive psychological stress during pregnancy may have a negative impact on children’s development: prenatal depression will lead to fetal reprogramming of the fetus, 10 decreased vagal nerve tone of newborns, changes in responsiveness to pain or stress, physical movement, and cognitive development delays. 15 And there is a strong correlation between prenatal and postpartum depression; 14 it will affect children’s growth in the form of direct interaction with caregivers in turn. Based on the adverse effects of CTEV on the child’s mother and family, we suggest that the mother should undergo psychological evaluation after the diagnosis of the disease, early detection and early intervention, patients should be encouraged to make full use of social resources and social support, and the hospitals should provide emotional and information support.
The results of Coppola’s study showed that mothers of babies with a diagnosis of clubfoot had significantly more stress-related anxiety and depression than those of healthy ones. It is similar to our results that the prenatal diagnosis of CTEV significantly aggravates the anxiety and depression of the mothers. They also found that social support was negatively related significantly with both depression and stress in mothers of babies with clubfoot; they thought social support might help mothers to reduce the negative impact of the illness on their psychological well-being. 16 Radler et al. 26 also found that contact between future parents and the mothers with children undergoing active treatment appears to help future parents fully understand the implications of the diagnosis, implying the need for a more complete system in the future, to provide a platform for mothers of children with CTEV to communicate and encourage each other. Interestingly, studies have confirmed that pregnant women prefer to know a possible clubfoot diagnosis in advance rather than at birth, and the vast majority of mothers express a desire to know about the deformity before birth.4,26 This suggests that if we provide timely prenatal counseling to mothers and clearly explain the clinical manifestations, treatment of the Ponseti method, and prognosis of congenital clubfoot, including social support, it may have a positive effect on the treatment of the CTEV and reduce the level of anxiety and depression of the mothers.
In this study, it is not difficult to conclude that after treatment with the Ponseti method, the anxiety and depression of mothers have been significantly improved, which confirms the practicability of the Ponseti method, which can not only correct the deformity of children but also alleviate the maternal psychological pressure. Therefore, we suggest that the maternal psychological status should be evaluated while diagnosing and treating CTEV, so as to ensure the mental health of the mothers.
Conclusion
The diagnosis of CTEV will increase the maternal psychological pressure to varying degrees, and the maternal psychological status will be significantly improved after the deformity of CTEV is corrected effectively by the Ponseti method. In the whole process of diagnosis and treatment of CTEV, we suggest not only to pay attention to the therapeutic effect of CTEV of children but also to ensure the mental health of the mothers.
Footnotes
Acknowledgements
The authors thank Yang Jidong, Cui Chen, and Fan Zongrui for their contributions to the statistical processing and analysis of data. The authors also thank all of the colleagues who participated in this study for their time, insight, and collaboration.
Author contributions
W.D., MD contributed to the statistical analysis and manuscript preparation. N.S., MD performed the psychological evaluations and manuscript preparation. C.W., MD performed the psychological evaluations. Y.Z., MD contributed to the study design and manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Each author certifies that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article. All ICMJE Conflict of Interest Forms for authors and Journal of Children’s Orthopaedics editors and board members are on file with the publication and can be viewed on request. This work was performed at Shenzhen University General Hospital, Shenzhen, P.R. China.
Ethical approval
This study did not directly involve human participants and/or animals. Each author certifies that all investigations were conducted in conformity with ethical principles of research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Basic Research and Free Exploration Project of Shenzhen Science and Technology Innovation Commission of China (JCYJ20180305125332754), the Basic Research General Project of Shenzhen Science and Technology Innovation Commission of China (JCYJ20190808153011417), the Natural Science Foundation of Shenzhen University General Hospital in China (SUGH2018QD009), and the Sanming Project of Medicine in Shenzhen of China (no. SZSM201911011).
Informed consent
Informed consent was not required for this study.