
Abstract
Formalized debriefing after travel is a critical component of medical global health elective rotations (GHERs), but evidence-based processes are lacking, resulting in significant variability among institutions. There is increasing attention to the need for learner debriefing that can address both emotional and cognitive components of their experience. Our multi-institution workgroup reviewed best practices in debriefing simulation-based learning and acute clinical events, the role of narrative reflective writing on learning and professional identity formation, and the unique components of global health debriefing. Utilizing Kern's six-step process of curriculum design, we developed a comprehensive curriculum to support implementation of rigorous post-rotation debriefing in global health education programs. The resulting Understanding Needs in Post-rotation Activities and Coaching Kit modules consist of peer-reviewed activities to address five critical elements of a robust GHER debriefing program. These include institution/organizational structure, learner debrief preparation, conducting the debriefing session (addressing emotional and cognitive components), facilitating mental health support, and bringing experiences back to partner institutions. We outline the piloting process and next steps for curricular evaluation.
Introduction
Formalized debriefing after travel is a critical component of medical global health elective rotations (GHERs), but evidence-based processes are lacking. From an educational perspective, there is increasing attention to the need for learner (inclusive of pre-medical students, medical students, resident physicians, subspecialty fellow physicians, other graduate students, early career faculty, nurses, allied health professionals, etc.) debriefing that can address emotional, cognitive, and logistic components that are unique to GHER. While guidelines support debriefing and many institutions have the expectation that debriefing follows GHER, there is considerable variability regarding the structure, processes, and resources used.1–3 There is a paucity of data regarding outcomes or impact of debriefing in this setting.
Multi-institutional collaborative efforts are an effective method to design and implement curricula that can address gaps in global health education.4–6 Our multi-institutional workgroup, The Midwest Consortium of Global Child Health Educators, is described elsewhere. 7 Members of the Consortium and affiliate colleagues from four separate institutions envisioned a toolkit of resources to support all aspects of the post-GHER period, spanning administrative practices to faculty training in facilitating debrief conversations. We followed Kern's six-step process for curriculum development to address this need for comprehensive debriefing. 8 Here we describe the unique components of debriefing GHER, critical evidence-based concepts integrated into our materials, and the step-by-step iterative process to develop this novel curriculum. Our final product, Understanding Needs in Post-rotation Activities and Coaching Kit (UNPACK) is unique and distinct from other existing and frequently used global health educational resources. UNPACK's focus on debriefing complements existing Consortium educational resources including simulation learning (SUGAR), procedural skills (PEARLS), pre-departure training (S-PACK), and immigrant and refugee health (I-PACK), among others.4–6,9–12
What Makes Debriefing GHER Unique
The experiences associated with GHER are distinct from other clinical debriefing scenarios and warrant special consideration. GHER are generally weeks or even months in duration, and it may not be feasible to debrief these experiences “in the moment” for both logistical and emotional reasons. Pre-departure preparation is increasingly expected before participating in a GHER and generally address logistical (eg, vaccine requirements) as well as clinical and cultural components of practice in a low-resource setting.4,13–15 Simulation is often included in pre-trip preparation, covering common scenarios that learners may not have previously experienced, such as pediatric death in a low-resource setting.4,16 Despite the best preparation, real-world experience impacts all learners differently, particularly with the additional stressors of being away from home. 17 Ensuring that learners have the opportunity for structured debriefing can contribute to positive learning experiences and ongoing professional identity formation.
Debriefing after GHER should address clearly articulated goals, and cover logistical, cognitive, and emotional aspects of the rotation3,18 (Figure 1). Existing literature supports clear themes that often emerge as discussion points during debriefing for those who participate in GHER. These include but are not limited to: patient death, the perceived benefits of the GHER, the culture shock that accompanies a learner both in their host environment and upon return with reacclimation into their native one, the emotional impact of certain events, and the awareness of scope of practice and difficulty setting boundaries during the GHER.4,14,16,19–21 These stressors may generate or exacerbate mental health concerns for learners engaging in GHER. Faculty familiar with recognizing these unique themes and equipped with a framework for navigating between the cognitive and emotional debrief components can guide their learners to reflect productively on the experience in a way that supports professional development and mitigates harm.
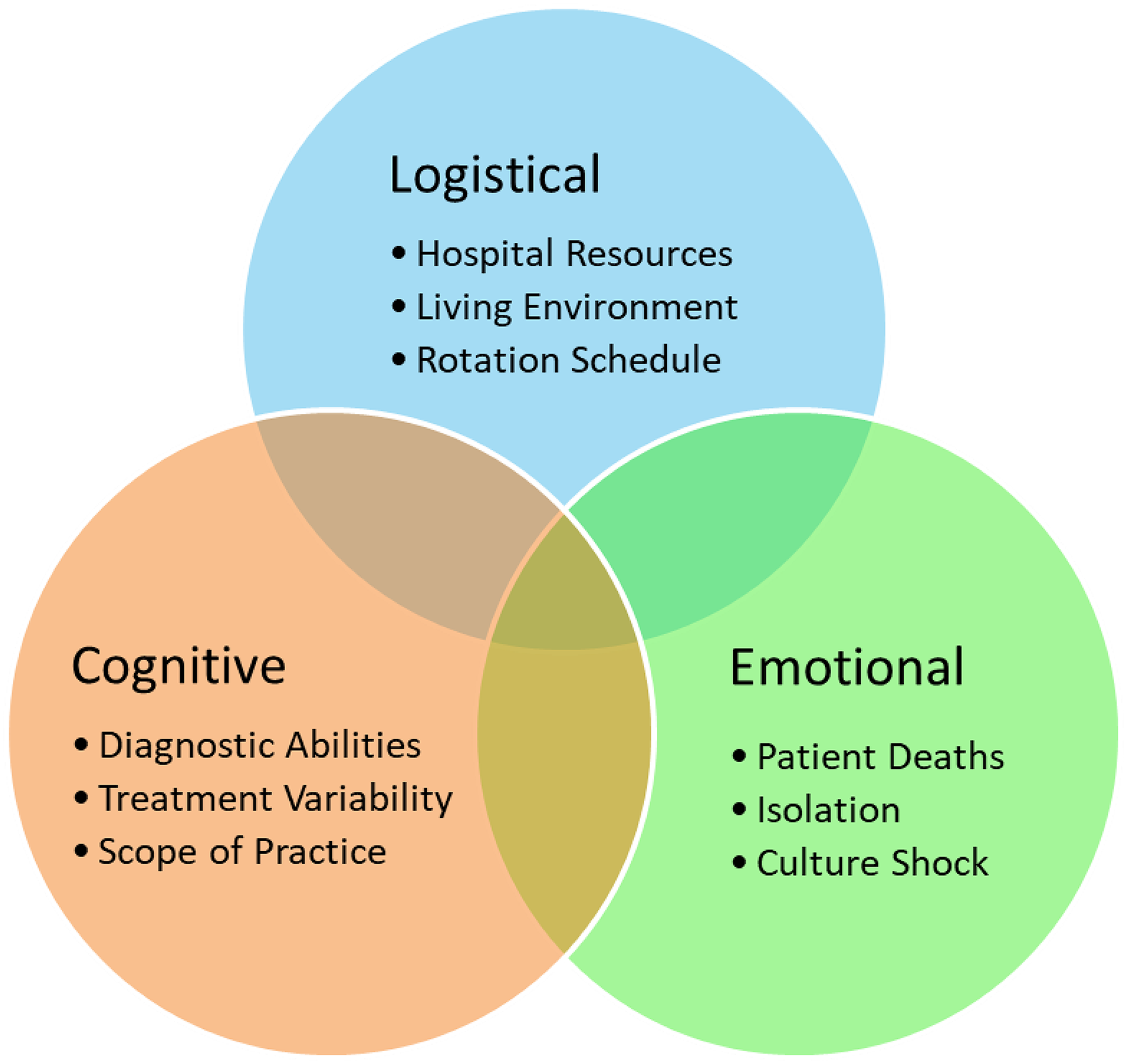
Debriefing GHER Should Include Structured Discussion within the Following Domains: Rotation Logistics, Cognitive Differences, and Emotional Perspectives. GHER, Global Health Elective Rotation.
After debriefing a GHER, there remain several components necessary on the individual and institutional level to support learners. On the individual level, debriefing by itself is not a sufficient intervention to address mental health concerns—it is critical to connect learners identified as struggling with post-GHER-related impacts to appropriate professional mental health support.17,22,23 On an institutional level, academic centers should aim to uphold principles of decolonization and reciprocal partnership with host institutions rather than perpetuate unilateral systems. Best practices support co-creating GHER goals and curricula, bidirectional exchange, and integrating mechanisms to communicate with host institutions about learner experiences and impact (both positive and negative).24–26 Feedback from all individuals involved in the partnership should be sought in culturally appropriate ways, recognizing the power dynamic that often exists between academic institutions and host institutions in low- and middle-income countries. Both soliciting and providing actionable bidirectional feedback for all participants involved in GHER are key elements to identify and maintain priority areas for the partnership. There should be ample opportunities to provide both real-time, summative, and transparent feedback regarding how this feedback will be used, including specific follow-up plans for changes and actionable elements.
At present, there are no unifying curricula that bring together best practices and recommendations for debriefing that address the distinct concerns of learners returning from GHER. Our UNPACK modules offer a toolkit for global health educators to implement a post-rotation process that builds upon foundational debriefing and narrative writing principles and strategies. It addresses unique considerations in the global health context and moves beyond the debriefing conversation to address learner mental health and equity with partner institutions to create a comprehensive GHER debriefing program.
Foundational Debriefing Principles
Debriefing as a facilitated reflective conversation in the context of experiential learning distinguishes it from other processes such as feedback. 27 There exists an extensive body of literature on debriefing in health professions education, variably addressing the structure, content, audience, and goals of the process. These draw from multiple disciplines, including medicine, nursing, paramedicine, service volunteers, and simulation sciences. For our purposes in debriefing after GHER primarily for resident physicians, we considered the following foundational literature on relevant process and content.
Process
Much of the current debriefing literature focuses on debriefing singular simulation-based learning opportunities27–32 or specific clinical situations in which a critical and often emotionally charged event occurred.4,33–39 Colleagues in the fields of nursing, social work, and paramedicine have published additional perspectives on the role and impact of debriefing in promoting resiliency and self-reflection.30,34
A variety of debriefing methods have been described: utilizing written materials versus only verbal discussion, one-on-one debriefs versus group debriefs, and formal scripted debriefs versus informal chats.
From the clinical and simulation-based learning literature, key components to consider in deciding on a particular workflow include optimal debrief timing, methods of facilitation, conversational structures, and other important process elements.27,28 Overall, many different models of simulation and clinical debriefing exist, and there are different but often overlapping ways to articulate the phases and elements of effective debriefing.
Content
The content of a debriefing session is unique to the simulation or scenario. A recent literature review and concept analysis on clinical debriefing identified five E's as key attributes to include: educated/experienced facilitator, environment, education, evaluation, and emotions. 39 On a conceptual level, there is often a complex interplay between cognitive and emotional content of a debrief conversation, and nuance in how to address them ie, focusing on medical decision-making and a more detached analysis versus a focus on the ethical, personal, and social-emotional response to the case. The approach and needs for each component are necessarily distinct. Specific to our intended audience, Haq et al 18 conducted a Delphi study in 2024 which rated best practice components for debriefing resident physicians after GHER. Twelve components were deemed essential, including assessing learner well-being and coping skills, ethical concerns, supporting reflection of the experience, and the need to provide mental health support for those experiencing distress. 18
Established educational theory emphasizes the importance of trained facilitators in supporting effective reflection and debriefing. Facilitators must both challenge and foster the thinking behind reactions and practices, acting as a guide rather than lecturer. 28 A wide body of literature details core skills of facilitators that are necessary for effective debriefs, including ensuring the psychological safety of learners, asking open ended questions, and allowing for learner self-assessments.27,28,38,40 Both learners and facilitators are often faced with difficult-to-debrief situations, including but not limited to sudden changes in clinical conditions, unanticipated clinical outcomes, interpersonal conflict, and the limitations of technology and available interventions. 14 Frameworks exist to help facilitators in guiding difficult discussions and attending to emotions,29,38,41,42 though they are often specific to the clinical simulation scenario and with little data to support impact on outcomes. 43 A more generalizable toolbox by Grant et al outlines communication strategies and reactive skills for facilitators to address challenging debriefs (whether for learner or situation-related factors). 29 These frameworks and tools have strong potential to inform a cohesive approach to navigating the debriefing conversation with learners after GHER.
The Role of Reflective Narrative Writing
There is abundant evidence that cultivating reflective writing as a form of processing with appropriate feedback can develop curiosity and self-inquiry and engage medical learners in their professional growth.44–46 Learner engagement with such methods may be slow at the beginning and depends on effective engagement to increase uptake and the consistency that results in the best outcomes.47,48 In GHER, these methods are increasingly being harnessed.21,49,50 While there are multiple reflective writing frameworks described, best practices support a structured, progressive approach to invite deeper analysis of behavior especially for novices such as the “what, so what, now what” model or the 4 F's of Active Reviewing. 51 Additionally, frameworks exist for faculty to review and give feedback on narrative reflections.45,51,52 Others have supported incorporating reflective writing into GHER debriefing as an impactful learning tool and way to identify struggling learners.17,50,53
Curriculum Design Using Kern's Six-Step Process
Based on these foundational principles and practices, members of the Midwest Consortium set out to create a comprehensive curriculum to support implementation of rigorous post-GHER debriefing in global health education programs. Members met every 2 weeks to articulate goals and objectives, develop educational materials, and make iterative changes based on feedback solicited from peer educators (Figure 2). We incorporated existing literature on the utility of narrative reflective writing in professional development and debriefing following simulation-based learning and clinical events to develop five modules. The following steps outline key aspects of our curriculum design using Kern's six-step process.

Timeline of Processes Employed to Develop, Implement, and Evaluate the UNPACK Debriefing Curriculum. UNPACK, Understanding Needs in Post-rotation Activities and Coaching Kit.
Step 1 - General needs assessment:
Our group reflected on our own institutional processes for debriefing learners after GHER, and considered the body of literature outlined above. Based on these, we articulated the need for a standardized, structured approach to debriefing for learners after GHER that could address the nuances of these unique clinical experiences. Second, we recognized the potential roles of narrative reflective writing and that of well-trained faculty facilitators in making meaning from clinical experiences.
Step 2 - Targeted needs assessment:
To pursue a more targeted needs assessment, we invited members of the Midwest Consortium who attended our annual meeting to complete a Qualtrics survey on their current debriefing practices including faculty preparation, learner needs, and institutional priorities for post-GHER debriefing. The following reflects the notable highlights of the 13 respondents’ perspectives, spanning all seven member institutions.
Results from this informal polling (See Supplemental Table 1) demonstrated that all Midwest Consortium members offered post-rotation debriefing, with 85% making it mandatory. The timeframe to complete a debrief was widely variable: notably 23% expected to conduct the debrief within 1-2 weeks of return, 38% within 2-4 weeks, 15% within 4-8 weeks, and 8% before the end of the academic year. Over two-thirds of respondents indicated their debriefing was unstructured, and only one-third of faculty had received formal training in conducting debriefs. Priorities to address during the debriefing were identified as, in decreasing order of importance: a) mental health/ emotional well-being/culture shock, b) ethics/equity/colonialism, c) feedback to host sites, d) medical knowledge/clinical care, e) logistical concerns, and finally, f) professional development.
The majority of concerns, whether about learner mental health and well-being or host site issues, were reported to leadership on an ad-hoc basis, without established feedback loops. Those who completed the survey did report a range of possible mental health supports when a concern was identified, from Graduate Medical Education (GME) office, residency-program-specific, and community resources, but even the most frequently reported (GME-based) was only “readily available” to 63% of respondents. When reflecting on how well their institutions conduct post-rotation debriefing, only 33% reported “well” and 67% reported “neutral.” Based on these findings, we identified five major areas to tackle in our debriefing curricula.
Step 3 - Goals and objectives:
Our resulting UNPACK modules address five GHER debrief processes: institution/organizational structure, learner debrief preparation, conducting the debriefing session (addressing emotional and cognitive components), facilitating mental health support, and bringing experiences back to partner institutions (see Table 1).
The 5 UNPACK Modules.
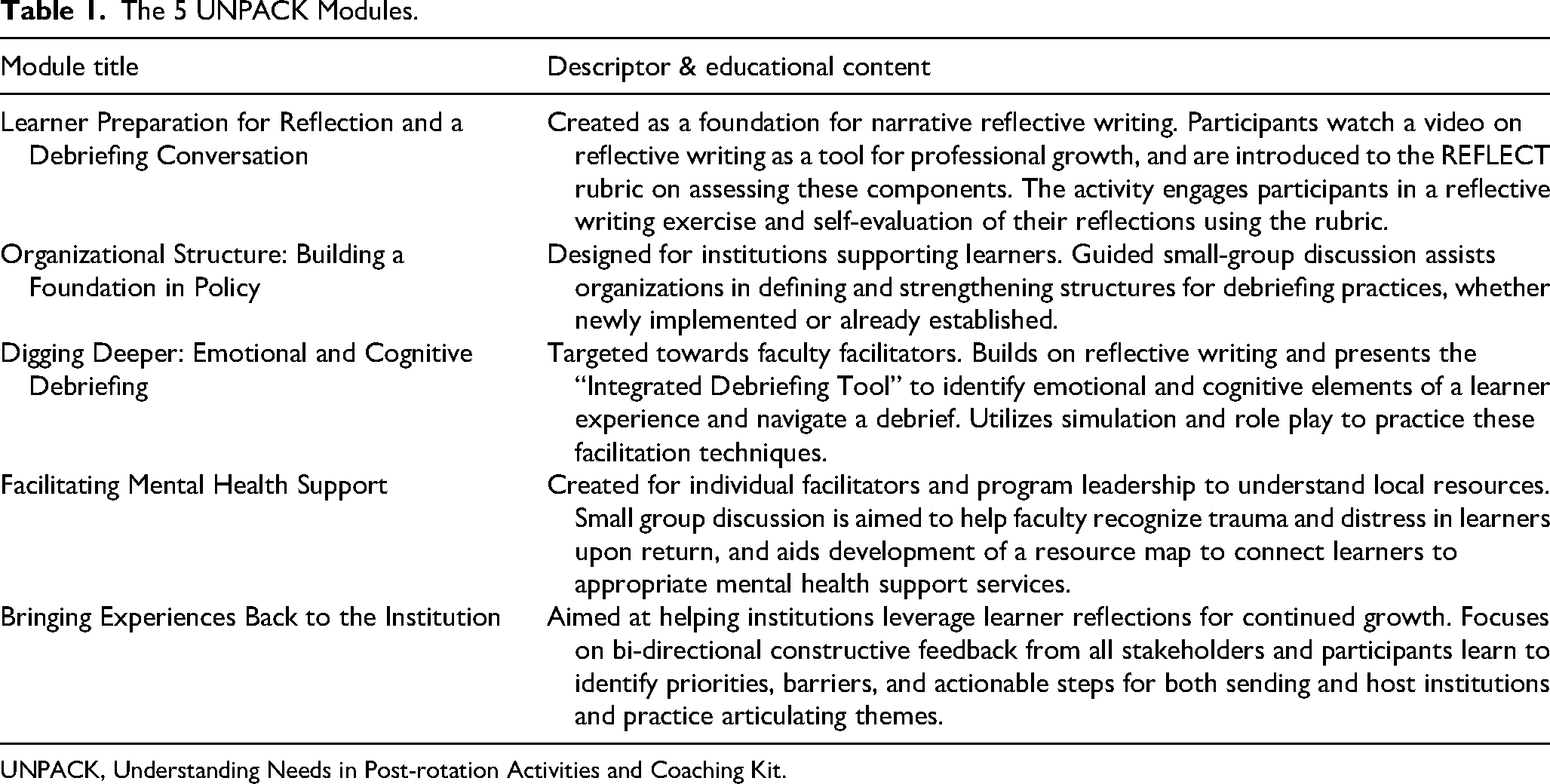
UNPACK, Understanding Needs in Post-rotation Activities and Coaching Kit.
Each module in the curriculum incorporates components from GHER debrief processes among the authors’ academic institutions and the aforementioned foundational literature/expert recommendations, debriefing best practices in general, and narrative reflective writing in healthcare professional development. The modules aim to consider different stakeholder needs and perspectives when a GHER concludes: those of both sending and host global health program leaders/administrators, faculty who facilitate debriefs, and learners themselves.
We intend to maximize the benefits of the learner GHER debriefing process by incorporating narrative reflective writing into our structured debriefing curriculum, which provides facilitators with a powerful tool to gain learner insight. First, by introducing the components of narrative reflective writing as one piece of a larger debriefing strategy and encouraging learners to engage in this self-analysis, we hope to promote this personal development practice. Facilitators of the debrief can cue into and highlight key themes from these reflections with learners. Even if only utilized once during the debrief, we believe the evidence supports this methods’ ability to foster analysis of significant events. For those enthusiastic adopters, it could be used to intentionally foster professional growth throughout their career. Second, using their understanding of the components of critical reflective writing and themes unique to GHER, faculty facilitators can effectively engage learners during a debriefing discussion by generating reflective questions based on the learner's own words. Narrative writing can be a tool faculty leverage to “come prepared” to meet learners where they are at in the debrief, promoting deeper reflection, analysis, and meaning-making from their experience.
Step 4 - Educational strategies:
Our curriculum consists of modules that can be conducted either by individuals or in small groups, in person or entirely virtually. Modules stand independently and each take approximately 2-3 hours to complete. Modules can be utilized by programs who are just starting GHER as well as by programs with longstanding global partnerships looking for ways to strengthen their debriefing processes or provide additional faculty development. As a complete package, this kit is designed to support training programs to create a comprehensive debriefing process to help returning learners unpack their experience. We solicited peer feedback from Midwest Consortium members at multiple points of curriculum development to ensure that key competencies were addressed.
The educational strategies incorporated into the modules are variable and include small group discussion, reflective writing activities, guided self-evaluation using established tools, and simulation/role-play to reinforce new frameworks and actively practice communication skills (see Table 1). The modules are specifically designed to provide tools for facilitators to establish and support learner psychological safety. Debriefing conversations are led by the learner with the facilitator soliciting the learner's perspectives, which allows the learner to draw conclusions and discover common themes within their own experiences and reflections.
Step 5 - Implementation:
The target audience for our curriculum are global health educators (clinicians and administrators) who would be able to utilize the individual modules to improve the debriefing process at their own institutions. We are conducting an initial introduction and training for how to utilize the curriculum at the 2025 annual Midwest Consortium meeting. Piloting key components of the curriculum with seasoned global health educators will help to further refine curricular elements and reveal additional opportunities for growth and clarity before introducing the curriculum to a more general audience. After this pilot session, the entire curriculum will be made freely available through the established online portal for our Midwest Consortiums’ global health educator curricular suite (sugarprep.org). We will subsequently encourage implementation by offering training workshops at Midwest Consortium pilot sites and at larger forums outside our multi-institution workgroup. These workshops will provide additional guidance and hands-on practice on how to utilize the modules for further programmatic development at individual institutions. Individual institutions can determine how best to implement these modules to meet their specific needs, whether to develop new practice or improve and build upon current structures.
Step 6 - Concepts for Evaluating the Curriculum:
A formal survey will be completed by participants at the completion of each pilot/introduction workshop. The survey will assess global health debriefing experience of pilot users, feedback about specific elements of the curriculum, and plans for changes in current debriefing practice and implementation of the curriculum at respondent's institutions. Follow-up surveys after initial introduction to the curriculum will evaluate interim experiences with implementation and utilization of the curriculum at individual institutions, including which modules were implemented, the time required to learn and then implement the modules, the number of faculty members who participated in faculty development modules, and the changes made to systems and structures following implementation of the modules. Ideally, sites that implement the modules focused on facilitator training and learner support would investigate the real-world impact of this curriculum. This would include studying the development of faculty knowledge, skills, and attitudes about debriefing pre- and post-implementation, or soliciting learner feedback on the debriefing process as an educational and meaning-making aspect of their GHER.
Conclusion
GHER are distinct from other experiences in medical training. These experiences require dedicated and regular review of both institutional operations and faculty preparation for post-rotation debriefing to address learners’ emotional and cognitive learning. We used Kern's six-step process of curriculum design to develop UNPACK, a comprehensive toolkit to address these unique needs. UNPACK harnesses narrative reflective writing practices and gives structure to facilitated debriefing sessions in order to provide learners with opportunities to effectively unpack their experiences. UNPACK is currently being piloted at Midwest Consortium sites and will soon be available on Midwest Consortiums’ global health educator curricular suite. Piloting key components of the curriculum with seasoned global health educators will help to further refine curricular elements and reveal additional opportunities for growth and clarity before broader dissemination. Subsequent efforts to study uptake, satisfaction with and perceived value of the curriculum by both learners and faculty, and learner impact will lead to continued improvement of this educational endeavor.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251414783 - Supplemental material for Time to UNPACK: Understanding Needs in Post-Rotation Activities and Coaching Kit—A Global Health Elective Rotation Debriefing Curriculum
Supplemental material, sj-docx-1-mde-10.1177_23821205251414783 for Time to UNPACK: Understanding Needs in Post-Rotation Activities and Coaching Kit—A Global Health Elective Rotation Debriefing Curriculum by Emilee Flynn, Stephen Selinsky, Jessica Landry, Emily Danich, Lisa Umphrey, Kristin Van Genderen, Mounika Muttineni and Adriana Dhawan in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
None
ORCID iDs
Ethical Considerations
Polling was determined non-human subjects research by the University of Minnesota Institutional Review Board, STUDY00020005
Consent to Participate
Not applicable
Consent for Publication
Not applicable
Author Contributions
All authors conceived and designed the work, supported the curriculum development and implementation, and contributed to revisions of the manuscript. EF and AD wrote the first draft of the manuscript and managed all revisions. All authors critically reviewed and approved the final version of the manuscript as submitted.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.