
Abstract
Objective
Augmented reality (AR) is a technology that incorporates digital information into user's physical surroundings. It represents a paradigm shift in medical treatment and education. AR aides in surgical planning and patient therapy, as well as assisting patients in comprehending difficult medical problems. AR is evident in several facets of medicine, and there is a significant need for helping systems as a result of the increasing stress placed on public health systems during pandemics. The use of virtual reality (VR) and AR in surgery, dentistry, telemedicine, self-care, and wellness treatments has already improved many areas of healthcare.
Method
This systematic review adheres to Preferred Reporting Items for Systematic Reviews and Meta-Analysis checklist and was conducted using PubMed and Scopus databases with keywords such as “Augmented Reality (AR),” “Virtual Reality (VR),” “Extended Reality (XR),” “Medical Education,” “Surgical Planning,” “Clinical Training,” and “Patient Therapy.” Boolean operators (AND, OR) were applied, and through a systematic review process, 21 peer-reviewed studies published between 2010 and 2024 were analyzed.
Results
The usage of ARs and VRs in medical education is of great interest since they blend physical and digital learning features. Of the 21 studies (2021-2024), 8 systematic reviews and 3 randomized controlled trials showed that XR was effective in medical education (5 studies) and surgical planning (4 studies). Six studies identified low- and middle-income countries’ limitations (eg, costs, infrastructure), but one research found that non-XR approaches were successful in resource-limited locations. Common drawbacks were limited sample sizes (3 studies) and database biases (2 studies). XR showed transformational potential but needed equitable scalability techniques.
Conclusion
The primary goal of this systematic review is to provide insight into AR research, identify potential future trends, and serve as inspiration for healthcare professionals, medical college professors, researchers, and scientists working in the fields of AR, VR, and XR in the healthcare industry.
Introduction
A revolutionary technology called augmented reality (AR) presents digital information on user's physical surroundings, thereby augmenting their perspective of reality. Rising as a fundamental instrument in contemporary medicine, AR transforms patient treatment and medical education. AR is a great help in modern healthcare systems since it enables a more complete knowledge of difficult medical events by combining virtual data with real-world surroundings. 1 AR and virtual reality (VR) can be employed in clinical settings to provide patients with more engaging and interactive experiences. For example, AR can be used to superimpose information about a patient's condition onto their body, making it easier for medical personnel to explain and diagnose their illness. VR can be utilized to deliver immersive and calming experiences, such as virtual nature walks, to patients in order to relieve anxiety and pain. 2
From helping surgical planning and improving patient care to supporting medical trainees in visualizing complex anatomical features, AR has wide medical uses. Through interactive visualizing tools, AR has been quite helpful for patients understanding difficult medical issues. Furthermore, the necessity of creative support systems has become more important during public health emergencies like the COVID-19 epidemic, where AR was vital in maximizing under pressure healthcare services. 3 AR applications have been effectively used in medical education for image-based training, classroom learning, anatomical instruction, and clinical skill simulations. These instruments generate interactive learning settings whereby students may practice procedural procedures, investigate anatomical features in 3 dimensions, and get real-time feedback. The flawless blending of digital and physical learning elements has the power to completely rethink conventional teaching models and improve medical trainee knowledge retention. 4
This systematic review aims to present a thorough overview of AR's present uses in medical education and healthcare together with pointing up future possibilities and developing trends for the technology. The results shown are meant to motivate researchers, medical educators, doctors, and other professionals involved in AR, VR, and extended reality (XR) advancements in the healthcare industry thereby promoting additional investigation and application of these transforming technologies.
Materials and Method
Study Design and Search Strategy
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines until December 2024, and comprised of a preliminary search, study evaluation, eligibility, and risk of bias assessment. 5 Study was carried out in accordance with best practice guidelines. The risks of bias were reduced by following a rigorous and transparent review protocol. The reporting of this study conforms to the PRISMA checklist (attached supplementary). The systematic nature of the study precluded registration of the review protocol and ethical approval from the institutional ethical committee. Medical subject headings and keywords connected to the primary ideas of “Artificial Intelligence,” “Augmented Reality,” “Medical Education,” “Disease Diagnosis,” “Healthcare Accessibility,” and “Digital Health Technologies” helped shape the search strategy. Boolean operators were utilized to combine keywords; the “OR” operator was used inside each construct and the “AND” operator linked constructions to guarantee a wide yet targeted search result, as shown in Table 1.
Comprehensive Search Strategy Implemented Across PubMed and Scopus Database Using a Combination of Medical Subject Headings (MeSH), Boolean Operators, and Relevant Keywords. The Search Terms Were Structured to Ensure a Wide Yet Focused Coverage of Literature Relevant to the Integration of AI and AR in Medical Practice and Education.

Abbreviations: AI, artificial intelligence; AR, augmented reality.
Data Sources
Following the search method, scientific databases including PubMed and Scopus, were searched; the retrieved articles were imported into the EndNote reference management system (EndNote X20). In addition, to find more similar research, a hand search was conducted in the list of references of the included articles, as well as a Google Scholar search with different keyword combinations.
Study Selection Process and Inclusion–Exclusion Criteria
The search strategy aimed the publication of articles highlighting how artificial intelligence (AI) and AR influence medical training, disease diagnosis, treatment, and healthcare accessibility. Each selected paper was examined by 3 researchers and included in the final review if it presented the greatest results for learners in terms of group size in simulation. Focused on peer-reviewed English-language papers, the inclusion criteria examined the implementation of AI and AR technologies in experimental or clinical healthcare environments. Studies were included if they addressed: (a) the use of AI in disease diagnosis, treatment optimization, and patient data analysis, (b) AR applications in medical education, surgical training, and patient care, (c) the impact of these technologies on low- and middle-income countries (LMICs), and (d) ethical concerns and implementation challenges in the adoption of AI and AR in healthcare. Exclusion criteria included: (a) studies emphasizing only on theoretical models without experimental validation; and (b) non-peer-reviewed publications, commentaries, and editorials. To guarantee coverage of the most recent developments in AI and AR, the main search range ran from January 1, 2010 to December 2024. Selected early 1900s historical articles were also added to offer a complete chronology of technical advancement and fundamental field changes. To find more pertinent research, a secondary hand search of the reference lists from the included papers was done.
Quality Assessment
Using the GRADE framework, we evaluated risk of bias (using Cochrane/ROBINS-I tools), consistency, directness, accuracy, and publication bias to gauge confidence in the evidence for every outcome. High, moderate, low, or very low were the categories for evidence certainty.
Data Extraction and Synthesis
Three reviewers conducted independent analysis of papers that fulfilled the inclusion criteria by using a standardized extraction form. The research collected information about “First author and publication year” as well as “Study Title,” “Study Design,” “Country and LMIC status,” “Population and technology type,” “Application Area,” “Key Outcomes,” “Main findings,” and “Limitations.” The researchers determined single-center studies from country specifications which included “multicountry” for multicenter trials or from the LMICs.
VR, AR, Mixed Reality, and Metaverse Technologies: History and Current Scenario
How it Started
Several new fields in technology are emerging in healthcare that aim to provide a new setting for work that can be changed as needed, including VR, mixed reality (MR), AR, and metaverse. VR, MR, and AR all fall under the term extended reality that in which different environments and immersive technologies are demonstrated and represented. 6 When the first head-mounted display (HMD) was developed in 1965, the term “virtual reality” (VR) first originated to describe a situation where the user perceives the virtual environment as real and behaves realistically in it. The first artificial reality lab was opened in the 1970s in Videopalace. 7 One of the respected definitions of VR was by Gigante as “The illusion of participation in a synthetic environment rather than external observation of such an environment. VR relies on a 3-dimensional (3D), stereoscopic head-tracker displays, hand/body tracking and binaural sound. VR is an immersive, multi-sensory experience”; 8 VR is then a fully immersive digital environment designed synthetically for various purposes. A user in healthcare as a healthcare worker or patient should feel immersed in VR as though they are placed in a second world but operate similarly with physical surroundings. 9 This experience is becoming more immersive, amplified, and interactive and more natural with specialized multisensory equipment. 10 In order to produce more immersive simulations for medical education, these technologies have been integrated over time with additional sensory experiences like motion tracking and haptic feedback. These simulations are now becoming more user-friendly and accessible globally. Their study revealed that medical personnel may rehearse difficult operations safely and affordably without endangering patients by using VR-based simulations. It also demonstrated how AR systems may be used with actual instruments to aid in surgery or other medical procedures. 11
Is AR-Powered Digital Clinic Worth the Hype?
A technique called AR projects digital data over the actual environment. It is getting more and more common in the health industry since it offers a special chance to comprehend a certain group or circumstance in more detail. Users of AR-based applications may respond physically or emotionally to a scenario or surroundings or have a visceral experience. During a very short period of time, this experience may aid in developing understanding and provide an embodied view of different groups. This is advantageous for healthcare professionals. The evolution of AR and VR over time has the potential to produce settings that are both effective and safe for the development of new systems and the improvement of current ones, thus it is vital to understand their history. 12
AR takes a relatively far deviation toward real environment rendering virtual interference relatively minimal and focused on adding context and effects such as text, graphics, sounds, videos, and GPS data to already existing real-life objects and does not add fully virtual objects. 13 It rather adds these virtual elements to real-life objects to enhance them and merges the virtual and physical worlds. 14 A medical user would be seeing both real-life objects with digital effects to further guide and help. MR is a middle ground between VR and AR in which the 2 are simultaneously integrated and their elements coexist and interact in real time. 15 MR can be considered as advanced AR in which digital and real environment interact with each other instead of being limited to the case of AR where digital only enhances real environment. 16 Therefore, a medical user as a healthcare worker, student, or patient would have the digital environment changing and reacting in correspondence to their actions and choices.
Revolutionizing Healthcare With Metaverse
Metaverse is best understood in terms of healthcare as the Internet of Things for the medical sector made feasible by wearable technology like AR and VR eyewear. Healthcare is about to enter a new age of innovation with the emergence of AI, VR, AR, Internet of Medical Devices, Web 3.0, intelligent cloud, edge, and quantum computing, and robots. Metaverse is a different parallel universe made up of entirely virtual environment or environment that merges reality and virtual environments, not a related physical technology. It would be a virtual environment or setting that could be accessible via XR where people or things might communicate with one another, such as in a virtual medical school. It would be built on XR technologies with the aid of stereoscopic displays that would provide depth perceptions, where each eye would have displays that would accurately reproduce the sight in physical settings and real-world activity. 17 XR systems would also allow for 3D spatial and binaural audio benefit that is not provided in 2-dimensional (2D) systems of conventional digital instruments that would replicate real-life audio. 18
Medical Training With AR: What Data Shows
There has been a worldwide trend in the use of AR, VR, and MR technologies for surgical research. Major contributions to the literature have been made by organizations in the United States, the United Kingdom, Italy, and Canada. 19 The most commonly studied medical conditions in this field are pain, stroke, anxiety, depression, fear, cancer, and neurodegenerative disorders. The literature concludes that XR technologies have the potential to cause a paradigm shift in healthcare education, but a learner-centered approach is necessary for its success. A meta-analysis to assess the effectiveness of AR in medical training was conducted; 13 studies that included 654 participants were used to assess how effective AR is compared to other educational methods, such as conventional teaching and non-AR techniques, in terms of skills, knowledge, confidence, performance time, and satisfaction. Results showed that AR improved performance time (I2 = 99.9%; P < .001), confidence (I2 = 97.7%; P = .02), and satisfaction (I2 = 99.8%; P = .006), but had no effect on knowledge or skill levels when compared against control conditions (I2—knowledge: 99.4%; skill: 97.5%). It can be concluded from this study that while AR has potential benefits, it should not replace traditional learning methods completely due its lack of impact on certain areas like knowledge and skill development. 20 However, it is not as effective when it comes to acquiring some aspects of knowledge or skill development which means traditional learning methods should still form the basis for teaching these specific areas. 21
Digital Health Literacy in Person-Centric Era: Overview
The correlation between health literacy and health outcomes encompasses access to and utilization of healthcare services, interaction between patients and providers, and self-care. Computer techniques can be created to test comprehension, broaden or simplify ideas, and do so without any time constraints. AI, machine learning, VR and AR, and blockchain are recent technological innovations that have the potential to expand technology's function beyond data collection into a more unified system (Figure 1). Instead of being apathetic spectators, people may actively participate in their healthcare thanks to digital solutions. The use of digital technologies can increase someone's confidence in the viability of their idea and reinforce their belief in its success. 22

Fascinating Examples of Augmented Reality (AR)-, Virtual Reality (VR)-, and Extended Reality (XR)-based Applications in Healthcare and Medicine.
Digital solutions can provide more chances for learning by incorporating multimedia education in a variety of formats, such as videos, audio, and textual material in multiple languages and reading levels, using both formal and informal teaching approaches. By allowing them to express their thoughts and actively participate in their healthcare, patients can improve their ability to make decisions and participate in shared decisions. When implementing an engaging approach or an educational solution, our health literacy teaching framework gives emotional needs of the individual top priority. 23
Although if a precise definition of health literacy and an instructional framework are crucial, additional study is required to identify more practical approaches to include health technology in order to continually improve health outcomes. After finalizing this article, we all believe that developing digital health literacy necessitates redefining healthcare consumers as individuals, rather than disease states, and moving away from disease management toward patient empowerment. When problems are solved digitally, a far more powerful resource is revealed: the actively involved patient. 24
Potential Future Use: Are We Ready for the Changes?
Alternate reality creates a unique experience for learners by allowing them to interact and influence a narrative through their decisions. It does not require any hardware or equipment investments, making it significantly cheaper than AR or VR modalities. Participants can use real-world tools such as interacting with patient data in electronic health record simulations which helps create an immersive yet low stress environment that encourages problem solving and learning. XR-based HMDs can be used as an effective tool for medical education in LMICs. 25
The use of XR technology in medical education, specifically HMDs, provides an immersive and interactive experience that combines physical objects with computer-generated elements. HMDs are a type of XR device that display 3D images or videos to create realistic simulations, which can be used in a variety of applications, including medical education. A literature review of 27 studies with a total of 956 participants, most of which included medical students and residents, found that XR-based HMDs have beneficial effects on learning knowledge and skills, with users demonstrating greater enthusiasm and enjoyment compared to traditional methods. 26
Siff and Mehta 27 observed that the interactive holographic mode of learning was effective in the acquisition of knowledge for surgical anatomy. Study participants ranked the AR-based training as much better when compared to conventional training. Despite higher motivation and enjoyment for learning anatomy with HMDs, there was no significant difference in knowledge acquisition when compared to learning from textbooks. This is similar to other reports, suggesting XR interventions are at least as effective or more so than their selected conventional therapy counterparts. These findings suggest that XR-based HMDs may have potential for use in medical education in LMICs. However, the majority of the studies were conducted in high-income countries, so further research is needed to determine their effectiveness in LMICs. 8
Researcher, Clinician, and Patients’ Consensus: Trust Game?
Understanding different viewpoints is essential for working together to bring about a technological revolution. It would help us better grasp the constraints and knowledge gaps, as well as aid in designating tasks in various disciplines, ultimately improving global healthcare. This section aims to discuss the many viewpoints on the deployment of AI in healthcare. New AI research is developing. Medical research involves vast amounts of patient data. AI helps researchers handle screening, diagnosis, and treatment data. Due to such investigations, medical specialists may learn about subject–outcome relationships. Researchers say AI technology can assist physicians and researchers make judgments by uncovering crucial facts buried in massive data sets. 29 Research funders in technology, education, and health should also finance AI-related research. AI in healthcare and AI-assisted learning requires transdisciplinary study. Global humanitarian health analysis and interventions need AI research and education. Virtual health tours for medical professionals to learn about health issues in other countries might start this. 30
AI may boost healthcare company productivity, workload, collaboration, performance, and satisfaction. AI improves imaging and diagnostics. Clinical screening may be done more efficiently and effectively, enabling individualized and precision therapy tailored to each patient. AI will assist physicians manage large patient loads and low staffing. It will allow hospital employees to log all medical visits and talks, reducing administrative labor. An ambient computing device may collect vital signs and clinical data during a medical session. Hence, patient–doctor contact may take up more time. 31 AI can monitor and retain patient health information throughout a patient's lifespan, helping clinicians offer high-quality treatment. AI replacing doctors is a common misconception. Doctors believe AI-based healthcare technology cannot replace professional expertise and knowledge. A licensed doctor must assess a patient's condition and treatment options. Doctors see AI-based solutions as tools, not decision-makers. Doctors think AI may improve evidence-based knowledge by using real-world care data and recommending effective treatment techniques. The clinicians are clear that data use should improve patient outcomes, healthcare access, or community. 32
Patients are confused about computers’ capabilities, according to qualitative research on AI in radiology. In this research, patients respected doctors’ knowledge and doubted AI systems. They recommended a second radiologist reading. Personal interaction allows patients to ask questions in a safe environment and have someone understand their symptoms and sentiments after their diagnosis. VR technology and implicit bias research are used to tackle social health inequalities, cultural insensitivity, bias, and prejudice. Despite intriguing, these AI algorithms are yet in clinical trials; therefore, it is uncertain whether they will be beneficial in clinical results. 33
Medical Education, Training, and Upskilling of Healthcare Professionals and Medical Students
XR is a novel technique for building simulated experiences that are more affordable than conventional simulation modalities. Its goal is to integrate, or mirror, the real world with a “digital twin world” that can converse with it. As noted earlier, the terminology XR comprehends various technologies, such as AR and VR. 34 AR may augment traditional teaching tactics by superimposing digital material over the real environment, providing students with a more realistic and interactive picture of anatomy, physiology, and medical procedures. Similarly, VR allows trainees to perform simulations of medical procedures and operations in a safe environment, providing practical education and enabling them to make errors without hurting patients. VR may also be used to create interactive anatomy and pathology classes. 35 Furthermore, Kyaw et al 36 discovered evidence indicating that VR, when compared to traditional education or other forms of digital education such as online or offline digital education, improves post-intervention knowledge and skill outcomes of health professionals; similarly, Baashar et al discovered evidence indicating that AR significantly increases performance speed, contentment, and confidence, but it is less effective in areas such as knowledge and skill. 37
Surgical Training
VR and AR have been used in many ways in healthcare industry, including surgical training. VR and AR platforms use head mounted displays (HMDs), head-tracking devices, audio headsets, audio and noise-canceling headphones, and handling and automation tools to create a multisensory, 3D experience that could contribute to surgical accuracy and education. Lesch et al found that laparoscopic appendectomy and cholecystectomy films were less effective learning aids than the teaching in procedure-based simulations (TIP) platform, which increased confidence in repeating the procedure. 38 The laparoscopic-looking TIPS surgical illustration immersion platform lets users interact with anatomical drawings. Blumstein et al found in a survey that VR instruction was more effective than a standard guide for inexperienced medical students using their model of simulated tibia shaft fracture intramedullary nailing, with significantly higher aggregate global assessment scores. 39 These findings are important because they inspire educators to employ XR in classrooms and labs. HMD-assisted teaching was more enjoyable than traditional instruction, according to Peden et al Self-directed learners who used HMDs with pre-recorded movies learned, as well as wet-lab students. 40 In a year-long neurosurgery elective course, Atli et al used Surgical Theater's Precision VR visualization platform to incorporate diverse teaching modalities. At the end, all students reported increased competency and confidence and believed VR had improved their grasp of neuroanatomy and neurosurgery. Every student thought the course was useful and VR was a good learning tool. 41 XR may also solve global issues. UpSurgeOn, a startup, builds hybrid teaching platforms using low-cost and high-tech digital and physical technology to boost manual and mental training. In response to the global need for novel neurosurgical training technologies, including in LMICs, this strategy cuts expenses. XR can improve surgical training by giving doctors tools to boost performance, confidence, and patient outcomes. 42
Nursing Training and Patient Care
Nursing education is essential to delivering high-quality patient care nurses. Clinical simulations have long been an excellent nursing teaching method. These simulations may assist trainees gain experience and confidence before treating patients in a safe and controlled environment. Holographic MR, an affordable and realistic technology, could improve nursing education. This technique can create a standardized virtual patient for healthcare simulations. A computer-generated, interactive virtual standardized patient can simulate many medical conditions and circumstances. This technology enables nursing students a realistic and immersive experience to improve their clinical abilities safely, regulated, and cost-effectively. 43 Holographic MR may benefit nursing education with its low cost and accuracy. It not only gives nursing students hands-on experience in a range of clinical settings, which may boost their confidence as they prepare for patient care, but it may also reduce the cost of clinical simulations, including actors, equipment, and facilities. Furthermore, it may provide nursing students with a standardized and uniform experience, ensuring a high-quality education independent of location or program. 44
Despite the benefits of holographic MR in nursing education, there remain challenges. Faculty who use technology must be properly trained, which is a major obstacle. To ensure technology functions properly and is available to all students, strong technical support and infrastructure are needed. Finally, nursing educators and healthcare practitioners can work together to accurately portray real-world clinical circumstances in the virtual standardized patient. 45 Economic and realistic holographic MR may improve nursing education by giving students a safe, controlled, and cost-effective way to practice clinical skills. The virtual standardized patient may help future nurses prepare for real-world patient care while cutting costs and standardizing student experience. This technology's concerns must be addressed to ensure its successful deployment and improve nursing education. 46
Anatomy Teaching
XR tools can be an effective aid, or alternative, to traditional teaching methods in anatomical science and beyond. Anatomy has always been a challenge for medical students; understanding the relationships between structures on a 3D or 4-dimensional (4D) plane, while studying in 2D textbooks is particularly daunting. That is why AR and VR are gaining a crucial role in anatomy teaching, as they can greatly enhance the learning experience. 47 XR tools are pushing in this direction to comprehend 3D printing, virtual mirrors, and seamless integration with technological devices, such as mobile learning ones. 48 The same goes for VR, with either semi-immersive or immersive technologies, such as 3D puzzles, cooperative systems, and volume rendering. Kurul et al. 49 discussed their findings of the pre-test and post-test knowledge, revealing a much greater difference in favor of the 3D interactive VR group, showing its benefits. On a similar note, Weeks et al showed that a 3D computed tomography (CT) hologram improved students’ average percentage of questions answered correctly, up to 15%. 50 However, this has not always been the case, as Stepan et al demonstrated that an immersive VR learning resource improved student motivation and provided a better overall learning experience; but, in terms of teaching neuroanatomy, VR technology was just as helpful as conventional textbooks. 51 Similar to Chan et al, 360° videos were assessed as more practical and entertaining than 2D videos, despite no significant difference in perceived ease of learning. 52 This demonstrates that although XR technologies might be exciting, they are still in the process of determining the best approach to significantly affect students’ understanding. However, AR and VR research have presented a considerable amount of data showing their advantages in teaching anatomy; such evidence has been documented and summarized in, where Zhao et al found that VR enhances anatomical post-intervention test results in contrast to other training modalities. 53
On the other hand, Uruthiralingam and Rea highlighted the upside of XR but simultaneously noted some crucial factors to consider, such as the type of technology people will employ to study depending on their visuospatial abilities. 54 A desktop VR system for studying anatomy is more beneficial for people with low spatial skills; however, people with high spatial abilities would not be able to use such technology. 55 Moreover, one aspect that is too often overlooked is the cognitive load theory and how it should guide the design of XR tools. 56 Küçük et al created MagicBook, a neuroanatomy learning aid, using mobile augmented reality (mAR) technology. The experimental group reported higher accomplishment and lower cognitive load while utilizing mAR apps, demonstrating the formation of an efficient and effective learning environment in anatomy training, assisted by the use of mAR applications. Student retention was better and cognitive scores were lower, resulting in improved results. Ultimately, XR has the potential to change anatomy instruction by providing students with immersive and interactive learning experiences that increase student comprehension and retention of anatomical information 57 (Figure 2).
Teaching Faculty Demonstrating Digital Dissection with Anatomage Table at International Medical Faculty, Osh State University, Osh City, Kyrgyzstan. (Source: OshSU University Archive Gallery.)
Telesimulation
Telesimulation is a method for delivering instruction, training, and evaluation to learners in distant locations using telecommunication and interactive tools like HMDs, solving major issues with traditional simulation training, such as access, cost, people, and content, addressed in novel ways. 58 Almousa et al made the most out of Oculus Quest, a standalone, cordless, head-mounted VR system that works with a digital platform to create realistic clinical simulation experiences. Their system allows academic and interactive clinical training in environments analogous to the real world, enabled by real-time connection and live stream between the instructor's control panel and VR-training system. Live streaming and real-time connection are also what made it feasible for McCoy et al to assess the viability and efficiency of employing telesimulation and wearable/mobile technology to teach medical professionals abroad about mass casualty incidents in emergency medical services (EMSs). 59
Regarding their opinions, sentiments, and attitudes in learning EMS-based material through telesimulation participants responded positively to all survey items. Once again, XR tools can aid in enhancing and equalizing medical training in rural or disadvantaged areas. That has been the focus of Wang et al, as they investigated how remote students can execute difficult medical procedures like Point of Care Ultrasound using AR technology without being distracted by their surroundings. Using MR capture, HoloLens recorded the first-person perspective of a model rural emergency department, serving as a platform with remote pointing capabilities. Using a Leap Motion, the mentor's hand motions are recorded and visually presented in the HoloLens’ AR world. Nevertheless, the results of the study were subpar compared to the expectations, as the system did not show a significant statistical difference when compared to a full telemedicine setup. Moreover, some participants experienced dizziness, and the mentors found it more challenging to deliver the training than a traditional teaching method. 26 As a result of offering medical professionals and students immersive and engaging learning experiences that boost comprehension, retention, and performance, XR has the potential to significantly improve medical education and training. As XR technology develops, it is anticipated to become a more vital tool in the medical industry, enhancing patient outcomes and elevating the standard of medical training and education.
Another virtual medical training innovation is the Digital Medical Education System (DIMEDUS), a cutting-edge virtual clinic campus and training platform that seeks to give high-quality training and education to medical professionals in a risk-free setting. DIMEDUS provides a one-of-a-kind combination of immersive technology, modern medical devices, telemedicine solutions, and cutting-edge learning materials. The DIMEDUS virtual clinic campus is a fully realistic simulation of a real medical clinic. It provides a variety of virtual facilities necessary for medical training and education, such as virtual classrooms, simulation labs, virtual medical libraries, and others. The virtual clinic is outfitted with cutting-edge technology like VR headsets and electronic medical records systems, allowing medical professionals to learn and practice in a realistic and interactive environment (Figure 3). The courses are taught in a number of ways, including interactive lectures, group discussions, and hands-on training in a virtual clinic environment. The portal also provides self-paced courses for medical professionals to learn at their own pace. The platform's creative approach to training and education, along with advanced technology and interactive learning resources, making it a fantastic alternative for medical professionals aiming to advance their careers. 60

Author, Dr M F Siddiqui in Clinical Setting Training on Virtual Patients (On Screen) with VR Gear in DIMEDUS Campus of International Medical Faculty, Osh State University, Osh City, Kyrgyzstan. (Source: OshSU University Archive Gallery.)
Solving Global Health Disparities: Shifting Paradigm With AI, VR, and XR
COVID-19 has increased the demand for contactless learning which has boosted the application of VR in healthcare training. VR and AR technologies grew in the field of medical education and telemedicine during the pandemic year of 2020. The remote learning has also helped to make the VR technology more affordable and reachable, thus enabling the healthcare workers to attend the training through internet connection from any part of the learning world, which in turn enhances career and development of the healthcare workers. 61 VR is used in telemedicine for remote consultations and virtual visits. This is because the interactions between the healthcare providers and the patients through VR are more real life like as compared to video conferencing or even phone calls. It also provides the doctors a 3D view of the body parts of the patients thus enabling accurate diagnosis and treatment. It also enables the medical students and other health practitioners-to-be to practice clinical skills without patients. 62
Multidisciplinary groups might remotely monitor patients using AR technology via telemedicine before the COVID-19 pandemic. Virtual care clinics provide telemonitoring. This lets clinicians remotely monitor blood pressure and heart rate and educate patients. Virtual care clinics schedule appointments and remind patients to improve treatment adherence. 63 AR helps people understand healthcare information via contextual, localized learning. Virtual things intrigue users more than text or static websites in AR. Visualizing complex medical subjects improves patient education and health literacy. VR enables doctors try innovative therapies without patients, reducing risk and enhancing education. Video conferencing, webinars, and emails enable remote work, education, exercise, and recreation, increasing social isolation. These gadgets can entertain, treat, and educate during COVID-19 quarantine. Snap's “Give Filter” enables pandemic sufferers donate from their accounts. International Rescue Committee, Feeding America, and Save the Children get pandemic aid. Our parent company, Snap Inc., gave $1 million to these charities. Snap's AR lens illustrates how other companies may use similar technology to combat future pandemics. 64
Future healthcare treatments including VR need digital literacy. Health literacy is “the degree to which a person can receive, communicate, process, and comprehend fundamental health information and services to make informed health decisions.” Digital health literacy improves patient care using AR, VR, and XR. 65 Therefore, AR may improve treatment plan adherence, service quality, and healthcare system load via learning. VR software is popular, but its usability and learning aids define its value. Developers should employ basic use cases and do usability testing with prospective users to guarantee healthcare professionals use VR apps. The risks of XR telemedicine include ethical issues like when it is appropriate and ensuring practitioner competency; misuse of immersive features for therapeutic purposes; privacy issues due to data logging by proprietary devices and software used for XR applications; and lack of usability or easy integration into existing clinical workflows. 66
Harnessing Global Health and Medical Industry With Tech
Medicine has always been an in-person experience. Despite this, the advent of modern technology involving the digital world has not only ushered in a new era in the healthcare system, but has also pirated the entertainment business. Several areas of medicine have seen significant transformations in recent years. These technologies are considered tools aiding in clinician guidance, patient education about their health, or treatment delivery. 67 For example, the applications of VR/AR have helped in the visualization of medical images in a 3D manner. Different sets of studies were performed to fuse magnetic resonance imaging (MRI) data and holographic augmented reality for the purpose of planning neurosurgical procedures. In addition, these technologies have potential to enhance surgery in general and to promote less invasive procedures. 68 Moreover, it has provided a learning platform for medical students as well. Many studies have demonstrated the use of these digital instruments in multiple clinics where it has been able to evolve educational requirements for oncology learners. Virtual reality for radiation training has provided an unlimited risk-free practice for radiation therapists and an improved understanding of spatial concepts. 69 In addition, the applications of VR/AR technologies have benefited the psychiatry department in therapy. Several studies have shown that for people living with dementia, implications of VR/AR have enhanced patients’ well-being and cognitive function and are preferred when compared to non-virtual experiences. 70
These innovative models have also suggested the conduction of remote routine follow-up visits with patients, condition management by several physicians, and genetic counseling. 71 In India, a pediatric brain tumor study showed that over 25% of patients quit neuro-oncology treatments due to late diagnosis and lack of management consistency. For such reasons, telemedicine has facilitated the communication between advanced centers and local care facilities for a successful improvement in management of these situations. 72 Metaverse is not only wonderland to escape the crowdedness of reality, but it is also a place that offers facilities and services for people to experience. Multiple studies have shown that metaverse can be utilized in disease diagnosis, surgery, and treatment. 73
Assisting General Surgery and Trauma Cases With AR, VR, and XR
Information processing and data computing have helped people in numerous personal and professional areas throughout the past century. Several new technologies have entered healthcare. Computer graphics in medicine originated with 3D medical imaging structures like CT scans and MRIs. This technology has transformed medical diagnosis and treatment. Technological advances have also led to the widespread usage of AR, VR, and XR in surgery. This is especially true given the increased ability to examine and negotiate human anatomy preoperatively to choose the appropriate treatment and method and intraoperatively to aid the surgeon. 74 Recent research shows AR and MR improve surgical precision. In trauma surgery, Goh and Liow report improved hip and knee arthroplasties accuracy. These technologies allow intraoperative manipulation, reducing preoperative calibration and improving operation efficiency. Safety and recovery have been improved by using these technologies into training and surgery. 75 AR, MR, and XR have enhanced healthcare and lowered perioperative costs. Smart devices avoid the high capital costs of robotic and navigation systems. Smart technologies may improve healthcare service and lower costs by decreasing manpower. They improve and lower medical training costs. They walk surgical residents through skills they've acquired or need to practice. Simulating rare diseases can help surgeons improve. Study shows medical apprenticeships are outdated. Professionals teach surgical residents, which increases patient discomfort, operation length, cost, and danger. Additionally, learning machinery algorithms will evolve to collect more data and improve education. 76
Technology has changed post-surgical monitoring and rehabilitation. The new field of telerehabilitation uses virtual and augmented environments to aid patients with house-based trauma treatment. AR, MR, and XR have improved surgery training, performance, costs, and results. Others say such devices have downsides. Although short-term trials show benefits, Goh and Liow call for long-term research. 77 Despite their initial advantages in skill learning and delivery, they may produce a gap in surgeon skill retention and improvement. Their initial use in resident training programs may not be as cost-effective as prior studies predicted. Batteries for lengthier operations, lack of voice recognition for medical terminology, and privacy seem to be limits of the aforementioned technologies, which need to be explored and developed to be more effective in surgery. 78
AR and VR in Basic and Advance Life Support Certification
AR and VR training can enhance medical education and life support training in the limited-resource settings of LMICs and revolutionize them. In situations where there are few simulation labs and professional instructors, these technologies are low cost and easily deployable skill development solutions. The virtual platforms are also beneficial as they provide standard and quality training without the need of equipment which may be scarce in such places. VR-based life support training can be used to deliver training in the rural areas where there are limited options for healthcare education as it does not require actual space and equipment. 79 Virtual scenarios with manikins in basic life support simulators help the trainees to execute life-saving actions in a setting with restricted resources. Without technique, the monitoring can be used as a teaching tool for cardiopulmonary resuscitation under direction. The AR defibrillation with VR technologies assist also in this appropriate approach for multilingual training, which makes the training fit for different populations in LMICs. The self-paced, repetitive training experiences enable the healthcare workers to enhance professionally, where there is a shortage of teachers. When combined with mobile technologies, AR and VR can provide the necessary support to the underdeveloped areas with health limited care facilities. 80 Thus, through the enhancement of skill retention, emergency response time, and preventable mortality, AR- and VR-based life support training can help LMICs to build a stronger healthcare workforce and reduce the inequity in the global health.
AR–VR in Critical Care
VR and AR could revolutionize critical care by increasing patient outcomes and saving costs. VR and AR technology can improve patient experience and healthcare personnel treatment abilities in critical care. A fully immersive 3D VR world has been found to reduce patients’ anxiety, dread, and discomfort. 81 A VR headgear displays calming videos of landscapes or other images plus hypnotic speech and breathing exercises. VR helps severely ill people rehabilitate and move by offering a safe and controlled environment. VR can also help critically sick patients cope with the stress of the intensive care unit (ICU) by providing an escape from the environment. VR's immersive experience may also help sufferers feel empowered. The same effects apply to pediatric ICU patients. VR reduces chronic and acute pain in patients and can enhance or replace pharmacological pain management. Pain was reduced most in pediatric, burn, and postoperative patients. This avoids adverse effects of painkillers including addiction. 81
Critical care training with AR has been promising. As mentioned, AR allows critical care professionals to practice placing a central venous line, maintaining tracheostomies, intubating patients, and performing cardiopulmonary resuscitation. 82 One drawback of VR is “cyber sickness,” which can cause headaches, nausea, and vomiting. A headgear and head motion during VR may create this sickness. There is also little evidence that VR and AR equipment might spread diseases like drug-resistant germs. Before using VR and AR in the ICU, study is needed. 83
Telemedicine: Post-Pandemic Scenario
Telemedicine sends medical data between places. Since the COVID-19 pandemic, the healthcare system has worked to adopt telemedicine. Telemedicine has been utilized for 5 years before COVID-19. It worked well in severe acute respiratory syndrome, Middle East respiratory syndrome, and Ebola epidemics. According to research, telemedicine may enhance patient outcomes. Telehealth is utilized for monitoring, management, consultation, medical education, and patient education. 84 Telemonitoring involves sending medical data to doctors electronically. It's important because clinicians may easily contact patients, assess deterioration early, and adapt therapy based on data. Congestive heart failure patients’ mortality rates dropped 20% and hospitalization rates dropped 21% with telemonitoring, according to Scott et al 85 Telemedicine also lowered mortality and improved high-density lipoprotein and low-density lipoprotein levels in coronary heart disease patients. Telemonitoring also detected lung transplant and asthma exacerbations early. It also reduced asthma symptoms and boosted exercise.
But telemedicine was used to manage patients. It also provided psychotherapy and smoking cessation. After robot-assisted therapy, Högg et al found improvement in motor control of stroke patients. 86 Telepsychiatry anxiety therapy yields results comparable to in-person management, and electronic physical treatment is better than waiting for in-person availability. Telemedicine lets patients consult doctors. Malhotra et al showed that telepsychiatry is equally accurate as in-person examinations. Telepsychiatry and in-person appointments had equivalent patient satisfaction. 87 Telemedicine may help educate patients. Telemedicine increases asthma knowledge, according to a large study. Telemedicine is used to instruct medical students. An American Association of Medical Colleges survey found that most second-year medical students prefer recorded digital lectures over live ones. Students can access educational courses, conferences, and virtual electives online and on social media. Medical schools used technology to help students enhance their research and interpersonal abilities. A meta-analysis found no significant difference between mixed digital and in-person sessions. The study found that telemedicine is cost-effective in addition to its benefits. Teleophthalmology should lower diabetic retinopathy treatment costs. In rural locations worldwide, telemedicine is cost-effective for treating depression, bulimia, and pulmonary issues. 88 Telemedicine works, but it's not commonly used in clinical practice due to many obstacles. Both technology and patients are problematic. Poor internal connections also hurt telemedicine. Slow internet caused low patient satisfaction and compliance. Patients with major medical issues who need modern telemedicine technologies may experience technical issues. In most institutions, there are no telemedicine regulations or synchronization between platforms and patients’ medical data. Patients’ reluctance to telemedicine due to lack of knowledge and familiarity, as well as home distractions, may make it harder. 89
VR, XR, and AI in Surgery
AR/VR and AI are becoming more essential in plastic surgery as they become part of our daily lives. Although this technology is young, it is evolving quickly. AR/VR begins with aesthetics procedure predictions. It is used largely not only in cosmetic, breast, and craniofacial surgery, but also in microsurgery, hand surgery, and wound healing. AI uses AR in preoperative planning, intraoperative actions, postoperative management, and outcomes prediction. 90 In preoperative simulation, MR lets patients give their opinions on the findings before the operation. La Padula et al found that patients like the 90-min breast augmentation simulation before surgery. 91
Cosmetic surgeries require accuracy, fineness, and dexterity, and VR/AR technology can represent a virtual anatomy and vasculature, which can reduce complications and improve precision, especially for craniofacial and microsurgery. A thorough review by Moosa and Dydynsky shows that AI integration in free flap surgery reduces surgery burden, making it safer and more accurate. 92 Cosmetic surgery education can benefit from VR/AR, which can replace anatomical drawings, cadavers, and manuals with 3D virtual models. Only VR glasses allow trainees to interact and understand anatomy in 3D. This method also lets students simulate surgery with virtual dissection. VR/XR surgical training is not required in medical schools; hence it is not properly supported. Plastic surgery residents also lack time for this instruction. AI cannot replace plastic surgeons in management due to ethical issues related to data security, machine learning algorithms that can mask surgery outcomes, and practices that require surgeons to always be involved in decision-making and give their opinion on outcomes. 93
Rehabilitation with Minimally Invasive Spine Therapy
The integration of AI into spine therapy has been of great interest as the traditional procedures for operations such as pedicle screw placement, known as freehand technique, depends majorly on the surgeons anatomical knowledge of landmarks. This is because a significant portion of the spinal anatomy and neurovascular is not visible during the procedure. The reliance on the surgeon's expertise creates a risk for inconsistencies and lower accuracy of screw placement; hence several techniques using AR and VR have been developed to overcome such obstacles. Moreover, the use of AI techniques has been incorporated into several aspects of minimally invasive spine therapy (MIST) beyond just surgical preparation, including medical image analysis, rehabilitation monitoring, progress tracking, and VR guidance for the patient. 94
One of the key uses of VR and AR is as an aid to navigate in the operating room. Such systems combine VR with imaging techniques like CT, MRIs, X-rays, or ultrasounds, and use image processing to track and link images to patients. They have shown to increase efficacy and accuracy of screw placement. Moreover, one of the main concerns regarding MIST is the radiation exposure which is greater than that in open spine surgeries. However, AR-based navigation systems successfully diminished the radiation dose exposure during spine surgery. Granted the use of AI in MIST is an emerging field with its sets of limitations including discomfort to the surgeon secondary to the head devices worn during the procedures with complains of headaches and dizziness. Also, there is a restriction in efficiently simulating physical touch by AR systems, which is a vital feature to surgeons. Moreover, the system places one screw at a time which can increase the operation time when compared to 2 surgeons working at different positions concurrently. 95
Result
Search Results
Database searches in PubMed and Scopus retrieved a total of 506 results. After removing duplicate studies and those that couldn't meet inclusion criteria, 219 articles were reviewed for eligibility and went through preliminary title and abstract screening. Of these studies, 21 were found to be relevant for evaluating simulation and group size; these were evaluated through full-text screening and systematic data extraction as shown in Figure 4.
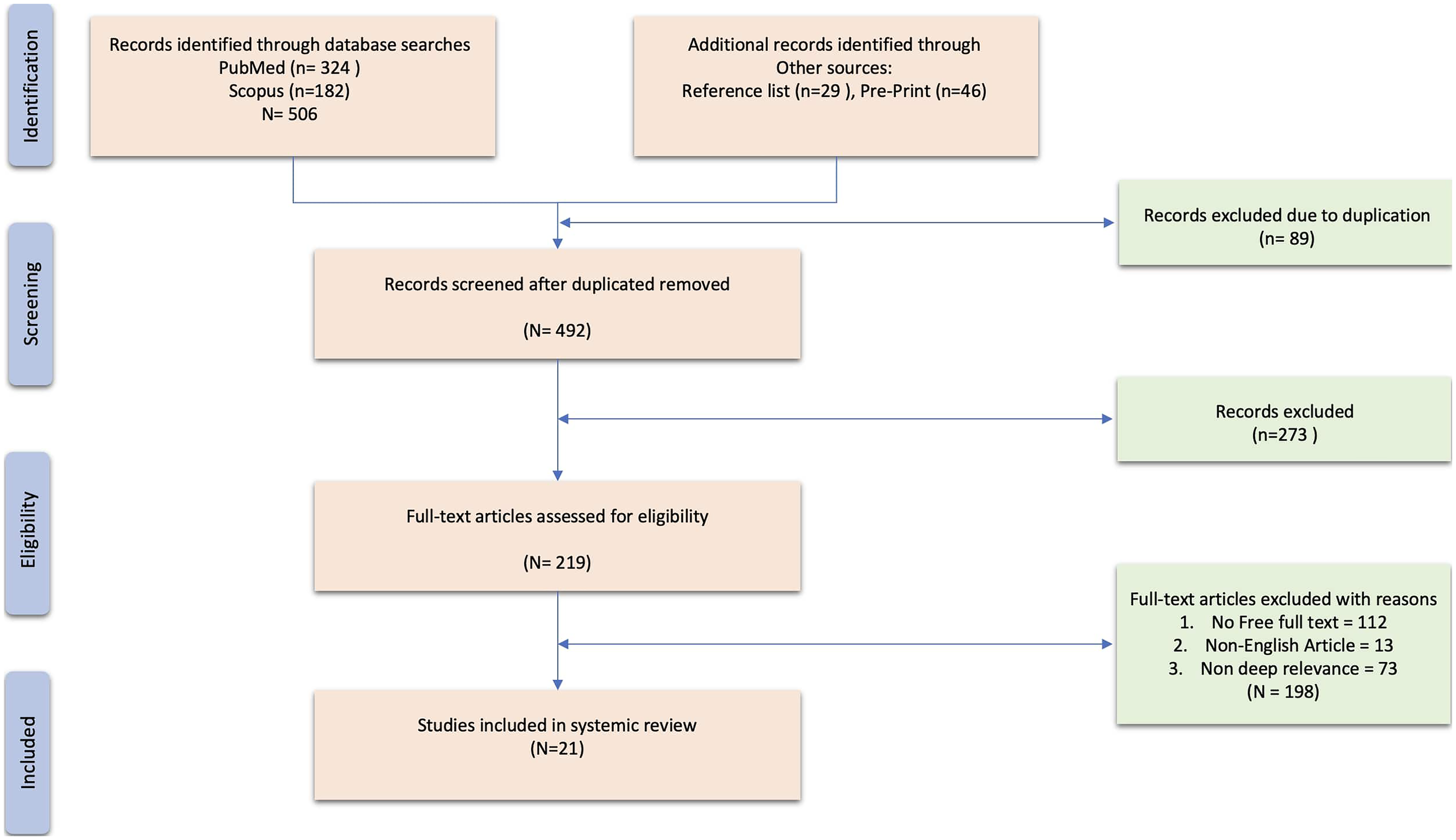
PRISMA Flow Diagram. Flowchart Illustrating the Study Review and Inclusion Process, Detailing the Steps Taken to Identify, Screen, and Select Articles for the Qualitative Synthesis.
Study Characteristics and Quality
The research studies included in this analysis present their characteristics in Table 2. The research studies were published between 2021 and 2024 in various locations across the United States, Pakistan, India, Australia, Germany, the United Kingdom, Spain, China, Ethiopia, Peru, Singapore, and multiple collaborating countries. The research took place primarily in non-LMIC locations where 15 studies were conducted, but 6 investigations specifically studied or gathered data from LMICs such as Peru, Pakistan, India, Egypt, Ghana, and Ethiopia. The research included 8 systematic reviews together with 3 randomized controlled trials, 2 bibliometric analyses, and other study types such as cross-sectional surveys, longitudinal studies, and quasi-experimental designs. The research subjects included medical students together with professionals and trainees who practiced in surgery and emergency medicine as well as cardiology and public health.
Shortlisted Articles Included in our Systematic Review.

Abbreviations: LMIC, low- and middle-income countries; AR, augmented reality; VR, virtual reality; XR, extended reality; HMD, head-mounted display; NIH, National Institutes of Health; FWCI, field-weighted citation impact; BERI, basic emergency response initiative; TAM, technology acceptance model; PU, perceived usefulness; PEU, perceived ease of use; ATU, attitude toward use; PGY-1, postgraduate year 1; CPD, continuing professional development.
Synthesis
XR has been demonstrated by studies to be beneficial to medical education. Using 27 research studies, García-Robles et al conducted a meta-analysis showing XR performed better than conventional educational techniques (SMD = 0.40) and demonstrated its best efficacy when used as additional resources (SMD = 0.52). 106 The research by He et al showed that undergraduate students who used VR with case-based learning achieved better anatomy scores (87.71 vs 82.59, P < .05) but the system had a minimal effect on their physiotherapy skills. 100 The study by Walls et al found that VR simulations enhanced both student engagement and enjoyment levels during emergency training in UK medical education. 104 The study by Mengesha et al demonstrated that non-XR educational approaches specifically flipped classrooms proved effective for improving pharmacology results in Ethiopian settings because of limited resources in LMICs. 110
The surgical applications of XR technologies demonstrated initial potential. The research by Kantor et al demonstrated that XR led to shorter procedures and decreased mistakes and better teamwork during preoperative planning. 96 The study by Arjomandi Rad et al highlighted XR's utility in thoracic surgery for creating 3D anatomical models and intraoperative navigation but did not explore its potential use in LMICs, while Keramati et al highlighted both educational and planning benefits of immersive technology in cardiology yet they warned about the expense and technical constraints.99,115
Khan et al provided a detailed analysis of the use of immersive technologies during the COVID-19 pandemic for stress management, medical training, and remote operations. 93 Bailey et al found that stereoscopic XR was useful for new residents in obstetric emergency training, but they also noted that the dependence on infrastructure limits the use of LMICs. 107 Studies performed in LMICs generated both favorable and unfavorable outcomes. The research conducted by Khan et al revealed that 83.8% of Pakistani healthcare professionals endorsed XR educational benefits yet 70% identified technological infrastructure as a major limitation. 116 The study by Li et al observed that LMIC medical education faces 2 main obstacles which include insufficient funding and technological limitations. 108 Mondal reported that India has conducted almost no XR research (1.7% AR and 2.2% VR studies) while also recommending increased research activity. 98 The studies we included in this systematic review had several limitations as well which needs to be mentioned, including high costs,96,104 small sample sizes,102,107 infrastructure dependency, 107 and limited LMIC representation.101,104 Sampling bias 97 and database restrictions (eg, only PubMed/Scopus searches) also limited generalizability.
Discussion
Rising trend of publishing articles on AI and AR in healthcare reflects growing knowledge of their evolving potential. AI and AR have drawn a lot of attention as innovations in digital health continue as they could revolutionize medical practice and education. These technologies are under research not only for their use in clinical settings but also for their capacity to raise patient outcomes and forward medical education. Driven by the ability of AI to examine massive data sets and AR to provide immersive, interactive learning chances, research articles targeted at examining their impact on global upgrading of healthcare systems have flood of volume. Integrating AI and AR into healthcare is altering therapy delivery and diagnosis making. Processing vast amounts of data, AI has shown its capacity to provide predictive insights, support diagnosis, and customizing of treatment regimens. AI has shown itself to be quicker and more accurate in fields like medical imaging, drug development, and electronic health records. AI-powered imaging technologies, for instance, enable early stage illness diagnosis including cancer, therefore enhancing patient outcomes. Furthermore, genetic risk factors are being found by means of AI analysis of genomic data, therefore providing fresh avenues for focused treatments and preventative care. AI may be used to give quicker, more accurate diagnosis and treatments in fields such as medical imaging, medication development, and electronic health records. For example, AI-powered medical imaging systems may aid in the early diagnosis of illnesses such as cancer, resulting in better patient outcomes. AI may also be used to evaluate genomic data and discover genetic risk factors for a variety of illnesses. AR, on the other hand, has the potential to improve the quality of medical education, patient care, and medical procedures. AR may be used to replicate medical procedures and operations in order to give realistic training for medical students and to improve the surgical abilities of professional doctors. AR may also be utilized to enhance healthcare by delivering real-time information on the patient's state, and AR-powered wearable devices can be used to monitor patient vital signs and send emergency alarms.
There are several examples of AI and AR being used successfully in healthcare and medical education has been included in the article as well. For example, the AI-powered chatbot “Buoy” may give patients with individualized health evaluations and suggestions, eliminating the need for in-person visits. Another example is the AI-powered robot “Moxi,” which may help hospital personnel with chores like retrieving and delivering supplies, enabling them to concentrate on patient care. The 3 most prominent medical corporations involved in the healthcare metaverse are: “Virtual hospital” is in the works at Latus Healthcare. The system consists of a simulated hospital setting, with initial emphasis on physiotherapy; “Apollo Hospitals” by Apollo Hospital Group, India has announced a novel cooperation with “8chili Corp” to facilitate participation in the metaverse, and “iMining” is the first hospital foundation to be created in the Decentraland Metaverse.
In terms of AR, the usage of AR in medical education has been found to increase medical students’ information retention and surgical abilities. In one research, medical students who got AR-based instruction performed better in laparoscopic surgery than those who received standard training. AI and AR have the potential to aid LMICs through boosting access to healthcare and medical education. For example, AI-powered telemedicine may give remote consultations and medical treatment to patients in rural or underdeveloped locations where medical practitioners may be scarce. Moreover, by delivering high-quality, interactive training to medical professionals in LMICs, AR-based medical education may assist to overcome the education gap.
VR and XR have the potential to change the way healthcare and medical education are offered in LMICs and contribute to addressing problems driven by a lack of resources. When other tools like cadavers, high-tech medical gadgets, and skilled teachers are hard to come by, these technologies can be used as quick and cheap ways to train doctors and treat patients. For example, Osso VR and other VR options offer realistic surgery models that can greatly lessen the need for real bodies for anatomy training. XR tools, like Microsoft's HoloLens, can be used to perform treatments and diagnoses from afar, making it easier to get specialized care in places that are hard to get to.
Despite the potential advantages of AI and AR in healthcare and medical education, there are still problems and constraints. One difficulty is the expense of integrating these technologies, which may be too expensive for certain healthcare institutions, especially in LMICs. Another difficulty is the need for regulatory control to verify that these technologies are safe and effective. Moreover, the application of AI and AR in healthcare and medical education creates ethical considerations, such as privacy and informed consent concerns. For example, the use of AI-powered algorithms to make medical diagnoses raises concerns regarding medical personnel liability in the case of an inaccurate diagnosis. From improving diagnosis and treatments to increasing medical education and training, AI and AR have immense promise in healthcare and medical education. Although there are certain hurdles and restrictions to using these technologies, the advantages they provide make them well worth investigating. AI and AR have the potential to enhance healthcare outcomes for people all around the globe if the ethical implications of these technologies are properly considered and implementation issues are addressed.
Preparing and Combating Upcoming Infectious Disease Epidemics With AI
Medical education and patient care have been profoundly impacted by the unanticipated COVID-19 epidemic. Notwithstanding these difficulties, patients and the healthcare system have shown amazing tenacity and creativity to produce workable but temporary solutions preserving continuity. Whether the temporary policies implemented during the epidemic will be kept long term in medical education and telemedicine is yet unknown. Some technical developments motivated by the epidemic may have long-lasting advantages that demand careful thought for retention or adaptation in the changing scene of healthcare education. Medical teachers and other healthcare professionals must critically evaluate these developments as we move past the COVID era, so conserving those clearly improving medical education and patient care.
Pandemic Predictive Modeling
AI can be used for predictive modeling to assess the spread of pandemic like recent COVID-19 and evaluating the alterations in infectious capacity of COVID carriers over first days of their illness, aiding in creating control measures for the virus. An example is a COVID-19 forecast model was proposed that estimates and considers the variation of infection rates and the impact of control strategies and public awareness. The model combines a susceptible-infected model, natural language processing module, and long short-term memory network creating a hybrid AI model with enhanced COVID-19 predictions. This model is superior as it takes into account the different infection rates of COVID-19 positive individuals, unlike conventional models that adopt a uniform rate. AI can also aid in predicting the protein configuration that is vital for viral replication. Such model includes a deep learning approach that provides insights into such proteins fold shape, binding site side-chain configurations. AI allows for an accurate and fast prediction of such structures allowing an understanding of the different viral variants and their target mutations to weaken the protein and the virus. 117
Diagnosis
COVNet is a 3D deep learning model for COVID-19 identification through CT scan imaging and distinguish it from community-acquired pneumonia. It retrieves local 2D and global 3D characteristics from CT scans, processes the images by slice, coalesces them through max-pooling, and outputs a probability score for the pneumonia (COVID-19 vs CA vs non-pneumonia) via a fully connected layer and softmax activation. The images are then processed by COVNet for diagnosis. This model attained high sensitivity and specificity in the recognition of COVID-19 of 90 and 96%, respectively. 24
COVID-19 Drug and Vaccine Designing
When COVID-19 first emerged, the surge of infections and deaths generated a pressing demand for pharmacological treatment. To which experts elected to repurpose drugs conventionally used for other infections, for use in COVID-19. An example is CoV-KGE, a network-based deep learning approach that detects such drugs for COVID-19 treatment. It used a comprehensive knowledge graph from 24 million PubMed publications relating to medications, proteins, viruses, and pathways to recognize 41 medications as possible therapies. Furthermore, CoV-KGE supported the drugs therapeutic connotations using information from COVID-19-infected human cells and clinical trial data. Through utilizing such AI programs scientists can concentrate their efforts on the most effective drugs, saving on financial and time resources. 118
Combating Ebola
One of the priorities in any epidemic is the collection of data in real time pertaining to infected individuals, their interactions and possible contacts. This data can then be analyzed and used to maintain follow-up with individuals after isolation and treatment. Data can also be shared with neighboring countries to limit spread and allow preventative interventions to be carried out. During the Ebola epidemic in 2014 several AI systems were created for this purpose, the 3 most effective ones include Surveillance and Outbreak Response Management and Analysis System (SORMAS), CommCare, and Sense Ebola Followup App. 119 SORMAS is an open-source system that allows real-time, 2-way exchange of information gathered from mobile devices between healthcare workers on the field and the Ebola Emergency Operations Centre. SORMAS allows management of follow-up, self-generated status updates, and GPS tracking allowing for epidemic management. 120
CommCare is another open-source platform that allows low-income countries to build Android-based mobile applications. This was used to enable gathering data from mobile devices and return analyzed data to the same devices. Sense Ebola Followup App is a mobile application created for 21-day follow-up of patients. It kept track of patients’ laboratory findings, symptoms, and contacts and had an alert system for fever (≥38 °C) for followed up contacts. 121
Future Direction and Challenges
The integration of AR and AI can have a profound impact on the enhancement of medical education and healthcare delivery, specifically in the context of LMICs. Despite their transforming potential, there are still significant barriers to the uptake of these technologies including lack of acceptance, which come with many infrastructure, accessibility, and ethical concerns. Implementation of AR and AI in LMIC settings is sensitive to these challenges and thus requires promotion of novel applications to ensure effective integration (Table 3).
Clear Summary of Both the Challenges and Benefits, Emphasizing how AR and AI can be Game Changers in LMIC Medical Education and Healthcare Systems.

Abbreviations: LMIC, low- and middle-income countries; AI, artificial intelligence; AR, augmented reality.
Limitation
The research studies examined different educational results (eg, skill acquisition, engagement, cost barriers) which made it difficult to directly compare learning effectiveness or group size effects. The synthesis became complex because XR applications included both procedural (eg, surgery) and non-procedural (eg, anatomy education) types. The search of multiple databases including PubMed and Scopus without date or language restrictions helped reduce publication and selection biases. The majority of studies (15/21) came from high-income nations which provided better resources such as advanced XR infrastructure and funding but this limits the generalizability to LMICs. The 6 LMIC-focused studies revealed barriers to implementation such as costs and infrastructure gaps but their restricted scope failed to demonstrate how these findings could apply to low-resource settings. The research faced limitations due to small participant numbers ranging from 82 to 133 and database restrictions which only included PubMed and Scopus. The review demonstrates how XR technologies can revolutionize healthcare education and practice despite existing research constraints. Research in the future needs to focus on studies from LMICs because these investigations will address current challenges regarding accessibility and cost-effectiveness and scalability to achieve equitable global adoption of immersive technologies in such countries.
Conclusion
This systematic review underscores the transformative potential of immersive technologies like XR, VR, and AR in healthcare, from enhancing surgical accuracy to democratizing medical education. However, their global promise remains unevenly distributed. There needs to be more research into better ways to use health technology to improve health around the world, though, before this promise can be fully kept. The road ahead looks both exciting and hopeful. It's possible to create a new era of healthcare that is better for everyone if we keep working hard and come up with new ideas. While we are on the brink of Industry 5.0, which holds even greater potential, further research is necessary to understand the challenges and opportunities ahead. One such challenge lies in the influence of health literacy on the patient–doctor relationship, healthcare access, and self-care, all of which are critical to improving health outcomes. This study shows the latest developments and challenges in this rapidly changing field in medical education as well. It also gives us a positive view on how new technologies may affect the future of healthcare. To fully achieve this promise, however, more research is needed to come up with better ways to use health technology to improve health results around the world. The road ahead is both exciting and hopeful. With continued hard work and new ideas, we can bring about a new age of healthcare and medical education that is more effective, accessible, and meaningful for everyone in most equitable way in LMICs.
Footnotes
Acknowledgments
Mohd Faizan Siddiqui (MFS) sincerely thanks Prof. Dr. Kozhobekov Kudayberdi Gaparalievich, Rector of Osh State University, for awarding the prestigious Dean’s Fellowship and for his generous support, including access to the university's archive gallery. MFS, AA, SJ, SV, LD, BA-H, AJ, FFB, HKAZ, JH, and REHC are grateful to Medical Student Advisory Board (MSAB) for providing the research infrastructure, access to IJCR research courses, regular mentorship, and sharing their constant guidance and support throughout this study.
ORCID iDs
Author Contributions
MFS: conceptualization, writing, illustration, reviewing, and editing; RK: supervision and validation; AA: original draft preparation and data curation; SJ: original draft preparation and review; SV: methodology, original draft preparation, and software; LD: original draft preparation and methodology; BA-H: original draft preparation and review; AJ: original draft preparation and data curation; FFB: original draft preparation and software; HK: original draft preparation and supervision; AJ: original draft preparation and editing; JH: original draft preparation and supervision; REHC: original draft preparation and data curation. Each author carefully read the entire manuscript, provided critical feedback, and actively participated in the revision process.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.