
Abstract
Introduction:
Recently, participation in clinical global health rotations has significantly increased among graduate medical education (GME) trainees. Despite the many benefits these experiences provide, many ethical challenges exist. Well-intentioned partnerships and participants often encounter personal and professional dilemmas related to safety, social responsibility, and accountability. We designed a curriculum to provide trainees of all specialties with a comprehensive educational program aimed at delivering culturally mindful and ethically responsible clinical care in resource-constrained settings.
Methods:
The McGaw Global Health Clinical Scholars Program (GHCS) at Northwestern University offers a 2-year curriculum for selected GME trainees across specialties interested in global health. Each trainee must complete the following components: core lectures, peer journal club, specialty-specific lectures, a mentorship agreement, ethics and skill-based simulations, a global health field experience, a poster presentation, and a mentored scholarly project.
Results:
Since 2014, 84 trainees from 13 specialties have participated in the program with 50 current trainees and 39 graduates. Twenty-five trainees completed exit surveys, of which 95% would recommend this program to other trainees and 84% felt more prepared to deliver global health care. In addition, 78% reported career plans that included global health and/or work with underserved populations. Trainees described “acceptance of differences and respect for those differences” and “understanding sustainability” as learning points from the program.
Discussion:
Providing a comprehensive global health education program across specialties can be feasible and effective. GME trainees who participated in this program report feeling both more prepared for clinical experiences and more likely to serve the underserved anywhere.
Introduction
Over the last few decades, American medical trainees and professionals at varying levels of clinical training have expressed a growing interest in global health. 1 With increasing international travel and globalization, physicians and those in training have acknowledged a need for better understanding of global health systems, the global burden of disease and ways to address health disparities between systems. Academic institutions have responded to this interest and a large majority of medical schools and GME programs across the United States offer trainees opportunities to travel abroad and participate in short term experiences in global health (STEGH) and more and more programs include some form of global health teaching or training along with these rotations. 2 Furthermore, an increasing amount of American academic institutions have partnered with foreign institutions to provide educational exchanges and funding.3,4
An AAMC survey in 2010 showed that 30.2% of graduating medical students have participated in these activities. 1 Upon entering residency, numerous studies have shown that global health interest remains high and often influences trainees’ selection of a training program. 5 Offerings of global health education during residency and fellowship have historically been available to those training in primary care specialties (family medicine, primary care internal medicine, and pediatrics) but are now increasingly available for trainees of all specialties. 6 In a survey of ophthalmology residency programs in 2012, 54% of programs reported offering a global health elective.7,8 Additionally, a survey of plastic surgery residency programs in 2015 showed that 64% of programs sponsored resident participation in global health missions.7,9 Despite the growing availability of STEGH opportunities in GME training, trainees continue to voice more and more interest and desire for further and structured programs. 2 A 2007 survey of surgical residents revealed that 98% were interested in an international elective and 73% would prioritize this over any other elective. 10 In 2010, 91% of surveyed anesthesiology residents reported interest in global health as well as 72% of radiology residents, further showing that interest is persistent and prevalent across specialties.7,11,12
When participating in an international elective, trainees often encounter a new culture and medical system and are exposed to different and often unfamiliar methods of diagnosis, treatment, and interactions with patients and caregivers. The benefits of these international electives have been well-established and reported by trainees themselves. 13 Trainee STEGH participants have noted improved confidence in clinical skills, less dependence on technology, an increased awareness of cost, and an appreciation of public health and preventative medicine. 14 These benefits are thought to improve not only the individual trainee but the U.S. health system as a whole given that those who participate in international rotations are more likely to choose primary care specialties, work with underserved populations and opt for public health degrees.2,13
Despite these many benefits, many concerns have been raised about the risks of undertaking global health rotations without the preparation one would typically have when approaching a novel clinical setting. Without thoughtful planning and education, global health rotations can lead to ethical issues that negatively affect the host institution, local health professionals and trainees, the rotating trainee, patients as well as local communities. 15 Unbalanced partnerships can lead to undue burden on the local system and raise concerns about exploitation and sustainability. 16 Visiting trainees may feel compelled or be asked to practice outside their scope of practice or with minimal supervision causing significant harm to patients, who may be unaware of their individual expertise particularly in a new context. 17 Returning trainees have also reported feeling inadequately prepared to handle the ethical dilemmas encountered during these experiences. 18 Numerous initiatives have been launched to respond to these concerns and establish consensus on ethical guidelines for global health partnerships and rotations. Nearly a decade ago, The Working Group on Ethics Guidelines for Global Health Training (WEIGHT) collectively agreed upon the key components of global health partnerships including: the importance of structured programs between partners, reciprocal and mutual benefit, comprehensive accounting of cost, the value of long term partnerships, selection of suitable trainees, adequate mentorship and supervision of trainees, preparation of trainees, trainee safety, appropriate trainee attitudes and behaviors. 19 Since then global health competencies have been proposed as well as multiple best practice guidelines for both the structure of STEGH at the institutional level and for individual trainees.20-23 Multiple individual institutions have also created pre-departure trainings that are open to other institutions and better prepare trainees for these experiences including the American Medical Student Association, edX through Boston University, Unite for Sight, Child Family Health International, and Aperian Global.24-28
In addition to addressing these ethical challenges, creating and operationalizing a global health training program for graduate medical trainees can be a truly formidable task. GME residents and fellows have substantial workloads with significant time constraints and mandatory program requirements to complete training, which are particularly applicable to those in the surgical specialties (Obstetrics and Gynecology, Anesthesia, Surgery, and surgical subspecialties). 29 Furthermore, given the constant acquisition of new skills and evolving independence, defining scope of practice during global health rotations is a common ethical dilemma faced by GME residents and fellows. Finally, the individualized objectives, needs and partnerships across specialties vary significantly and can lead to global health education within an institution feeling disjointed. At our institution, the Center for Global Health which is now the Institute for Global Health and will be referred to as IGH, already existed and offered support to global health faculty and interested GME trainees looking for mentorship and international rotations. However, there was not a structured path for GME trainees to designate themselves as interested in global health, obtain formalized mentorship and education around these rotations or be exposed to intentional opportunities for collaboration and careers in global health. Thus, we designed and implemented a global health clinical scholars program (GHCS) that would fill these many needs and current gaps in standard training. We combine a standardized educational curriculum for GME residents and fellows across all specialties to prioritizes institutional unity, collaboration and consensus in our approach to global health education with individualized specialty-specific teaching and mentorship for trainees to be successful within their interest area. The global health rotations themselves are offered through their training departments however our program aims to create an educational scaffolding around these STEGHs. The core curriculum is focused on teaching trainees how to provide culturally respectful and ethically responsible care in resource constrained settings.
Methods
Curriculum development
We used a modified Kern’s methodology to develop our curriculum and focused on identifying the problem/general needs assessment, targeted needs assessment, goals and objectives, educational strategies, implementation and evaluation, and feedback. 20 As an initial needs assessment, internal medicine residents participated in a 2-part survey that asked who would participate if a global health opportunity were available. Of 51 participants, 33% responded yes and 31% responded maybe. We also asked how important they feel global health opportunities are to residency applicants, of which more than 60% responded with moderately or very important. After establishing this general trainee interest, the IGH faculty drafted a preliminary curriculum and conducted 2 rounds of focus group interviews. The curriculum was created based on seminal training texts,21,22 PubMed literature searches, ACGME competencies, and input from professional networks such as the Consortium of Universities for Global Health (CUGH). The first group was a meeting comprised of interested program directors, leaders of GME and IGH faculty who revised the initial draft. Given the many stakeholders involved in creating a curriculum that spans all specialties, institutional alignment, and support for the program was imperative. A second targeted needs assessment was completed and recommendations from a second focus group was used to finalize the curriculum. We ensured that global health competencies were in alignment with GME competencies for each specialty (Figure 1).

Alignment of global health competencies with GME competencies for the GHCS program.
Program structure
A 2 year program is available for all graduate medical trainees (residents and fellows of all specialties) interested in global health whose program partners with the GHCS. Our program staff is composed of a core faculty including a program director (PD), assistant program director (APD), and program assistant. Curriculum development, arrangement, and supervision of partnerships with each specialty, provision of educational opportunities, and general scheduling are the primary roles of this faculty and the program itself. The education program assistant from IGH supports the McGaw GHCS as part of her portfolio in program administration.
A formal partnership agreement with the trainee’s department and our program is required as there are many support and scheduling roles needed to participate. Each individual training program agrees to provide specific lectures, scheduling support including time for the field experience, simulation instruction, and provision of a faculty mentor within the trainees’ department. Once a trainee expresses interest in the program, a formal meeting is held with their program director and potential specialty-specific mentors in order to determine the feasibility of the partnership. Programs are added as partners on a rolling basis. Once part of the program, specialty specific mentors meet together with core faculty every 3 months to discuss progress of mentees, delineation of tasks, and ideas for program change and improvements. The PD receives support from Northwestern GME, the APD and faculty mentors are supported by the Global Health Initiative, an internal global health philanthropic fund.
Applicant selection
A program application and recruitment materials (see Appendix 1) are now sent out to all GME trainees (until 2018, these applications were sent out at the discretion of the residency or fellowship program director). Interested GME trainees complete an application which includes a statement of interest and a formal recommendation from their program director (see Appendix 2). Information sessions for all interested trainees are provided by our program director and for individual programs upon request.
Program components
Once admitted to the program, all trainees are provided with a copy of the following educational objectives which are continually emphasized throughout the duration of the program.
Educational objectives
Describe the global burden of disease and demonstrate understanding of epidemiologic tools and methods
Understand health implications of travel, migration and trade
Recognize the major determinants of health
Demonstrate a basic understanding of the relationship between health and human rights
Demonstrate high standards of ethical conduct and quality in global healthcare
Explain the role of community-engagement strategies in capacity strengthening
Demonstrate cultural humility and cross culturally effective support to patients
Develop strategies for ethical practice in unfamiliar and resource-constrained settings
Develop a global health focused scholarly work and peer teaching skills
Trainees must then complete the following curricular requirements in order to graduate from the global health scholars program (see Appendix 3). Trainees have 2 years to complete all requirements based on individual schedules though we allow trainees with longer clinical programs, especially those in surgical specialties, to use additional years to complete the program.
Once admitted to the program, all trainees must attend orientation. This time serves as a general introduction to the program and curricular requirements and an opportunity to meet with trainees in other specialties.
These lectures serve to provide a basic foundation in global health and tend to cover broader topics that are pertinent to all specialties (see Figure 1 for complete list of core lectures).
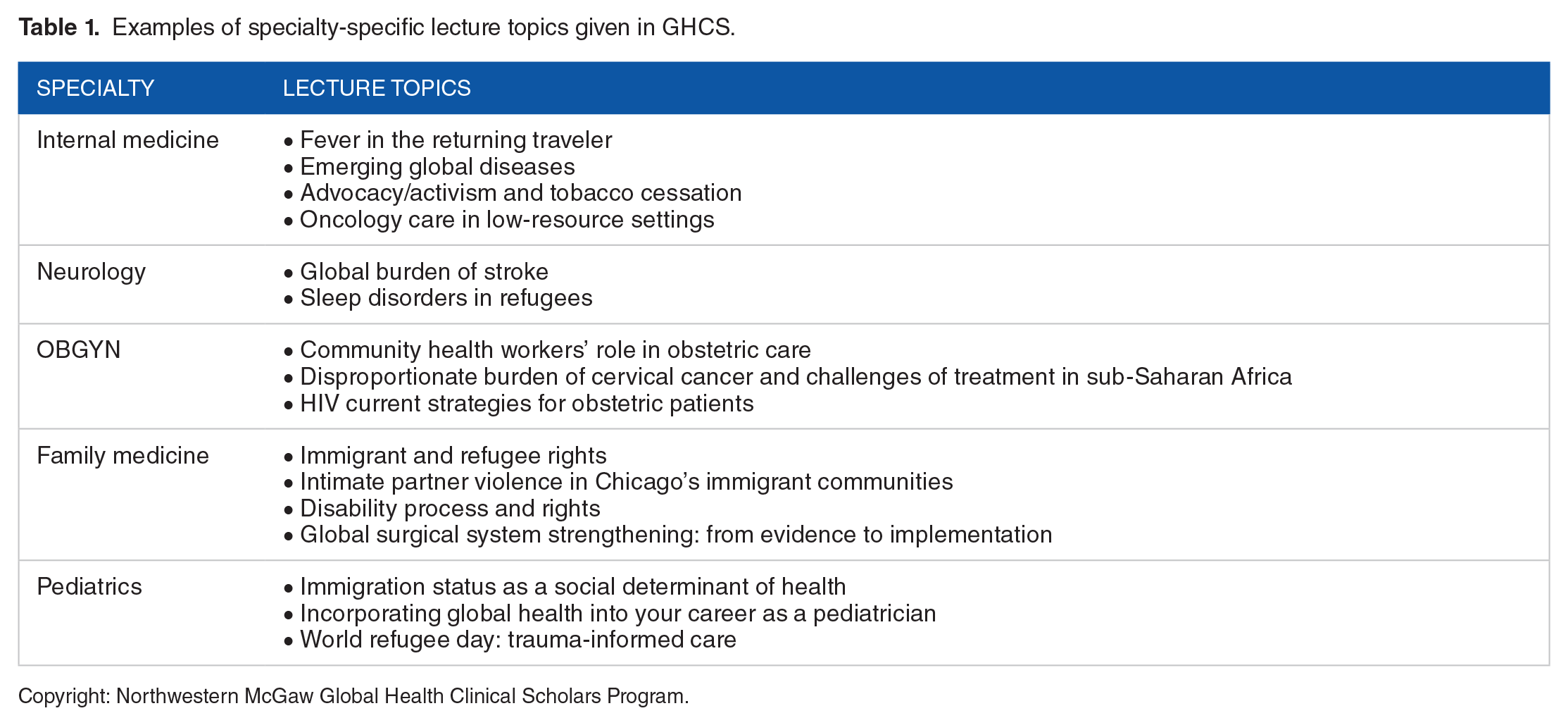
These lectures are organized by the global health mentor and are intended to provide their trainees with global health knowledge specific to their specialty. Of note, all trainees are invited to each other’s specialty-specific lecture series as there are often cross over areas of interest (Table 1).
Examples of specialty-specific lecture topics given in GHCS.
Copyright: Northwestern McGaw Global Health Clinical Scholars Program.
In order to encourage trainees to remain updated on emerging issues in global health and to critically appraise global health literature, trainees from each specialty, either as a group or individual, present a journal article relevant to that specialty. Each trainee must discuss the selection and plan for discussion of the chosen article with their global health mentor prior to presentation. On the day of presentation, the trainee should be prepared to discuss key takeaways, strengths and weaknesses, and relevant discussion questions.
Each trainee is paired with a global health mentor who is a faculty member from their home department. Mentors are expected to use their specialized knowledge in both global health and that particular specialty to support, supervise, and mentor each trainee. Each mentor is provided with a set of expectations and responsibilities (see Appendix 4). Mentors meet with trainees before, during and after each field experience, assist with creation of peer journal clubs, and provide career guidance. Each mentor has no more than 3 mentees at one time in order to provide each trainee with a meaningful relationship. Mentors and mentees are required to sign an agreement stating that both have a mutual understanding of what the mentoring relationship will involve and can agree on action items that should take place. All mentors from all programs meet every 3 months in order to review and revise the program and troubleshoot current issues, discuss upcoming lectures or educational products, receive global health education trainings or resources and discuss trainees and their progress toward graduation requirements.
A detailed description of the Ethics and Skills Simulation Series can be found in Appendix 5 which describes the entire curriculum and contains documents to support implementation.
Trainees complete a 4 to 6 week experience at an approved field site. Our institution has several global health partnerships and different specialties have partnerships that are supervised and arranged by their department at international clinical training sites. Our trainees typically choose a specialty-specific site where there is an existing partnership that is approved by their program director, global health mentor, and finally the GME leadership. Each partnership varies in terms of Memoranda of Understanding, trainee activities, participation, supervision, and support at the site.
Examples of Active International Partnerships include:
Internal Medicine: Hillside Health Care Clinic, Belize; Centro Medico Humberto Parra, Bolivia
Family Medicine: Clínica de Familia La Romana, Dominican Republic; Hillside Health Care Clinic, Belize
Anesthesiology: Hospital Materno Dr. Reynaldo Almanzar, Dominican Republic
General Surgery: Bolivia Trauma Initiative, Bolivia
Pediatrics: Bugando Medical Center, Tanzania
Trainees are required to complete all 3 modules of “The Practitioner’s Guide to Global Health” which is a timeline-based course provided by EdX and Boston University as well as Unite for Sight’s module on Ethics in Photography.25,26 The simulation series, particularly the ethics simulation and nearly all of the core lecture series, also comprise essential pre-departure training.
Trainees are also required to meet with their mentors prior to travel in order to reflect on the content of the pre-departure training modules and discuss the trainee specific objectives of the experience. They can opt to communicate with their mentor during their field experience but are required to debrief with their mentors within 2 weeks of their return. 30
Upon returning from their field experience, trainees are required to complete a scholarly project which should demonstrate understanding of a learning objective relevant to their global field experience. This may include any of the following: poster or abstract presentation, opinion piece, clinical reflection essays, peer-reviewed publications, curriculum development or training materials, literature reviews, educational initiatives for health care workers, research (encouraged only from those participating in year-long research fellowships already), and quality improvement initiatives.
Trainees are asked to present a poster abstract on global health day hosted by the IGH that is relevant to their field experience or global health area of interest. This should also meet one of the aforementioned educational objectives. Trainees have recently presented posters entitled “Seizures in Tuberculous Meningitis in Zambia,” “Birth Tourism: Obstetric and Neonatal Outcomes,” and “Understanding the High Caesarean Section Rate in Egypt: An Exploratory Study.”
Results
2014 to 2015 served as our pilot year in which 3 trainees participated in the program. Trainees were from internal medicine, family medicine, and physical medicine and rehabilitation and formal partnerships were formed with these programs. Since our pilot year, the program has grown to a total of 84 trainees and 13 formal partnerships with residency and fellowship programs. As of 2019, 50 trainees are actively participating in our program. New specialties continue to be added each year and now non-primary care specialties make up the majority of our trainees (see Figures 2 and 3). Our trainees have participated in global field experiences with established partner sites as listed above. A few training programs have established new formal partnerships after approval from their program’s and GME leadership. Some trainees are beginning to create local partnerships with underserved communities in the U.S. as well. Our faculty play an advisory role in these final decisions.

Total participants in GHCS by specialty, 2014 to 2019.

Graduates of GHCS by specialty, 2014 to 2019.
In total, 39 trainees have graduated the program. The 2 trainees who completed all curricular requirements except a field experience received an area of focus designation. There has not been a surgical specialty graduate outside of OBGYN given their longer training programs and propensity to extend participation in the program to fit individualized scheduling needs. Many of our trainees have continued to pursue work with underserved populations both in and outside the United States after graduation. Three trainees have been awarded NIH Fogarty awards, one for cardiovascular health services research and one for paternal roles in OBGYN in Kenya and one for Neurosurgery in Peru (while participating in the program). One of our recently graduated trainees worked as an oncology clinician for Partners in Health in Rwanda. Two are working at federally qualified health centers. One will continue to teach simulation curriculum in Tanzania as part of a faculty appointment and will have a leadership role in global health education at our institution. Many of our trainees are currently pursuing fellowships including additional graduate global health training programs.
In total, 25 exit surveys were completed with 90% agreeing or strongly agreeing when asked if the program added value to training. When asked, if after completing the program, trainees felt more prepared to deliver global health care 84% agree or strongly agree. Eighty percent agree or strongly agree that the program encouraged them to start or continue a career in global health. Ninety-five percent would recommend this program to other trainees. Seventy-five percent will be working with underserved populations, both in and outside the U.S. Trainees reported that, “the combination of didactics, mentorship, resources, and funding provided by the GHCS program unquestionably added to my development as a global health physician-scientist.” Another noted that the program led to “increased awareness of global health, cultural considerations and limitations, resource limited decision making, and provided networking opportunities. The simulation sessions were highly informative and helpful.”
When asked what they learned from the program, one noted, “acceptance of cultural differences and respect for those differences in partnered health decision making” and another said they learned, “ethical considerations, my place in a multinational healthcare team.” In regards to core lectures, some trainees with prior global health experience felt that these were too “basic” for their knowledge base. Other trainees felt that they provided the broad education that they needed.
When asked specifically about their mentors, 96% felt that their mentor met their needs. One commented that “our mentor was always available to us for advice and heavily facilitated our travel and clinical arrangements for our month-long site visit. For our simulation sessions, she was also very helpful and kept us on track and organized. She is an excellent mentor who consistently encouraged us to seek out global health opportunities for our education.” Another wrote “. . .having a scholarly project as part of the requirement made us think more critically about systems improvement and helped make our site visit even more valuable.” Others also noted that “the program allows for interactions with residents and attendings from other specialties who would otherwise potentially never interact with one another.” Another trainee commented, “Had I gone abroad without this program, I would have been unknowingly ill-prepared. The adage ‘you don't know what you don’t know’ comes to mind. I know I will make my share of mistakes in the future while practicing abroad (and stateside) but I will make far less and I believe. . . (do) more good and less harm, because of the global health program.” A few trainees also alluded to the idea of making the program more of a community. One trainee specifically noted, “We do individual debriefing in our program, but I think post-travel discussing what we have done and experienced together would be valuable.” A final and unexpected outcome of creating the global health clinical scholars program was the subsequent development of 3 other scholars programs (bioethics, medical education, and health disparities and equity) 31 at our institution using the structure of our program as a template.
Discussion
Given concerns around and needs for safe and ethical STEGHs, many institutions have recognized both a need to better prepare trainees for these experiences and that trainees interested in careers in global health require dedicated education and professional development which are not traditionally offered in most GME programs. Learning objectives, best practices and frameworks have been established to standardize the ethical principles that should guide trainees’ actions during global health rotations. With these in mind, we aimed to create a general curriculum that could be adopted by graduate medical education programs for trainees across all specialties. We have found that this approach can establish a standardized, mindful and safe approach to clinical global health practices by GME trainees, increase collaboration and promote trainee professional development throughout the institution. We were able to deliver a robust educational curriculum incorporating a variety of instructional strategies and using asynchronous curricula from other platforms like EdX, Unite for Sight which helped to expose trainees to a variety of approaches to the material. Experiential and transformative learning were central to our curriculum with both the field experience and simulation.25,26 Our simulation curriculum provides trainees with high-fidelity, safe, experiential learning with structured debriefing in preparation for challenges they may encounter in their field experience. We also came to recognize the immense value in creating an educational home where trainees interested in global health can receive the support to reach their goals.
There were also several challenges that we encountered when implementing this curriculum. Coordinating schedules, lectures, and simulations across specialties can be incredibly difficult. We held global health faculty meetings every 3 months to improve communication and arrange educational activities. Having a designated program assistant to arrange and disseminate logistics, schedules, and educational materials improved efficiency and offered unified support to trainees and program partners. Trainees in our program also reported struggling to attend required curriculum components due to clinical schedules. In fact, we created this program over 2 years (or more for those with longer clinical programs) in order to have a better chance of attending more events. Trainee feedback about the content of the core lectures reflected the diversity of our learners. Given trainees join the program with differing levels of expertise, it can be difficult to meet all trainees’ needs. We are planning to incorporate a more in-depth lecture schedule especially for second year trainees and those with prior global health experience. We have also found that trainees are interested in learning more about career opportunities and are planning a career development series that will illuminate opportunities in global health related to research, clinical care, advocacy, and work with both governmental and non-governmental organizations. In response to trainees requesting that our program provide a deeper sense of community and collaboration, we are planning to incorporate more shared experiences and platforms for group discussion through videos, small groups, and social events.
Other institutions such as Mount Sinai, University of Virginia and Indiana University have formed global health education programs that also focus on collaboration between specialties and have been designated as collaborative interdisciplinary global health tracks (CIGHTs). These programs have further highlighted the strengths of the multidisciplinary approach including shared allocation of global health resources, consensus on global health education, and consistent mentorship regardless of year-to-year trainee interest. 32 With similar program components (educational activities, international experience, and mentoring etc.), these curriculums are seemingly differentiated in their educational approach with our focus being on learning global health ethics especially through simulation whereas other programs have emphasized participation in bidirectional educational exchanges and public health courses. 32
Although it can be difficult to meet the needs of many different trainees, we have found that creating an educational space for global health trainees and mentors of all specialties is fundamental to a supportive and collaborative learning environment. By establishing a codified set of basic knowledge, attitudes, and professional skills rooted in ethical practice in STEGH, we can begin to prevent unintentional harms, improve patient and trainee safety, support and enable professional development for dedicated trainees and standardize best practices in clinical global health both within our institution and beyond.
Footnotes
Appendix 1
Appendix 2
The McGaw Global Health Clinical Scholars Program offers Northwestern University’s McGaw Graduate Medical trainees (residents and fellows) a 2-year program. Curricular requirements include 10 of 12 core lectures, 5 of 6 specialty lectures, participation in a quarterly professional development and journal club, faculty mentorship, web-based training modules, simulation training, contribution to cross residency skill simulation, global health field experience, and production and presentation of a scholarly project.
Do you believe the applicant would be able to complete the requirements of this certificate program? What would they contribute to the program?
________________________________________________________________________________________________________________________________________________
I have reviewed the McGaw Global Health Clinical Scholars program and am familiar with the above applicant applying for admission. This applicant is in good standing with their program and has demonstrated leadership potential. I believe the above applicant would contribute to the Global Health Community and the academic quality of the program. I hereby recommend this applicant for admission.
Name of Program Director recommending applicant: _____
Title: _____________________________
Signature: __________________ Date: __________________
Please return this form to:
Appendix 3
Global Health Clinical Scholars—Program checklist for graduation. Completion rate.

| # | Check Items |
Descriptions | Checked by (user stamp) | Checked at (time stamp) | Status (double click to |
|---|---|---|---|---|---|
|
|
|
||||
| 1.1 | Orientation | ⎕ | |||
| 1.2 | The History of Global Health & Globalization | ⎕ | |||
| 1.3 | The Global Burden of Disease & Travel Medicine | ⎕ | |||
| 1.4 | Issues & Innovations in Reproductive Health | ⎕ | |||
| 1.5 | Issues & Innovations in Child Health | ⎕ | |||
| 1.6 | Issues and Innovations in Global Surgical Care | ⎕ | |||
| 1.7 | Global Mental Health & Trauma Informed Care | ⎕ | |||
| 1.8 | Immigrant & Refugee Health | ⎕ | |||
| 1.9 | Planetary Health & Climate Change | ⎕ | |||
| 1.10 | Health & Humanitarian Disaster Response | ⎕ | |||
| 1.11 | Implementation Science & Quality Improvement in Global Health | ⎕ | |||
| 1.12 | Global Health & Human Rights | ⎕ | |||
|
|
|
|
|||
| 2.1 | Lecture 1 | ⎕ | |||
| 2.2 | Lecture 2 | ⎕ | |||
| 2.3 | Lecture 3 | ⎕ | |||
| 2.4 | Lecture 4 | ⎕ | |||
| 2.5 | Lecture 5 | ⎕ | |||
|
|
|
|
|||
| 3.1 | Internal Medicine | ⎕ | |||
| 3.2 | Neuro | ⎕ | |||
| 3.3 | OB/GYN | ⎕ | |||
| 3.4 | Peds | ⎕ | |||
| 3.5 | Radiology | ⎕ | |||
| 3.6 | Dermatology | ⎕ | |||
| 3.7 | Anesthesia | ⎕ | |||
| 3.8 | Surgery | ⎕ | |||
|
|
|
|
|||
| 4.1 | GH Practitioner’s Guide 1 | ⎕ | |||
| 4.2 | GH Practitioner’s Guide 2 | ⎕ | |||
| 4.3 | GH Practitioner’s Guide 3 | ⎕ | |||
| 4.4 | Photography and Ethics | ⎕ | |||
|
|
|
|
|||
| 5.1 | Ethics Simulation | ⎕ | |||
| 5.2 | OB/GYN and Pediatrics Simulation | ⎕ | |||
| 5.3 | Surgery/Anesthesiology Simulation | ⎕ | |||
|
|
|
|
|||
| 6.1 | Global Rotation | ⎕ | |||
| 6.2 | Post-Trip Debriefing | ⎕ | |||
|
|
|
|
|||
| 7.1 | Scholarly Project | ⎕ | |||
| 7.2 | Global Healt Day Poster | ⎕ | |||
Appendix 4
Appendix 5
Acknowledgements
The study group acknowledges valuable input from Dr. Elizabeth Groothius, Dr. Mamta Swaroop, Dr. Magdy Milad, and Dr. Feyce Peralta as well as staff support from Sara Caudillo and Elizabeth Nicole Christian. We would also like to express a sincere thank you to Northwestern Graduate Medical Education, McGaw Medical Center of Northwestern University, and the Global Health Initiative.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
Conception and Design: JM, SG, ADP
Collection and Assembly of Data: JM, CF, ADP
Data Analysis and Interpretation: JM, CF, ADP
Manuscript Writing: All Authors