
Abstract
Abstract
Background
The clinical features that define congenital talipes equinovarus (CTEV) are the presence of four principal components, equinus, varus, adductus and cavus. Classification systems in CTEV often include a form of assessment of these components and also other concurrent clinical parameters which feature in the condition.
Methods
Over a 14-year period from 1992 to 2006, 95 consecutive cases of CTEV were prospectively assessed and data recorded in order to investigate the relationships between the clinical parameters in CTEV and to compare these relationships with those that one would expect from our knowledge of the pathological anatomy and mechanics of the condition, relating these findings to the commonly used systems for classification.
Results
Ninety-five cases of CTEV had failed conservative treatment and had undergone surgical release. The mean age at surgical release and assessment was 9 months. Cluster analysis demonstrated that there were, broadly, two groups of patients. The first group was those patients with a greater equinus deformity (greater than 31°). This group had a greater adductus deformity and the presence of other parameters indicating increased severity (multiplanar stiffness with the presence of cavus and medial skin crease). The second group was those patients with a smaller equinus deformity (less than 31°) who were more heterogenous with regards to the other parameters.
Conclusions
We analysed on a statistical basis the relevant aspects of the deformity in CTEV. We have demonstrated that there are certain parameters, namely, equinus and adductus, whose severity can reasonably predict the severity of other components of the deformity. With regards to hindfoot parameters, increased equinus is related to less sagittal plane reducibility and to stiff hindfoot varus (coronal plane stiffness). In terms of midfoot parameters, the degree of adductus is related to the presence of cavus deformity and the presence of a medial skin crease is associated with less reducibility of the adductus (axial plane stiffness). This is consistent with our current understanding of the pathological anatomy of CTEV and bears implications with regards to treatment and the design of proposed classification systems that are in use.
Introduction
The clinical features that define congenital talipes equinovarus (CTEV) are the presence of four principal components, equinus, varus, adductus and cavus. Classification systems in CTEV often include a form of assessment of these components and also other concurrent clinical parameters which feature in the condition. These have included supination, medial and posterior skin creases, assessment of subtalar, ankle, and midtarsal joint stiffness and reducibility, calf size, curvature of the lateral border and condition of the heel.
From a pathological viewpoint, both neuromuscular and vascular aetiologies have been described. These result in anatomical abnormalities which afflict the osseous, ligamentous and tendinous structures of the foot and ankle, and have been described in detail in cadaveric and, more recently, magnetic resonance (MR) studies [1–5]. How these individual structural abnormalities are related to one another and how they culminate in the characteristic clinical picture have been described by those investigating the pathomechanics of CTEV and also the mechanics of the normal foot and ankle (in some respects, the CTEV foot can be considered as an exaggerated fixed normal equinovarus position).
The aim of this study was to investigate the relationships between the clinical parameters in CTEV and to compare these relationships with those that one would expect from our knowledge of the pathological anatomy and mechanics of the condition, and relate these findings to the commonly used systems for classification.
Patients and methods
Over a 14-year period from 1992 to 2006, 95 consecutive cases of CTEV were prospectively assessed and their data included in this study. These cases had been referred to the senior author (R.W.P.) and had subsequently failed initial conservative treatment with either stretching and strapping, with or without casting, using the Kite method (67 cases, 1992–2003) or the Ponseti method 28 cases (2003 onwards). These cases underwent surgical release using the Cincinnati approach. Thus, postural types of CTEV were excluded and the more severe forms of CTEV were the subject of this investigation.
While anaesthetised and prior to surgical release, clinical assessment of the deformity was made. Table 1 presents a list of the parameters evaluated. All measurements were carried out and recorded by the senior author (R.W.P.). Equinus was assessed using a goniometer along the lateral border of the foot and ankle with the foot in a passively corrected position. A concurrent assessment was made of the reducibility of the equinus (sagittal plane stiffness; ‘0’ being partly or completely reducible and ‘1’ being irreducible). Adductus was assessed using a goniometer on the plantar aspect of the foot with the forefoot corrected relative to the hindfoot. Reducibility of the adductus deformity provided an evaluation of the axial plane stiffness, recorded as ‘0’ or ‘1’ (‘0’ being partly or completely reducible and ‘1’ being irreducible). The presence of cavus was assessed by observing from the medial side and noting whether the line between the medial malleolus and head of the first metatarsal was straight or curved. The presence of a medial skin crease was recorded. An assessment was made of the varus heel position, the reducibility of which gave an indication of the coronal plane stiffness (‘0’ being partly or completely reducible varus heel and ‘1’ being irreducible varus heel).
The seven clinical parameters of congenital talipes equinovarus (CTEV) assessed in this study
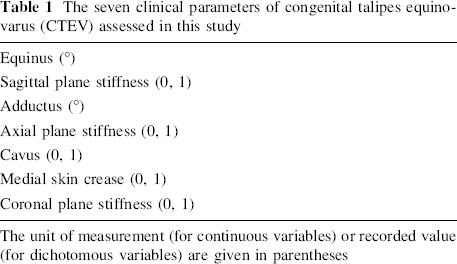
The unit of measurement (for continuous variables) or recorded value (for dichotomous variables) are given in parentheses
Data analysis was performed using SPSS statistical software (SPSS Inc., Chicago, IL, USA). Initial pair-wise comparisons between variables were performed after establishing what relationships may be expected on the basis of our prior knowledge of the pathoanatomy and mechanics of CTEV. Correlations were performed using Spearman's rank-order correlation coefficient when two interval variables were investigated, Cramer's V-test in the case of two dichotomous variables and the point-biserial correlation coefficient when one interval and one dichotomous variable were correlated. Associated P values were calculated and, using an overall alpha level of 0.05 as denoting significant, the Sidak–Bonferroni adjustment was made for multiple comparisons. The P value was deemed to be significant at P = 0.00465.
Further statistical analysis was performed using two-step cluster analysis in order to attempt to identify natural groupings (or clusters) of similar cases within the dataset. Analysis of these clusters would give an indication as to what combination and values of parameters are associated with one another.
Results
Over the 14-year period of study, a total number of 95 cases of CTEV had failed conservative treatment and had undergone surgical release. The mean age at surgical release and, hence, at the time of assessment was 9 months (standard error of the mean, SEM, 0.8). Twenty-three patients (24%) had bilateral CTEV requiring surgical correction. A further 33 patients (35%) also had bilateral CTEV but the contralateral side had responded satisfactorily to conservative treatment and only the data pertaining to the side undergoing surgical correction was included in the study.
Table 2 presents the results of the pair-wise correlations made between parameters.
Results of the pair-wise correlations between variables
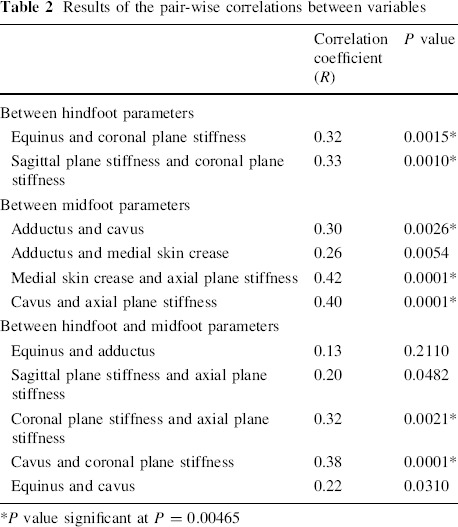
P value significant at P = 0.00465
Cluster analysis was performed, which demonstrated that there were, broadly, two groups of patients. Group 2 (Figs. 1, 2, 3) were those with a greater equinus deformity (greater than 31°). This group, inevitably, had a greater adductus deformity and presence of other parameters indicating increased severity (multiplanar stiffness with the presence of cavus and medial skin crease, Fig. 3).
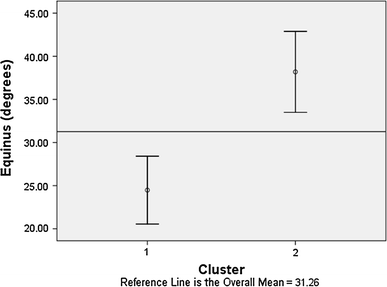
Graph depicting the mean and 95% confidence interval for equinus in the two clusters. Cluster 2 includes those patients with equinus greater than 31° and Cluster 1 includes those with less than 31° of equinus
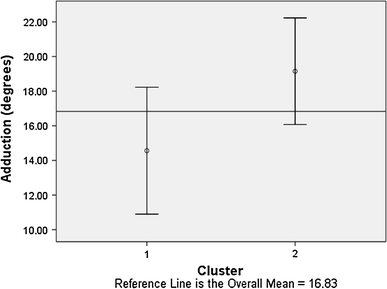
Graph depicting the mean and 95% confidence interval for adductus in the two clusters. Cluster 1 has a wider confidence interval with a greater range of adductus, whereas Cluster 2 includes patients with greater than 16° of adductus

Graphs demonstrating the relative contributions of the dichotomous variables to each cluster. Feet belonging to Cluster 2 all had the presence of coronal, axial and sagittal stiffness and the presence of cavus and medial skin crease. Those belonging to Cluster 1 had variable presence of these parameters
Group 1 of the cluster analysis (Figs. 1, 2, 3) tended to have smaller equinus deformity (less than 31°) and were more heterogenous with regards to the other parameters (Figs. 2, 3).
Discussion
Our data has demonstrated the relationship between various clinical parameters of CTEV. With regards to hindfoot parameters, increased equinus is related to less sagittal plane reducibility and to stiff hindfoot varus (coronal plane stiffness).
In terms of midfoot parameters, the degree of adductus is related to the presence of cavus deformity and the presence of a medial skin crease is associated with less reducibility of the adductus (axial plane stiffness).
There is an association between the position and reducibility of the heel and certain midfoot parameters, including cavus and the presence of fixed adductus.
Cluster analysis has demonstrated that those patients with severe equinus (greater than 30°) always had multiplanar stiffness, the presence of cavus and a medial skin crease.
For those patients with equinus less than 30°, the adductus tended to be more variable as was other parameters of the deformity.
These findings would be expected from our knowledge of the pathological anatomy of CTEV [6]. Anatomically, equinus, varus, cavus and adductus are considered to be composites of deformities which include abnormalities of the ankle, subtalar, midtarsal joints and the forefoot. The primary osseous abnormality is the talus, which is plantar flexed with associated plantar and medial deviation of the talar neck [1–5]. Plantar flexion of the talus is associated with tightness of the posterior tibiotalar capsule [6]. The calcaneus and navicular move in unison around the talus (the talocalcaneonavicular joint) [6]. The anterior end of the calcaneus is medially deviated and lies under the head of the talus. The medial displacement of the calcaneus and navicular contributes to the adductus and cavus deformities. The posterior end of the calcaneus moves upward and towards the fibula (into varus) with tightening of the tendo Achilles and calcaneofibular ligament [7]. The cuboid follows the anterior end of the calcaneus with contraction of the calcaneocuboid and cubonavicular oblique ligament. This contributes to both the supination and adductus deformities. The degree to which any of these component anatomical anomalies contribute to the overall clinical picture may vary with each patient; however, all are intimately related to each other. Together, they produce the clubfoot deformity, but they are not discrete, isolated elements.
Studies of the kinetics of the tarsus would also suggest that elements of the clubfoot deformity are closely related. Brockman described the deformity as a fixed exaggeration of the normal equinovarus position [8]. The concept of a link mechanism between the medial and lateral rays would suggest that movements of the hindfoot and forefoot are related [9, 10]. The direct relationship between subtalar and midtarsal motion was demonstrated by Lapidus and confirmed by others [11]. Huson [12] described the tarsal complex (subtalar, talonavicular and calcaneocuboid joints) as forming a closed kinetic chain with interdependence of motion.
One of the disadvantages of this study was that our patient population consisted of those individuals that had previously had conservative methods applied and that these findings would, therefore, potentially not be applicable to the pre-treatment clubfoot. However, given that recent MR studies analysing the pathological anatomy of CTEV following conservative management for failed conservative treatment have found the anatomy to be consistent with that found in dissection and MR studies of CTEV prior to such treatment; we feel that our results could be extrapolated to this group of patients [1–5, 13, 14].
Our assessments were made with patients under general anaesthetic, which may possibly not reflect those made in a clinical setting. However, the advantage of general anaesthesia is that it enables an accurate and more thorough assessment of deformity and correctability to be made without any discomfort to the patient.
Multiple classifications have been developed to date in order to describe the deformity and assess the results from treatment. The most commonly used classifications are those based on clinical evaluation and are those of Harrold and Walker, Pirani et al. and Diméglio et al. [15–17]. The system proposed by Harrold and Walker is the simplest to apply and, as has been demonstrated by our analysis, would imply the degree of severity of a number of aspects of the deformity besides the equinus it measures [15]. Its usefulness in terms of predicting response to treatment has been confirmed and a recent study, investigating its reliability, demonstrated that it was the most reliable when used by all observers involved in the study [18, 19]. However, we have demonstrated that the assessment of adductus would add information, as this does appear to be the parameter most resistant to treatment, conservative or surgical [20]. This would also be supported by our findings, as adductus appears not to be directly correlated with equinus in those feet resistant to conservative treatment with a smaller equinus deformity (i.e. less than 30°).
Diméglio's [17] classification assesses four components of the deformity, namely, equinus, varus, adductus and derotation of the calcaneopedal block around the talus, and assigns attributes of up to four points to each. There are four additional points for the presence of a medial skin crease, posterior skin crease, cavus and poor calf musculature. This classification is inherently more complex than others mentioned here, although it has been shown to be reliable [19, 21]. Our findings would suggest that a number of the parameters measured using this system are inherently related and, therefore, the system is potentially more complex than it needs to be. For example, the reducibility of varus and the degree of equinus have been shown to be correlated. The derotation of the calcaneopedal block is a composite of the reducibility of the varus, adductus and cavus, and we have demonstrated the inter-relationship of coronal plane stiffness, axial plane stiffness and the presence of cavus (Table 2). The additional points for the presence of medial skin crease and cavus would seem unnecessary given their relationship to adductus (Table 2) and the presence of poor calf musculature would appear to be a fairly subjective parameter.
Pirani's classification has been independently evaluated and found to be as reliable as the Diméglio classification [16, 21]. It assesses the hindfoot through assessment of the posterior skin crease, emptiness of the heel and rigidity of the equinus. It assesses the midfoot through evaluation of the medial skin crease, curvature of the lateral border and position of the lateral part of the head of the talus. The Pirani score has been shown to predict the need for tenotomy and the duration of treatment using the Ponseti method, and its 50–50 divide between hind and midfoot assessment is supported by our findings of equinus and adductus being the two most apparent major determinants of the overall clinical deformity [22].
In summary, the aim of this study was to analyse on a statistical basis the relevant aspects of the deformity in CTEV. We have demonstrated that there are certain parameters, namely, equinus and adductus, whose severity can reasonably predict the severity of other components of the deformity. This is consistent with our current understanding of the pathological anatomy of CTEV and bears implications with regards to treatment and the design of proposed classification systems that are in use.