
Abstract
Climate change is a well-recognized threat to human health with impacts on every organ system and with implications for disease processes across subspecialties. Climate-driven environmental exposures influence the pathophysiologic underpinnings of disease emphasized in the pre-clinical years of medical school. While medical schools are beginning to offer climate change and health electives, medical education is lagging in providing fundamental climate-and-health content to adequately prepare the next generation of physicians for the challenges that they will face in the provision of healthcare and the prevention and treatment of disease. This perspective piece highlights the unique role of medical students in catalyzing the incorporation of climate content into the pre-clinical medical school curriculum and provides topics for disseminated curricular integration with the concepts emphasized in the pre-clinical years of medical education.
Introduction
As medical students interrupted in our clerkship year by a global pandemic of zoonotic origins, we were forced to reflect on a rapidly changing clinical landscape. Long before COVID-19, the World Health Organization (WHO) declared climate change the greatest threat to human health in the 21st century. 1 Last year’s Lancet Countdown on Health and Climate Change starkly warned, “Without accelerated intervention, this new era will come to define the health of people at every stage of their lives.” 2 Climate-driven harms to human health and efforts to adapt to climate change are increasingly permeating aspects of patient care—from a clinician’s diagnostic index, to hospital supply chains and infrastructure, to environmental and racial inequities, to ethics and safety. While resonant in the COVID-19 era of health care delivery, these topics have been noticeably absent in medical education.
We and other medical students are distressed by the overwhelming challenges facing our planet and profession in conjunction with the short timeline to reverse course and safeguard human health from climate change. In a 2018 survey of Chinese medical students, nearly 90% agreed that climate change will have serious and negative impacts on human health globally and locally. 3 The daunting challenges that climate change poses to public health are well-documented. 4 Increasingly frequent and severe natural disasters disrupt healthcare, lives, and livelihoods, while more insidious effects of climate change pose risks to nearly every organ system.5,6 These exposures disproportionately harm those already vulnerable because of existing health conditions and those already disadvantaged by structural racism and inequality.
Within our own pre-clinical curriculum, we heard no reference to the threat multiplier climate change represents to the diseases we learn about and will be expected to treat. Where or when, we asked, will we learn the pathophysiology underpinning climate-related exposures and illnesses? How will we recognize and manage the burden of climate-related mental health trauma—on both ourselves and our patients—food-insecure communities, or spread of vector-borne and emerging infectious diseases if we do not learn about these threats? Addressing climate change requires mobilization of doctors and education of medical students to act on structural determinants of health 7 —efforts that students, themselves, are embracing and leading.
Calls for Medical Education to Adapt to Our Climate Reality
A growing number of physicians have called for more robust medical education on the implications of climate change on health.8,9 A 2018 commissioned report of the Accreditation Council for Graduate Medical Education (ACGME) identified “climate-change medicine” as an emerging internal medicine subspecialty by 2035. 10 The American Medical Association (AMA) echoed this position with a June 2019 policy resolution to support “climate change education across the medical education continuum,” starting with undergraduate training. 11 Less than a month later, the United Nations declared a “climate emergency,” and in partnership with over 7000 institutions across 6 continents, committed to strengthening climate change education. 12 In August 2019, the New England Journal of Medicine launched an online “Climate Crisis and Health” hub to help “mobilize the urgent, large-scale climate action required to protect health.” 6
A handful of medical schools have answered these calls by introducing courses in sustainability and climate change. 13 But so far, these courses represent exceptions. In a recent international survey of 160 institutional members of the Global Consortium on Climate Change and Health Education, only 15 respondents represented medical schools. 14 In the United States, “climate change” remains absent from the Association of American Medical College’s (AAMC’s) Curriculum Inventory topic list of required and elective courses. 15 The reality of current medical education does not reflect the vocal calls of medical professional societies for climate action.
Medical Students: Future Doctors and Current Climate Leaders
As future front-line workers in the climate crisis, students are uniquely positioned to advocate training in climate change and medicine. Recognizing a gap in our own pre-clinical education, we proposed a disseminated “Climate Change & Environmental Health” curriculum for the pre-clinical years at our medical school that has been endorsed by our Executive Curriculum Committee. We are now working alongside the director of the pre-clinical years curriculum and individual faculty to implement the proposal for current first year medical students, the class of 2024. While strategies for integration of climate and health content into curricula will vary by institution, our curricular objectives and approach are broadly applicable and potentially replicable at other schools. Our lessons learned may empower our fellow students to lead integration of climate and health education at their institutions.
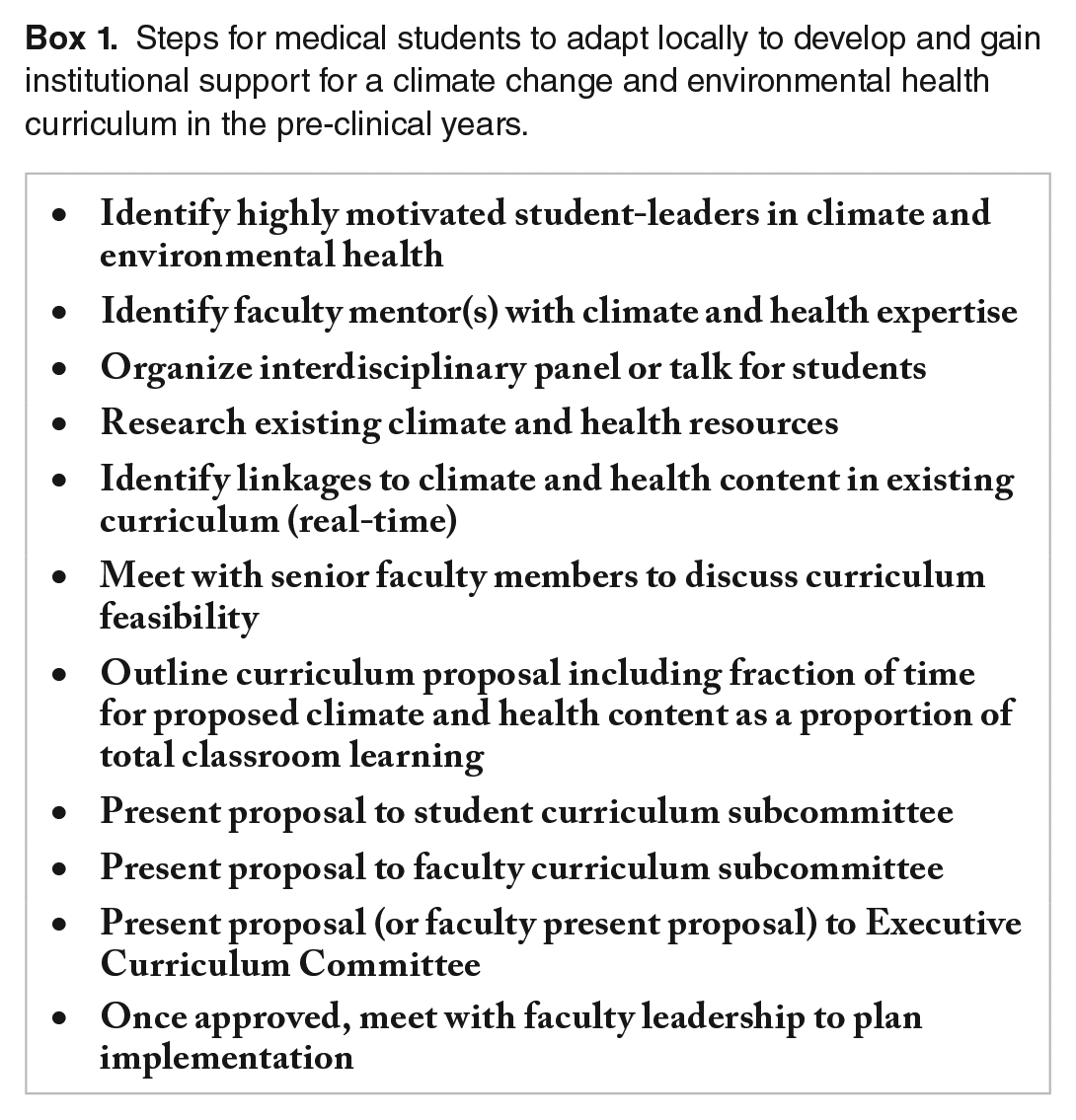
Our engagement with climate and medicine began by forging partnerships with other students highly motivated to lead change and identifying a faculty mentor with expertise in climate and health (Box 1). Galvanized by our mentor’s early support, we organized a lunchtime interdisciplinary panel on Climate and Health at the School of Medicine. The panel discussion revealed enormous enthusiasm and desire for comprehensive teaching on this topic. Inspired to expand the 1 hour-long discussion into a series, we dove further into the existing literature to identify additional topics for discussion. We found that much of what we were already learning in class—like the drivers and dependencies of cardiovascular and renal pathophysiology—are linked to climate change.
Steps for medical students to adapt locally to develop and gain institutional support for a climate change and environmental health curriculum in the pre-clinical years.
We looked for other examples of curricula on climate change in medical education. While workshops abroad have called for environmentally accountable curricula for the medical profession and outlined helpful curricular frameworks, suggested learning objectives provide broad themes rather than specific linkages of climate change to healthy human physiology and disease emphasized in the first 2 years of medical school. 16 We pored through our pre-clinical curriculum to identify critical dependencies between climate change and human health. Through this organic, real-time process, we gleaned relevant topics of pathophysiology to contextualize and reinforce with the most fundamental concepts within climate and health literature. We theorized that examples of climate and health linkages in every module, however brief, would both justify our request to include this content and give students the foundation to engage the growing evidence-base on the impacts of climate change on human health toward life-long learning. We sought feedback from our mentor and engaged key administrators and faculty to refine our curriculum. We knew real-time, first-hand opportunities for incorporating climate content, while school leadership understood the resources and approaches to make our curriculum feasible.
A Disseminated Model Replicable in All Medical Schools
Our process resulted in a disseminated curricular plan of climate and health content with proposed learning objectives dispersed across numerous subjects within the pre-clinical years (Table 1). The objectives of our curriculum are 2-fold: to educate students on the links between climate change and health as they relate to pathophysiology in the pre-clinical years of medical school, with particular emphasis on the disproportionate burden on under-resourced communities; and to prepare students to address the root causes of the problem by focusing on structural inequities and the healthcare system’s carbon footprint. The content throughout the pre-clinical years provides a scaffold for medical students to understand how local and global climate trends—combined with the built and natural environment—affect health and wellness. The curriculum provides a knowledge base on which to build in the clinical years and beyond.
Climate and health learning objectives for preclinical medical education: linked to existing content.

Lessons Learned: Making the Case for a Disseminated Climate Curriculum
The idea of students and clinicians learning from each other towards teaching sustainability in medicine and further securing transformation to sustainable healthcare has shown promise abroad. 17 In our experience, this approach supports timely integration of training for future doctors about climate change—and climate as a determinate of health—in the United States as well. This collaborative creation of curricular content models the interdisciplinary engagement necessary to address the complexities of climate change in medicine, inspires and empowers trainees to lead within an evolving clinical space that will define our careers, and supports urgent, adaptive, institutional change.
We anticipated that the biggest barrier to our curriculum would not be lack of concern about climate change or undervaluation of its impact on health, social justice, and healthcare delivery, but rather, the logistics of adding anything to an already tight curriculum at a time when administrators are aiming to reduce overall classroom time. To preempt concerns around time constraints, we quantified the time this curriculum would add to overall classroom learning. An introductory lecture on climate and health and another lecture related to nutrition would add 2 hours of learning, but the bulk of our content could be condensed into a slide or 2 for a given topic. We calculated the projected amount of time our curriculum would include as a proportion of the total hours of pre-clinical teaching. Our proposal would amount to less than 0.2% of total curricular time.
Members of both the faculty and student curriculum committees initially suggested an elective for second or fourth-year students as an alternative to our disseminated proposal. Their approach would mirror the output of several medical schools offering climate and health electives to students. 18 However, there are inherent deficits of an elective model. An elective is by definition self-selecting and exclusive: students with significant knowledge deficits in the subject area may miss the opportunity to gain critical education. An elective would also signal to students that the implications of climate change on health are non-essential content rather than critical knowledge for every physician—a message that undermines the educational mobilization required at this moment. A disseminated program guarantees all students exposure to climate and health education, while laying a foundation for future learning, and ultimately was endorsed by our Executive Curriculum Committee.
Implementation Opportunities and Challenges
Once our curriculum was approved, we were surprised to receive encouragement from faculty to transpose content from lectures to small group learning—a space we presumed least flexible for curricular additions. Faculty preferred small groups for their ability to foster dialogue, critical thinking and active learning in comparison with lectures. We hope these may further undergird our aim for co-production of knowledge. In a small group on environmental racism, for example, students may ask questions probing the health impacts of the built environment or the disproportionate toll of air pollution on communities of color. Case-based learning also offers flexibility for study of climate change and environmental exposure pathways that affect health. In a session during the renal module, students may learn aspects of heat stress nephropathy: knowledge toward creation of a plan of care with an at-risk patient on rehydration and limiting heat exposure. We hope that by providing space for these conversations, the curriculum will inspire more students and faculty to collaborate and pursue climate solutions.
Many challenges remain. The abrupt transition to virtual learning during the COVID-19 pandemic has presented unexpected hurdles for lecturers adapting their teaching modalities and concerned about student screen fatigue and students unaccustomed to learning from home. Despite these obstacles, in the first weeks of medical school, all first years participated in a virtual, interactive lecture, “Introduction to Climate Change and the Practice of Medicine.” We continue to employ a co-production of knowledge framework as we work with faculty to hone and incorporate content in a step-wise fashion, starting with early modules where strong links exist between existing content and our learning objectives. We know that the curriculum will evolve and that its long-term success depends on buy-in from the many faculty members involved in teaching medical students. The curriculum also requires engagement by some medical students wary of embracing a topic beyond the scope of United States Medical Licensing Examinations (USMLE)—at least unless and until USMLE includes climate change content. However, our experience demonstrates how students can partner with their institutions to win support for educating future doctors on climate and health in keeping with the policy statement of AMA and others.
COVID-19 has underscored the challenges of healthcare delivery and medical education in a time of global pandemic. Economic and public health recovery amidst the climate crisis demands urgent, collective mobilization toward decarbonizing industries—including healthcare—and rebuilding our economy as environmentally sustainable and supportive of human health. To prepare for future challenges in medicine and healthcare delivery, we cannot delay teaching medical students about climate change and health. This disseminated climate curriculum will benefit students and, above all, the patients and communities we serve.
Footnotes
Acknowledgements
The authors would like to thank Dr Mary Jo Lechowicz for encouraging us to continue our pursuit, Drs Erica Brownfield, Jason S Schneider, Mark Mullins, and others on the Executive Curriculum Committee for making the curriculum a reality, Dr David Schulman for his support in the implementation phase of this effort, and Dr Hughes Evans for providing insight and feedback on the paper.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was published with support from Emory Libraries’ Open Access Publishing Fund.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ Contributions
Authors BMR and EBL led this curriculum design effort. RPP provided technical expertise throughout the curriculum design process. All authors contributed to the drafting, editing, and reviewing of this paper. No financial disclosures were reported by the authors of this paper.