
Abstract
OBJECTIVE
To increase the knowledge and communication skills of health professionals related to climate change and human health (CCHH).
METHODS
From February to April 2021, Project ECHO (Extension for Community Healthcare Outcomes) created an 8-week, synchronous and virtual, CCHH ECHO telementoring series for health professionals. Didactics, simulated cases, and climate change tools were used to educate the interprofessional group of participants.
RESULTS
During this CCHH ECHO pilot series, 625 unique participants represented 45 US states and 25 countries. The participants reported that they increased their knowledge, skills, and communication techniques regarding climate change and health.
CONCLUSIONS
The human health effects of climate change is an emerging field, and increasing knowledge and communication skills among health practitioners is of critical importance. The CCHH ECHO is one potential platform that may reach a diverse community of health professionals globally due to the diffusion and demonopolization of knowledge.
Introduction
Scientists are convinced that greenhouse gas emissions are causing our world to warm at an unusually rapid rate, resulting in climatic changes and extreme weather events.1,2 In a recent United Nations poll of 50 countries, over 65% of one million respondents agreed that climate change is a global threat. 3 Extreme heat, drought, extreme precipitation, air pollution, wildfires, and sea level rise are among the climate-related changes potentially affecting morbidity and mortality, especially for low-income residents with underlying health conditions. 4
Health professionals are among the most trusted sources of scientific information and represent a critical voice to raise awareness regarding the health impacts of climate change.5,7 Many medical, nursing, and public health organizations recognize climate change as a global health crisis and endorse the need for climate change and health education.8,16 There are increased calls for nursing education related to climate change, climate justice, and climate action. 17 Similarly, there is now deliberate development of a framework for climate change competencies for community and other public health workers, one of the largest groups of healthcare workers worldwide. 18 In a recent survey of 2817 medical schools in 112 countries, less than 15% incorporated climate change and health into their curriculum. 19
Although health professionals are interested in learning about the congruence of climate change and human health (CCHH), they often lack the time and resources to increase their knowledge and capacity to address these issues. 7 Most receive little prelicensure training in communication skills.20,21 To gain expertise in having difficult conversations, some health professionals have participated in “Breaking Bad News” trainings. 22 However, few are trained to communicate sensitively about topics such as gun safety, suicide, intimate partner violence, and immunization safety, which impact both individual and community health. 23 Now health professionals are strongly encouraged to communicate about weather-related disaster preparedness and health adaptations due to climate change as these topics affect the health of the individual, the community, and the future of the planet. 24
Project ECHO (Extension for Community Healthcare Outcomes) is a peer-learning network for health professionals. In February 2021, University of New Mexico's Project ECHO launched a CCHH program for training postlicensure health professionals. The goals of the CCHH ECHO were 3-fold: to increase health professionals’ (1) knowledge, (2) self-efficacy, and (3) communication skills related to human health impacts of climate change. Evaluation of this program can help to inform effective strategies for preparing health professionals to understand and communicate the impacts of climate change.
Methods
The ECHO model
Project ECHO, launched in 2003, was designed to increase the capacity of health professionals working in rural and urban underserved areas to provide better care to their patients and communities where they live. 25 ECHO is a virtual and synchronous learning program that freely shares up-to-date best practices using case-based learning with the goal to improve lives around the world. Today, the ECHO model is being used by more than 536 partners in 48 US states and 44 countries to address urgent public health challenges, such as substance use disorder, chronic pain, diabetes, and autism. 26 An estimated 461 310 health professionals, public health experts, teachers, and other professionals have received training and mentorship through the ECHO model globally. 27
The ECHO model is a cost-effective method for providing ongoing training and mentorship for frontline health professionals. 28 In ECHO programs, interprofessional experts (the “hub”) connect with community-based or local members of a given workforce (the “spokes”) to learn from and with one another. All knowledge is demonopolized and shared at no-cost. 29 A plethora of research has demonstrated that the ECHO Model is successful at bringing significant practice change to the participant health professional's worksite to improve patient care.30,31
CCHH ECHO series
The CCHH ECHO Series consisted of one cohort, meeting weekly for 75 min, via a virtual and synchronous platform. The weekly sessions were open to all health professionals (physicians, nurses, public health professionals, community health workers, etc). Each session consisted of 2 brief (15-25 min) evidence-based didactic lectures, including moderated question and answer sessions. In 5 of the sessions, a simulated case was also included to match the session's content and illustrate the relationship between climate change and health. Project ECHO's staff entered evidence-based journal articles and other pertinent information into the online platform chat box that the subject matter experts discussed during the session presentations. Participants were offered an “opt-in” community of practice directory at the end of the course, receiving the name and contact information for other participants. Course presentation slides, video recordings, and digital librarian resources were also made available each week to the participants on the Project ECHO CCHH webpage. No-cost continuing education units (CEU) were provided for each session. Course participants also received a certificate of completion if they attended 75% of the sessions (6 out of 8) in the series.
Attendance and registration
Participants registered prior to the program via an online survey (REDCap secure web application) and provided demographic information (gender, age, race/ethnicity, location, and scope of practice). Attendance data were tracked using reports generated by the Zoom platform. Unique attendees were defined as people who attended at least once and for at least 10 min. Registration and attendance data were linked together using name and email. Geographic information was mapped using QGIS Version 3.18.3 and natural breaks, using the Jenks method, were used.
Zoom poll
Beginning week 4 of the CCHH ECHO, participants were polled during sessions to gauge their confidence and understanding. Questions were designed to assess participants’ self-reported knowledge change, and included: “Today's session increased my understanding of the role climate change plays in water- and vector-borne diseases,” “Today's session increased my confidence in my ability to talk to others about the mental health effects of our changing climate,” and “I feel more confident in discussing the human health effects of climate change with my patients and others.” Response options ranged from strongly agree to strongly disagree.
Postsession evaluation
Following each session, participants were invited to complete a postsession evaluation survey, linked to the acquisition of CEUs. Questions included whether the objectives of the course were met, the content was evidence-based, and if participants were able to ask questions to the SMEs. Additionally, participants were asked if they are likely to use the knowledge they gained and if they felt they were better able to communicate after the training. Response options ranged from strongly agree to strongly disagree. Lastly, participants were asked (in a free text field) what changes they might consider making to their practice after the training. These responses were grouped into broad categories (eg, improve my health education techniques; increase my climate change education to my patients, etc). The 7 most common response categories are reported.
Curriculum development: evidence-based didactics
The 8-week curriculum was developed by Joanna Katzman, MD, MSPH, Director of Public Health Initiatives, ECHO Institute, and David Herring, MA, Chief of the Communication and Education Division within the National Oceanic and Atmospheric Association's (NOAA) Climate Program Office. The Co-Chairs of the US Global Change Research Program's Interagency Working Group on Climate Change and Human Health (CCHHG) gave input and feedback on the curriculum. 32 Learning objectives for each week were created by answering the questions: (1) What is the science of climate change?, (2) How does climate change impact human health: biopsychosocially and with vulnerable populations?, (3) What are the most common climate-related health risks and how are they best managed?, (4) What are the current best adaptation practices related to extreme weather events and disaster preparedness?, and (5) How can health professionals improve communication with their patients and communities regarding climate change and health?
This introductory course gave health professionals a better understanding of each of these subjects, while suggesting to them that to gain expertise, the complexity, skill, and knowledge associated with each topic will require more study and practice.
Curriculum development
Case-based learning using standardized patients
Using the successes of medical simulation and standardized patients, 5 patient cases were developed as an integral part of the curriculum to both illustrate the importance of climate change communication and to share climate messaging strategies. Dr Katzman (the CCHH ECHO medical director) collaborated very closely with the medical simulation lead at the University of California, San Diego, John-Michael Maury (JMM). After Dr Katzman created the 5 simulated patient cases, JMM worked with 5 different professional actors to play the standardized patients. A mock session between one of the hub team members (portraying the clinician) and the actor (portraying the standardized patient) took place virtually the week prior to the live CCHH ECHO session. During the CCHH ECHO, the standardized patient/actor connected to the session as the ECHO patient in “full character.” The ECHO IT team spotlighted both the standardized patient and the clinician to fully engage the course participants.
Simulation has been defined as “a model of a set of problems that can be used to teach someone how to do something.” 33 Most postlicensure health professionals learn optimally and develop self-efficacy from iterative presentations of content and case-based learning. 34 The course participants in the CCHH ECHO benefitted from both didactics and cases, with ample time to ask questions. Cases were also developed to illustrate the diversity (people experiencing homelessness, rural and urban, range of ethnicities, gender and ages, etc) of patients seeking care for various climate related illnesses, and to model communication strategies that health professionals might consider when approaching a patient suffering from an illness provoked or worsened by the climate. Because the hallmark of the ECHO model is clinician to clinician telementoring with case-consultation, and patients are not part of the network, medical simulation with standardized patients comes very close to teaching best practices communication strategies with the Project ECHO platform.
Results
Curriculum
To meet the learning objectives, the 8-week series began with introductory presentations on the science of climate change and the gaps in climate change education and communication in the health professions (see Table 1). The second week connected climate change to human health outcomes, including global warming, extreme heat, and vulnerable populations. Weeks 3 through 7 addressed air quality, excessive precipitation, water- and vector-borne disease, mental health, extreme weather events, and disaster preparedness. Week 8 focused on the importance of climate communication and future solutions, including health professional advocacy and policy involvement. The rich contextual experience offered in this introductory course followed the educational principles and guidance provided by health and science, technology, engineering and math educators. 35
Climate change and human health ECHO-series 1 presentations and simulated cases.

Demographics and attendance
During the 8-week CCHH ECHO series, there was a total of 1838 attendances with 625 unique participants (see Table 2). There was an average of 230 nonunique and 78 unique attendees joining each session. Nearly 7% of participants attended all 8 sessions and a total of 41.5% of participants attended regularly (3-8 sessions). Four hundred fifty-two (72.3%) of these attendees had submitted registration information and the majority of participants were women. Over half the participants were white, while almost 14% of participants were Hispanic. Nearly half of the participants had terminal degrees (MD, DO, or PhD) and participants were from around the globe, with 25 countries represented (see Figure 1). The majority of participants hailed from 45 of the US states, most commonly New Mexico (95), where the program is located, along with Western and Northwestern states including California (21), Oregon (29), Washington (10) and Colorado (10); Southern states of Texas (15) and Louisiana (12); and Northeastern states such as Connecticut (14), Maryland (17) and Virginia (12). Roughly 13% (58) of participants resided in countries outside the United States, most commonly from Canada (13), Austria (4), Argentina (4), Peru (4), and Saint Kitts (4).

Climate change and human health ECHO attendance by United State (a) and country (b) among attendees with registration information, February 17, 2021 through April 7, 2021, N = 452.
Climate change and human health ECHO attendance and characteristics, February 17, 2021 through April 7, 2021.

Certificate of completion
The CCHH ECHO course offered a certificate for participants who completed at least 75% (6 out of 8 sessions) of the course. Almost 17% (106 of the 625 unique attendees) completed at least 6 of the CCHH ECHO sessions and within 1 week of the course completion, each of these participants was sent a Certificate of Completion.
Postsession evaluation
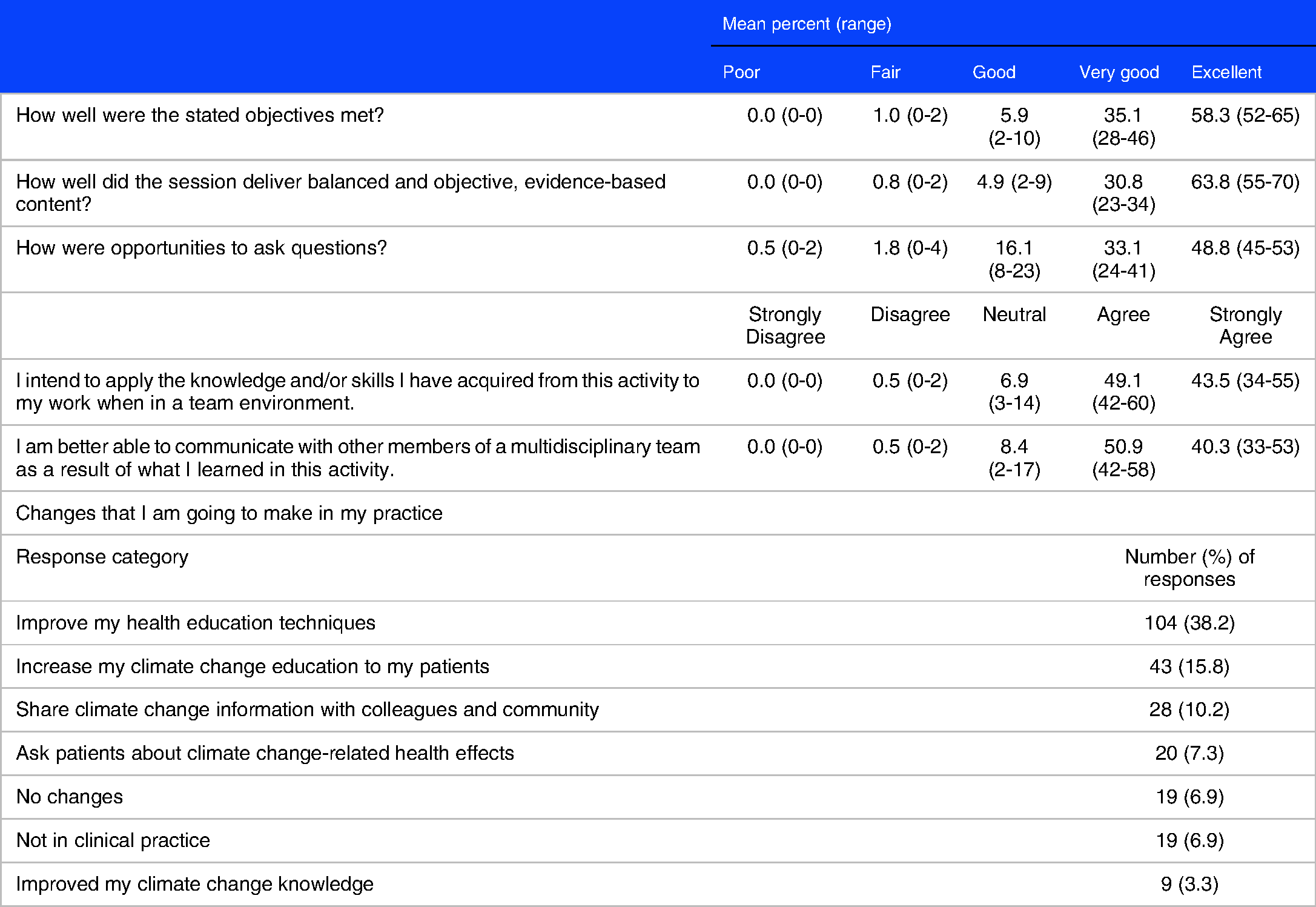
The number of responses to the postsession evaluation each week ranged from 50 (78%) to 66 (85%) respondents out of an average of 78 unique attendees per session (see Table 3). The large majority of survey respondents reported that the objectives of the training were met and that the sessions delivered balanced, objective, and evidence-based content, and rated opportunities to ask questions as very good or excellent. Additionally, participants reported that they intended to apply the knowledge they acquired and that they were better able to communicate with other interprofessional team members. The most common practice change reported was that participants used skills they learned to improve their climate-related health discussions with patients.
Climate change and human health ECHO postsession evaluation responses, February 17, 2021 to April 7, 2021, mean N = 58.6.
Zoom polls
An average of 123.3 (range: 114-137) participants responded to the polls during weeks 4 through 8. Over 90% of participants reported that they strongly agreed or agreed that the sessions increased their understanding of or confidence in each session's topic (see Figure 2). The session on water- and vector-borne diseases and climate change had the highest number of participants reporting that they strongly agreed that the session increased their understanding. Participants were more likely to report that they agreed (rather than strongly agreed) that their confidence increased in all of the Zoom poll sessions. Only in the first 2 weeks of the polls did some of the participants (less than 10) respond that they strongly disagreed. Beginning in week 6, the course facilitator explained the answer key format before the zoom poll began and there were no longer any “Strongly Disagree” responses.

Climate change and human health ECHO zoom polls, weeks 4 to 8.
Community of practice opt-in directory
A Community of Practice Opt-In Directory was offered to all participants in week 3 of the CCHH ECHO. Participants were given the opportunity to stay connected with fellow participants after the CCHH ECHO session by filling out a confidential survey listing their name, email address, and optional cellular telephone number. During the last week of the CCHH ECHO, 55 participants (8% of 625 unique participants) who signed up for this directory were sent information to their ECHO classmates as a method to connect with one another after the course.
Discussion
Success of the CCHH ECHO
This CCHH ECHO series proved to be highly satisfying for the vast majority of health professionals who participated in the 8-week series. Strengths of the CCHH ECHO include: (1) the large number of unique participants returning each week from throughout the United States and abroad, (2) the bi-directional, moderated question/answer sessions, (3) the simulated clinical climate change cases, (4) the course certificate and community of practice options, and (5) the benefits of a digital librarian. Some health professionals also identified areas of improvement for this CCHH ECHO series. Suggestions included: allowing more time for questions/answers, adding didactic presentations on climate and mental health, sustainability and climate justice.
The ECHO model: diffusion of knowledge, capacity building, and community of practice
The postsession evaluations and zoom polls suggest that the goals of this 8-week CCHH ECHO series (increasing health participant knowledge, confidence, and communication) were successfully achieved. In light of the current climate emergency, the ECHO Model is an invaluable platform for demonopolization and effective diffusion of evidence-based knowledge to build capacity among professionals, patients, and communities. The ECHO Model also has a strong history of developing communities of practice and reducing feelings of isolation among many health professionals. 27 This may benefit health professionals seeking to expand their engagement with communities and organizations addressing the health impacts of climate change.
Demographics and geographic distribution
The majority of participants were women, which is not surprising considering that women are slightly more likely to be concerned about the environment compared to men. 36 In terms of race and ethnicity, Hispanics/Latinos and African Americans are more likely to be alarmed about climate change than Whites, however the majority of participants in this CCHH ECHO were white. 37 This may be reflective of the racial/ethnic distribution of the healthcare field.
It is also possible that course participants, who reside in jurisdictions (West/Northwest and Southeast) which have acutely been affected by extreme weather events (wildfires and extreme precipitation), are participating in this course in larger numbers.
Curriculum: evidence-based didactics and case-based learning
The CCHH ECHO curriculum deliberately included both broad and more narrowly focused elements critical for health professionals to best understand the relationship between CCHH. The postsession survey and Zoom poll results suggest that the majority of participants increased their knowledge and confidence in the topics presented. They also reported that they plan to change their practice based on the information learned in the CCHH ECHO sessions. Specifically, they plan to communicate more with their patients, applying the knowledge they have learned and the tools they have gained.
Live simulated cases between a health professional and a standardized patient were part of 5 of the sessions. There are many benefits to simulation including “practice of complex clinical situations; rehearsal of serious and⁄or rare events; rehearsal of planned, novel or infrequent interventions; and induction into new clinical environments.” 37 Use of simulation with standardized patients or public health scenarios reduces risks to patients, communities, and learners. Educationally, simulation supports principles of active learning, safe application of knowledge and skills, and opportunity for iterative practice with feedback, incorporating evidence-based knowledge within each case or scenario.38,39
The advantages of using simulated cases for the CCHH ECHO are numerous. The cases: (1) can be adjusted for different types and levels of health professionals, (2) can be modified to educate health professionals regarding how to approach patients with varying levels of climate change knowledge and belief, (3) can be shifted to benefit the specific geographic region and culture of the population affected, and (4) the cases can be recorded and used for future training sessions. 29
Most ECHO programs include course participants sharing real, de-identified patient cases. Therefore, creating simulated cases for the CCHH ECHO is a novel adaptation of ECHO's successful case-based learning approach. Because patients do not join ECHO sessions, the use of simulated cases allows for climate change cases to be developed for a variety of health professionals as well as diverse, rural, underserved, and disproportionately impacted populations globally. Project ECHO has used simulated learning for many years in their MOCK ECHO trainings, whereby health professionals can practice their skills repeatedly in a safe environment before they launch a live ECHO session. 40
There are many other complementary climate change educational offerings for health professionals. These include a growing number of evidence-based, peer-reviewed climate change, and environmental journal articles, webinars from NOAA, CDC, the Medical Consortium on Climate and Health, Physicians for Social Responsibility and other highly regarded organizations, as well as other academic medical centers providing postlicensure trainings.41,46
Scaling up and moving forward
Due to the success of the 8-week CCHH ECHO series, the authors decided to launch a weekly 60 min CCHH ECHO “Continuous Conversation Office Hours,” beginning in August 18, 2021. Changes to the original format include shortening each session to 60 min, allowing more time for questions and answers, and planning for presentations on mental health, climate justice and environmental stewardship. The authors are also planning to begin a similar program in India, in addition to an 8 to 10 week “train the trainer” program, so that highly motivated health professionals may deliver a climate change course at their own institution.
Conclusions
Because the ECHO model is capacity-building, low-cost, and easy to deploy, the CCHH ECHO has the potential to reach many thousands of people globally due to the diffusion of knowledge between patients, colleagues, and communities. The human health effects of climate change is a necessarily emerging field, and increasing knowledge and communication skills among health practitioners is of critical importance. Given the climate crisis, a robust climate and health curriculum is needed in both pre and postlicensure settings for all health professionals. Future CCHH ECHO telementoring programs may explore avenues to equip health professionals with the competencies needed to teach climate-related health effects at their own public health programs and healthcare institutions.
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Footnotes
Acknowledgments
The authors would like to thank the Centers for Disease Control and Prevention for review of the manuscript. The authors are grateful to Kent Norsworthy, our Project ECHO digital librarian, to Shalin Prabhat Luitel, BA, BS at Project ECHO, for creating the maps for the manuscript, and to Hunter Jones, PhD from the National Oceanic Atmospheric Association for his thoughtful consultation.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
JGK created the idea for the program and the evaluation; JGK, DH, PH, LT, JMM developed the curriculum and evaluation; LT, JL, BKD, JGK collected and analyzed the data; JGK, DH, PS, LT, SK, CM, SA wrote and edited the article; JMM, BKD, JL edited the article.