
Abstract
Background
Global health (GH) education is of growing interest and importance among pediatric trainees, including those pursuing pediatric critical care medicine (PCCM) training. Despite this, opportunities for formal GH training in US PCCM fellowships are limited.
Objective
This study aims to describe the GH curricula at US PCCM fellowships, barriers to GH education expansion, and fellow attitudes toward GH.
Methods
This study was a cross-sectional survey of program directors (PDs) and fellows from PCCM fellowships regarding currently available GH education at their institutions.
Results
We obtained data from 48 of 76 (63%) PCCM fellowship PDs and 60 PCCM fellows. Of responding programs, 9 (19%) offered a formal GH track, 28 (58%) offered GH opportunities but did not have a formal track, and 11 (23%) offered no GH opportunities. Programs that offered GH training had more fellows (P = .02) and GH faculty (P < .01) than those with no GH training. The most common GH-related offerings were sporadic GH lectures (76%), international clinical experiences (65%), and a GH-related scholarly project (51%). The significant barriers to the expansion of GH training were lack of funding, scheduling considerations, and lack of faculty mentorship.
Conclusions
GH education is available for PCCM fellows in the majority of training programs; however, this education is highly variable and often incomplete. While there is interest from both faculty and fellows in making this education more robust, significant institutional barriers persist. Addressing these barriers will be essential to promoting and enhancing GH education in PCCM fellowships.
Keywords
Introduction
There is a growing recognition of the importance of global health (GH) among medical trainees and pediatricians in the United States. 1 The Accreditation Council for Graduate Medical Education (ACGME) and the American Board of Pediatrics (ABP) have provided a comprehensive guide for GH education in pediatric training programs. 2 This training is particularly relevant in the field of pediatric critical care, where the burden of childhood mortality disproportionately affects low- and middle-income countries (LMICs). 3 Inadequate recognition of and care for critically ill children contributes significantly to this high mortality rate. 4 There are many challenges to the care of critically ill children in LMICs, including poor infrastructure, limited access to technology, and a scarcity of critical care-trained personnel. 5 Critical care for children is complex and resource-intensive, making it challenging to expand pediatric critical care and adequately train pediatric intensive care unit personnel. Only three formalized pediatric critical care medicine (PCCM) training programs exist in Africa. 6
In contrast, PCCM is one of the largest subspecialties for pediatric trainees in the United States, accounting for 14% of all pediatric subspecialty applications in 2024. 7 US-trained physicians are well-positioned to collaborate with institutions globally to address the disparity in childhood mortality. In addition, US physicians participating in international rotations report several benefits, such as increased comfort with clinical and diagnostic skills and increased confidence in physical examination skills. 8 However, the field of GH has historically had practices that asymmetrically benefit physicians in high-income countries.9,10 Formal GH training may help mitigate this unwanted consequence by teaching important foundational principles such as equity, fairness, and bidirectionality. PCCM fellowships have been slower than other pediatric subspecialties in providing opportunities for GH training. A study by Crouse et al in 2020 reported that only half of PCCM fellowship programs offered any GH training opportunities, and only one program offered a formal GH track. 11
In this study, we aim to describe the current landscape of GH education in PCCM fellowship programs. Additionally, we will identify critical barriers to the formation of GH tracks and assess the interest and preparedness of PCCM fellows to pursue careers in GH.
Methods
This study is a cross-sectional survey of program directors (PDs) and fellows from ACGME-accredited PCCM programs in the United States. We included all current PDs, associate program directors (APDs), and fellows at ACGME PCCM programs. PCCM trainees outside the United States were excluded. The survey was developed following a review of existing GH literature and the ABP and American Academy of Pediatrics (AAP) recommendations for GH education. The survey was customized separately to accommodate demographics and responses for faculty and fellows. Each survey consisted of four sections. Sections I and II pertained to personal and program demographics. Section III addressed the current state of the GH curriculum, while section IV addressed the barriers to the growth of GH curricula. The majority of questions were on the Likert scale and multiple-choice format, with one question providing an opportunity for open-ended comments. Investigators with expertise in GH, survey methodology, and diversity and inclusion reviewed the survey. The Emory University Institutional Review Board reviewed the survey questionnaires, and exemption was granted.
This electronic survey was distributed via email to PDs and program coordinators for all 76 ACGME-accredited pediatric critical care fellowship programs. Email addresses were obtained from the FREIDA Residency Program Database and fellowship program websites. The fellow survey was distributed to program coordinators by email, through a social media campaign, and via distribution through the AAP Section on Critical Care (SOCC) listserv. The survey was not distributed in GH-specific listservs to minimize selection bias. The survey was accessed via a Qualtrics© website link in the email. All survey responses were collected between February and December 2023.
This study categorized programs based on the presence of a Global Health Track (GHT), Global Health Opportunities (GHO), or no Global Health Opportunities. A program was designated as having a GHT if it provided the following: a longitudinal, global child health curriculum, international or domestic underserved experience, predeparture preparation and postreturn debrief, preceptorship during the elective experience, and a scholarly project. Programs classified as offering GHO provided some, but not all, of the components, while programs categorized as having no GHO did not offer any listed components. This classification system facilitated the identification and comparison of PCCM programs based on their GH offerings and structures. Programs were categorized into geographic regions based on the US Census Bureau tracks. 12 The reporting of this study conforms to the STROBE Statement guidelines for cross-sectional studies (Supplemental Table 1). 13
Statistical Analysis
Discrete choice responses were analyzed in SPSS. Continuous variables were compared using the Mann-Whitney U test, whereas categorical variables were compared using the Fisher’s exact test. A two-tailed p-value of <.05 was considered significant. Open-text responses underwent thematic analysis by the primary author and qualitative statistician. One fellowship program had two responses from the PD/faculty survey. These were considered duplicates and reviewed manually. Missing data were handled by excluding unanswered questions from specific analyses. If a respondent answered some but not all survey questions, their responses were included in analyses for the questions they completed, while missing values were excluded from the relevant analyses. Given the voluntary nature of the survey, imputation was not performed. Neither the abstract nor preprint for this study have been previously published.
Results
Program and Respondent Demographics
We received responses from 48 (63%) of the 76 PCCM fellowship programs. The majority of responders were PDs or APDs (45, 94%), with only three responses from other non-PD/APD faculty members. Programs were spread evenly across the United States, with 12 (25%) in the Northeast, 16 (33%) in the South, 10 (21%) in the Midwest, and 10 (20%) in the West (Table 1, Figure 1). This is similar to the distribution of all PCCM programs (Supplemental Table 2). Most responding fellowship programs had eight or fewer fellows (n = 26, 54%).

Distribution of GH Educational Opportunities Among US PCCM Fellowships. Shown is the Distribution of Programs with Global Health Tracks (Dark Green), Global Health Opportunities (Light Green), no Global Health Opportunities (Red), and Programs That did not Respond to the Survey (Light Gray).
Program Demographics.

Abbreviations: GH, global health; GHT, global health track; GHO, global health opportunities.
Faculty
The median number of faculty members within responding programs was 15 (interquartile range 11-20), of which a median of 1 faculty member devoted time to GH (interquartile range 0-2) (Table 1). The majority of faculty identified as white or Caucasian (77%), female (54%), and were born in the United States (83%). Faculty respondents had a median of 9 years in practice (interquartile range 6-17), and 78% reported having had some prior GH experience. The most common types of experiences were sporadic lectures (39%), elective rotations (40%), and volunteer work (47%). Seven (14%) had received an advanced degree or certificate in GH (Table 2).
US PCCM Faculty Responder Demographics.

Abbreviation: PCCM, pediatric critical care medicine.
We received nine open-ended responses from faculty respondents (Supplemental Table 3). The only recurring barrier was a lack of fellow interest, with three faculty members indicating that this was a significant barrier.
Fellows
At the time of this study, an estimated 618 fellows were in US PCCM training programs. 14 A total of 60 fellows responded to the survey (Table 3), accounting for an estimated 10% of all PCCM fellows. An exact response rate could not be calculated as we could not ascertain how many fellows received the survey. The majority of respondents identified as white/Caucasian (75%), female (67%), and were born in the United States (80%). This is consistent with the previously reported racial, ethnic, and gender distributions of PCCM fellowships. 15 Year of fellowship training was evenly distributed between the first year (23%), second year (28%), and third year of fellowship (33%), with 15% of responding fellows completing a fourth year. Thirty-six (63%) fellows reported having had some prior GH experience, which included GH lectures (53%), international clinical experiences (42%), and domestic GH experiences (25%). Before fellowship, 22 (37%) fellows had been a part of a longitudinal GH curriculum. Eleven (18%) fellows participated in a formal GHT (Table 3). Experiences before fellowship were not limited to residency and could have occurred at any point before beginning fellowship. While 31% of responding fellows expressed an interest in pursuing a career in GH, 13% feel that they will be prepared to do so. Eleven (17%) responding fellows reported having had a GH experience during their PCCM fellowship (Table 4).
US PCCM Fellow Demographics.
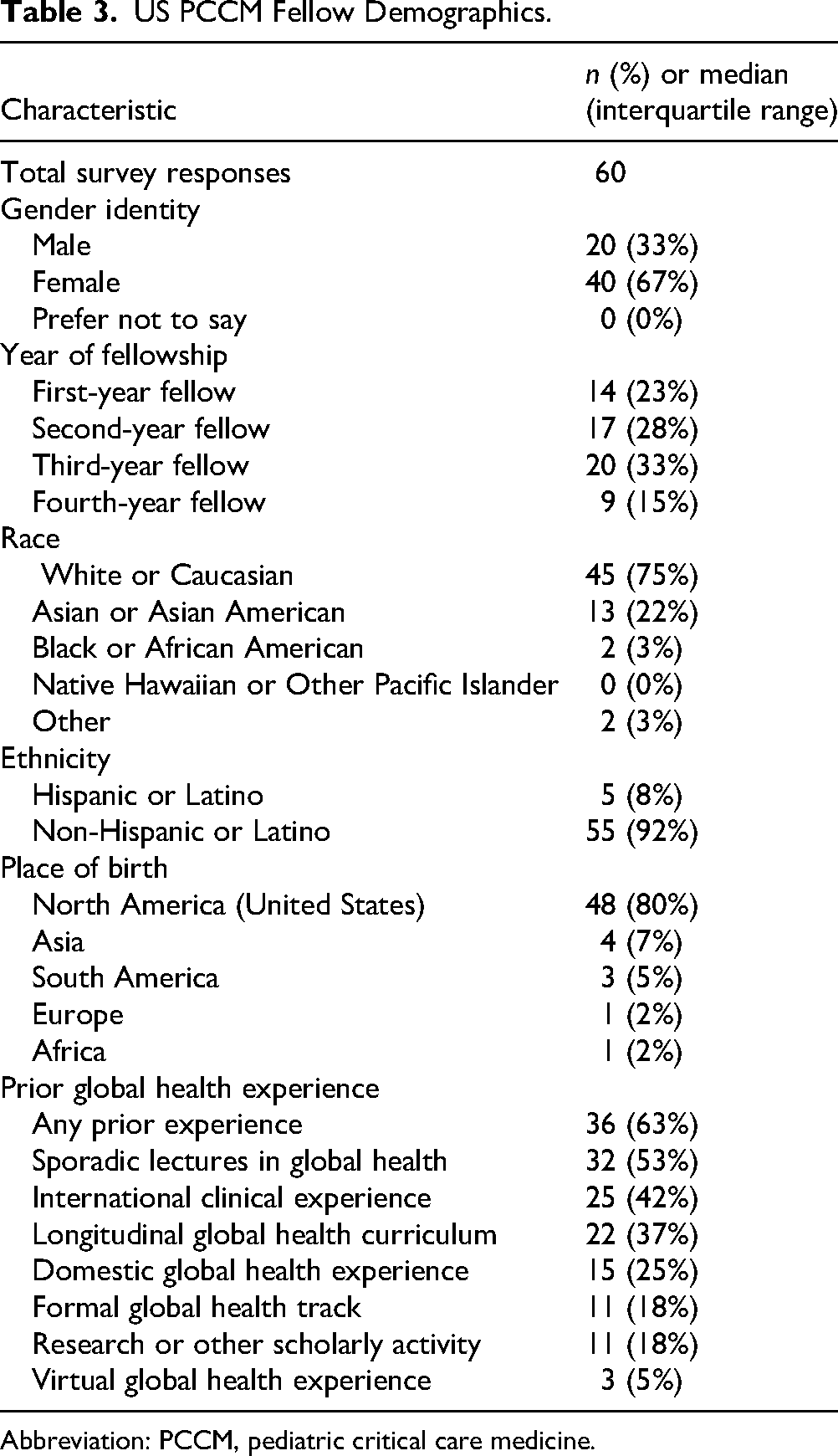
Abbreviation: PCCM, pediatric critical care medicine.
GH Education in US PCCM Training Programs: Fellow Responses.

Abbreviations: PCCM, pediatric critical care medicine; GH, global health.
We received 12 open-ended responses from fellow respondents (Supplemental Table 3). Six fellows reported little to no structured opportunities, with one stating, “There is virtually no global health education at my program.” Another fellow expressed disappointment, noting, “We don’t have global health education or opportunities, which is unfortunate because I think it would be incredibly beneficial for us as fellows.” Three fellows noted that participation in GH would require significant independent effort. As one fellow remarked, “I probably could have arranged an experience, but it would have been a lot of work on top of the traditional burdens of fellowship.” Responses did not reach thematic saturation.
Global Health Education Opportunities
Thirty-seven responding programs (75%) offered GH training opportunities. However, only nine programs (19%) had a formal GHT (Table 1). When compared to programs with no GHO, programs with GHT had a higher number of fellows (14 vs 3, P = .01), faculty (20 vs 10, P = .03), and GH faculty (2 vs 0, P < .01) (Table 5). Among those that offer GH education, most programs offered sporadic GH lectures (n = 28, 76%). Several offered an international clinical experience (n = 24, 65%) or the opportunity to participate in a GH-related scholarly project (n = 19, 51%). Fewer programs reported having virtual GH opportunities (n = 7, 16%) or a domestic GH experience (n = 6, 16%), and only four programs (8%) had an organized longitudinal curriculum (Table 6). Of programs that responded to this question, the Division of PCCM was the most common organizer of GH education (n = 5, 14%), followed by the Department of Pediatrics (n = 3, 8%). Twenty-one programs (44%) reported establishing international partnerships, but only 9 (19%) participated in bidirectional exchanges. The median number of partner sites was 2 (interquartile range 1-4).
Faculty and Fellow Demographics According to Program GH Offering.

Abbreviations: PCCM, pediatric critical care medicine; GH, global health.
PCCM GH Educational Structure Among Programs with GHT and GHO.

Abbreviations: PCCM, pediatric critical care medicine; GH, global health; GHT, global health track; GHO, global health opportunities; PCCM, pediatric critical care medicine; GME, Graduate Medical Education.
Primary funding for salary and benefits for fellows participating in GH opportunities was most commonly available through standard Graduate Medical Education (GME) funds (salary and benefits) (n = 34, 92%). Few programs received salary and benefits support from division discretionary funds (n = 2, 5%) and external grants (n = 1, 3%). Sources of funding for fellow travel and accommodation when participating in a GH away rotation are listed in Table 6. Seventeen programs (46%) report that fellows utilize personal funds to support these costs. Eight programs (22%) did not know the funding source for fellows participating in global away rotations.
Global Health Education Barriers
Faculty and fellows differed when asked what the perceived barriers to the expansion of GHO were. According to faculty, the most extreme barriers to the expansion of GH education were travel and accommodation logistics, lack of faculty mentorship, and scheduling concerns (Figure 2). While lack of fellow interest ranked low on the faculty quantitative assessment, it was mentioned in the open-ended responses. According to one PD, “None of our fellows have expressed a GH interest to date.” Fellows ranked research obligations and lack of interest from faculty and fellows as the most significant barriers. While lack of interest from institutions, scheduling, funding, and faculty mentorship ranked low, there was a higher percentage of fellows who were unsure of the impact of these on GH education. In the open-ended responses, lack of institutional support was the most commonly mentioned barrier, with one fellow stating, “Participation in GH experiences would have taken much of my personal time and money.”

Barriers to Expansion of GH Training. Shown are the Perceived Importance of Major Barriers to the Expansion of Global Health Curricula According to the Program Directors (A) and Fellow (B) Respondents.
Discussion
Our study is the first to characterize GH training opportunities in US PCCM fellowship programs. While most programs offer some form of GH education, there is significant variability in the content and type of GHO available for trainees. Additionally, we assessed faculty and fellow perspectives on barriers to GH education and the perceived importance of GH education within fellowship training.
Our findings are consistent with the study by Crouse et al, which reported that nearly half of all pediatric subspecialty fellowships offer GH training, but the offerings are variable. 11 Programs that offered a complete GHT were more likely to be larger, but no differences in geographic distribution were observed.
Several barriers to expanding GH efforts were identified. Both faculty and fellows identified lack of faculty engagement as a central concern, which is consistent with previously published data. 16 Even though most faculty respondents had some prior GH training or experience, the availability of mentors dedicated to GH education and supervision within PCCM programs remains low, with a median of 1 faculty member within the responding programs identified as dedicating time and effort to GH. We did not explore the barriers to faculty participation in this study. However, a prior study by Patel et al identified funding limitations, lack of protected time, and family obligations as significant barriers. 17 Without adequate faculty mentorship, participating in GH for trainees is challenging. 11 Faculty relationships are the cornerstone of building global partnerships and facilitating effective GH opportunities for trainees. Adequate supervision by a trained faculty mentor is essential to ensure ethically responsible scholarly work that is safe and mutually beneficial to all partners.
Faculty and fellows identify financial and time constraints as barriers. These findings mirror that of North et al, which identified a lack of dedicated funding sources as an essential barrier to offering GH training opportunities in adult pulmonary critical care fellowships. 18 Financial support for faculty travel expenses and the ability to dedicate time to GH initiatives were highlighted barriers. Over one-third of programs require fellows to bear travel and accommodation expenses for GH experiences. Seeking solutions such as leveraging GME funds or securing external grants may help alleviate financial barriers and promote equitable access to GH opportunities. Additionally, efforts to secure institutional support and resources are essential to fund GH initiatives sustainably within PCCM fellowship programs.
The demanding nature of PCCM training, characterized by long work hours and clinical responsibilities, poses challenges to integrating GH experiences into fellowship training schedules. PCCM fellows are often required to work clinically on nights and weekends during research blocks, which makes scheduling longitudinal GH experiences challenging. 19 In our study, faculty respondents ranked scheduling concerns as an essential barrier limiting the availability of GH opportunities. In programs that did offer GH education, the most common ways of accounting for this time were through elective time (41%) and dedicated research time (34%). Programs may consider implementing more flexible scheduling options, such as blocking time for elective rotations or call-free research time, to facilitate fellow engagement in GH activities without compromising clinical training requirements.
Additionally, utilizing virtual technologies like Zoom, Microsoft Teams, and Webex may offer innovative solutions to overcome logistical and geographic barriers and facilitate remote participation in GH initiatives. Virtual learning has been successfully used to facilitate GH education for medical trainees during the COVID-19 pandemic.20–22 It offers a low cost and time-flexible way for trainees to engage in GH while fostering the development of bidirectional partnerships. Domestic GH experiences or “local-global” efforts also offer a viable alternative to international travel. Trainees who participate in local experiences such as immigrant and refugee health clinics gain cultural competency, advocacy skills, and the ability to care for marginalized communities. Expanding opportunities for trainees to optimize healthcare for vulnerable populations within their communities can effectively integrate GH education into training programs. 23
When asked about long-term career plans, there was a discrepancy between fellows’ interest in pursuing a GH career (31%) and their preparedness for a GH career (11%). This is similar to other surveys of fellows in other pediatric subspecialty trainees. 24 This discrepancy highlights the need for more comprehensive training and mentorship. Interestingly, the availability of a GH education opportunity did not play a role in the fellow ranking of fellowship programs. This differs from recent studies showing that medical students consider GHO in ranking decisions. 25 This may be due to the relative sparsity and increasing competitiveness of PCCM fellowships and the earlier identified barriers in GH training, such as uncertain career development opportunities and challenges surrounding funding and protected time.
Our study has several significant limitations. Only 64% of fellowship programs, based on PD or faculty responses, responded to our survey. Additionally, we only received 60 responses from PCCM fellows, representing a tiny proportion of all PCCM fellows currently in training in the United States. The low response rate precludes some analyses. As this survey was voluntary, the demographics of individuals and programs that responded may differ from those who did not, leading to a biased sample that may not accurately represent the entire population of US PCCM programs and fellows. Sample bias of self-selection may have skewed the results in favor of respondents with a greater interest in GH. Among programs offering a GHT and GHO, this paper does not provide detailed information regarding the structure and content of their curricula. Yet, it would add valuable information for programs intending to develop GH education. Additionally, this study did not evaluate the barriers faculty encountered to developing their GH careers and dedicating time and effort to GH education. Due to the paucity of open-text responses, data saturation was not reached in our qualitative analysis.
Despite these limitations, we believe we captured a nationally representative sample of PCCM PDs and faculty. In this study, we described how PCCM fellowships currently organize and fund their GH training programs. We established interest among fellows and PDs in strengthening GH training for fellows. While significant barriers remain, our findings highlight opportunities for growth in GH education within PCCM fellowships. This lays the groundwork for programs looking to expand their GH offerings and eventually establish more robust GHOs or GHTs.
Conclusion
This study provides an important overview of the GH training opportunities within US PCCM fellowship programs, as well as barriers to fellow engagement in GH. Our study highlights the variability in GH education opportunities. It brings attention to the need for deliberate efforts to standardize and strengthen GH education within PCCM fellowship programs by increasing support for faculty engagement, leveraging institutional and divisional funding, and carving out protected time for faculty and fellows. By addressing these barriers to participation in GH and leveraging opportunities for collaboration and innovation with global partners, we can enhance the training of the next generation of pediatric intensivists to improve the inequities in critical care delivery for children worldwide.
Establishing formalized GHT, enhancing mentorship opportunities, and promoting interdisciplinary collaborations are crucial steps toward equipping trainees with the knowledge, skills, and resources necessary to navigate GH.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251343181 - Supplemental material for Global Health Education in US Pediatric Critical Care Medicine Fellowships
Supplemental material, sj-docx-1-mde-10.1177_23821205251343181 for Global Health Education in US Pediatric Critical Care Medicine Fellowships by Adeolu Aromolaran, Brittany Murray, Cynthia Sinha, Zhulin He and Mary L. DeAlmeida in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251343181 - Supplemental material for Global Health Education in US Pediatric Critical Care Medicine Fellowships
Supplemental material, sj-docx-2-mde-10.1177_23821205251343181 for Global Health Education in US Pediatric Critical Care Medicine Fellowships by Adeolu Aromolaran, Brittany Murray, Cynthia Sinha, Zhulin He and Mary L. DeAlmeida in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205251343181 - Supplemental material for Global Health Education in US Pediatric Critical Care Medicine Fellowships
Supplemental material, sj-docx-3-mde-10.1177_23821205251343181 for Global Health Education in US Pediatric Critical Care Medicine Fellowships by Adeolu Aromolaran, Brittany Murray, Cynthia Sinha, Zhulin He and Mary L. DeAlmeida in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The authors appreciate the American Academy of Pediatrics Section of Critical Care for their support in distributing the survey and the program directors and fellows who provided survey responses.
Author's note
Adeolu Aromolaran is currently affiliated with Department of Pediatrics, Rutgers Robert Wood Johnson Medical School, New Brunswick, NJ, USA.
Ethical Considerations
This study was reviewed by the Emory University Institutional Review Board (STUDY00004755), and the exemption was granted on 10/20/2022.
Author Contributions
Adeolu Aromolaran conceptualized and designed the study, created the survey, collected data, carried out initial data analysis, and drafted the manuscript. Mary L. DeAlmeida conceptualized and designed the study, drafted the initial manuscript and critically reviewed, and revised the manuscript. Zhulin He and Cynthia Sinha advised on survey design and performed data analysis. Brittany Murray advised on survey design and critically reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.