
Abstract
Background:
Sex- and gender-based medicine (SGBM) should be a mandatory part of medical education. We compared the quantity and quality of sex- and gender-related content of e-learning materials commonly used by German and American medical students while preparing for national medical examinations.
Methods:
Quantitative, line-by-line analysis of the preparatory materials AMBOSS 2017 and USMLE Step 1 Lecture Notes (2017) by KAPLAN MEDICAL was performed between April and October 2017. Subjects were allocated to one of the three main fields: clinical subjects, behavioral and social science, and pharmacology. Qualitative analysis comprised binary categorization into sex- and gender-based aspects and qualification with respect to the presence of a pathophysiological explanation for the sex or gender difference.
Results:
In relation to the total content of AMBOSS and KAPLAN, the sex- and gender-based share of the clinical subjects content was 26.8% (±8.2) in AMBOSS and 21.1% (±10.2) in KAPLAN. The number of sex- and gender-based aspects in the behavioral and social science learning material differed significantly for AMBOSS and KAPLAN (4.4% ± 3.1% vs 10.7% ± 7.5%; P = .044). Most of the sex- and gender-related content covered sex differences. Most learning cards and texts did not include a detailed pathophysiological explanation for sex- or gender-based aspects. The knowledge provided in the preparatory documents represents only a small part of facts that are already known about sex and gender differences.
Conclusions:
The preparatory materials focused almost exclusively on biological sex differences and the sociocultural dimension in particular is underrepresented. A lot more evidence-based facts are known and should be integrated into the materials to reflect the importance of SGBM as an integral component of patient-centered medicine.
Keywords
Introduction
Medical knowledge of biological sex differences as well as the awareness of socially constructed characteristics of the individual (gender) are recommended to use for diagnosis and therapy in daily clinical practice. Therefore, sex- and gender-based medicine (SGBM), as an integral component of patient-centered medicine, should be a mandatory part of medical education and national medical exams.1,2
Based on the definition of “sex and gender” used by the Canadian Institutes of Health Research (CIHR) and the Institute of Gender in Medicine in Germany, “gender” is a psychosocial construct comprising four main features: gender roles, gender identity, gender relations, and institutionalized gender. “Sex” refers to a set of biological attributes in humans and animals. It is primarily associated with physiological features including chromosomes, gene expression, hormone levels and function, and reproductive/sexual anatomy.3,4 Neither sex nor gender should be looked at solely due to their reciprocal influence of each other, and their joint impact on health. 5 The study by Pelletier et al. 6 laid the groundwork for the objective measurement of gender. This new ability to quantify the effect size of gender aspects in studies will lead to much more knowledge about the risk factors that contribute to the onset of disease.
Incorporation and translation of new facts based on sex and gender research into educational programs is challenging though.7,8 While medical curricula vary widely between universities, all medical students take nationwide standardized examinations, which therefore function as indicators for the governmental framework regarding the implementation of SGBM into medical education. Neither the German nor the American regulatory guidelines on medical licensing explicitly incorporate sex- or gender-based aspects in their learning outcomes apart from reproductive aspects and sexual disorders.9-11
To examine the extent of the implementation of SGBM and therefore the students’ sex- and gender-related medical knowledge, this study analyzes the learning material used to prepare for standardized national medical exams. All German medical students take the German state examination, a 3-day written, multiple-choice exam, at the end of their fifth year at university and before entering the 1-year clinical internship. The American counterpart with a comparable scope and value, the USMLE Step 1, is a 1-day written, multiple-choice exam, most medical students take at the end of their second year in medical school.
This study analyzes the e-learning materials of AMBOSS 2017 (https://amboss.miamed.de), a web-based knowledge platform used by 95% of German medical students to prepare for the German state examination, 12 and of USMLE Step 1 Lecture Notes (2017), an e-book series by KAPLAN MEDICAL, one of the leading companies in the test prep industry, and used by thousands of American students, 13 to test the hypothesis that the preparatory materials for the German and the American national medical exams incorporate sex- and gender-related content based on the already published scientific knowledge and that German and American medical students are therefore equally well prepared in the field of SGBM.
Methods
AMBOSS is a continuously updated, web-based knowledge platform, offering, inter alia, a comprehensive set of learning cards that cover the topics tested in the German state examination. The annually revised KAPLAN e-book series comprises seven volumes, each tailored for an examination subject of the USMLE Step 1. The subjects included in the analysis were allocated to one of the 3 main fields: clinical subjects, behavioral and social science, and pharmacology. To increase comparability, subjects specific to only one of the learning resources were not included in the analysis.
For a systematic analysis of sex- and gender-related content, a last year medical student who has been trained in sex and gender medicine for 3 years at the Institute for Gender in Medicine at Charité—Universitaetsmedizin Berlin performed a line-by-line analysis of the preparatory materials between April and October 2017 and was observed by a senior medical scientist expert for SGBM. Furthermore, a second expert in the field analyzed a randomly selected and representative sample size of the reviewed content with an inter-rater reliability (IRR) of 92.50%.
For the quantitative analysis of the respective preparatory material’s sex and gender awareness, each AMBOSS learning card and KAPLAN e-book chapter were assessed for the presence of sex- or gender-based aspects with respect to the eight categories: epidemiology, prevention, pathophysiology, clinical presentation, diagnostics, therapy, prognosis, and pregnancy. A section counted as sex- and gender-aware if there was at least one sex- or gender-based aspect included. After determining each subject’s share of sex- and gender-related content, the overall sex- and gender-awareness percentage for every main field was calculated. We used the weighted arithmetic mean of the respective subjects’ sex- and gender-awareness scores, considering their differing shares of the overall content.
The second step comprised the qualitative coding of the preparatory material by (1) binary categorization into sex-based aspects (biological differences of women and men) and gender-based aspects (socially constructed traits/characteristics attributed to an individual) and (2) qualification with respect to the presence or absence of a (patho-)physiological explanation for the stated sex or gender differences.
Statistical analysis
Descriptive and statistical data analyses were conducted using Microsoft Excel for Macintosh 16.12 and IBM SPSS Statistics 24 (Released 2016; IBM SPSS Statistics for Macintosh, Version 24.0; IBM Corp., Armonk, NY, USA), respectively. Inter-rater reliability was measured as the percent agreement between raters. Data were expressed in percentages for nominal variables. Significance of differences in sex- and gender-related content was calculated using Pearson chi-square test. A P value less than .05 was considered statistically significant.
Results
The distribution of the allocated subjects differed slightly between AMBOSS and KAPLAN. The learning material allocated to the category clinical subjects was 51.76% in AMBOSS and 35.71% in KAPLAN; 9.41% in AMBOSS and 14.29% in KAPLAN for behavioral and social science; and 5.8% in AMBOSS and 14.29% in KAPLAN for pharmacology. Subjects which presented with little content or were specific to either AMBOSS or KAPLAN were excluded from the analysis (Supplementary Table 1).
Quantitative analysis of the percentage of sex- and gender-related content of all analyzed subjects showed 84.2% within the immunology/rheumatology section of AMBOSS and 50% within the KAPLAN counterpart (P < .1). Sex- or gender-based aspects were mentioned in 35.7% of the AMBOSS learning cards covering the subject occupational and environmental medicine. Its counterpart, the KAPLAN chapter social sciences, did not contain a single sex- or gender-based aspect (P < .05). Analyzing the psychiatry content, 46.9% in AMBOSS, compared to 76.9% of KAPLAN behavioral science section, mentioned sex- or gender-based facts (P < .1). For the following subjects, the difference between the percentage of sex- and gender-related content of the AMBOSS and the KAPLAN learning material was less than 10%: endocrinology/endocrine pathology, hepatogastroenterology/hepatogastrointestinal pathology, nephrology/renal pathology, pneumology/respiratory pathology, and pharmacology. Epidemiology was identified as the only subject in both preparatory materials that contained at least one sex- or gender-based aspect in every e-learning card or e-chapter (sex- and gender-awareness of 100%).
In relation to the total content of AMBOSS and KAPLAN (Table 1), the sex- and gender-based share of the AMBOSS clinical subjects e-learning cards was 26.8% (±SD 8.2%) and the KAPLAN counterpart 21.1% (±SD 10.2%). The percentage of sex- and gender-related content within the behavioral and social science learning material differed significantly between AMBOSS and KAPLAN (4.4% ± 3.1% vs 10.7% ± 7.5%; P = .044). Within the main field pharmacology, 3.8% of the AMBOSS learning cards were sex- and gender-aware in comparison to 7.9% of the KAPLAN pharmacology chapters, however not significantly different.
Proportion of sex- and gender-related content of main fields in relation to total content of AMBOSS and KAPLAN.

Abbreviations: S&G, sex and gender; SD, standard deviation.
P < .05.
Figure 1A and B show the distribution of the sex- and gender-based aspects to the eight categories in the main fields clinical subjects and behavioral and social science. Approximately half of the sex- and gender-based aspects belonged to the category epidemiology. AMBOSS put further emphasis on the categories clinical presentation, diagnostics, and therapy. KAPLAN, however, focused on pathophysiology and clinical presentation. Learning material presenting facts concerning pregnancy was included in both. In the clinical subjects content, the following categories demonstrated significant differences between AMBOSS and KAPLAN: epidemiology (48.1% vs 39.7%; P = .024), pathophysiology (2.5% vs 28.5%; P < .001), diagnostics (9.8% vs 3.7%; P = .002), therapy (5.6% vs 0.7%; P = .001), and pregnancy (14.3% vs 9.4%; P = .045). The behavioral and social science content of AMBOSS and KAPLAN differed significantly in the following categories: pathophysiology (0% vs 14.6%; P = .002) and diagnostics (7.0% vs 0%; P = .009).

Distribution of sex- and gender-based aspects to eight categories in the main fields: (A) clinical subjects, (B) behavioral and social science, and (C) pharmacology. Comparison of AMBOSS and KAPLAN.
The pharmacological content of both AMBOSS and KAPLAN (Figure 1C) focused on sex- and gender-based aspects regarding therapy (43.6% vs 58.8%; P = .052), including differences in side effects between women and men and special instructions for the medical care of pregnant women, stating particular indications and contraindications.
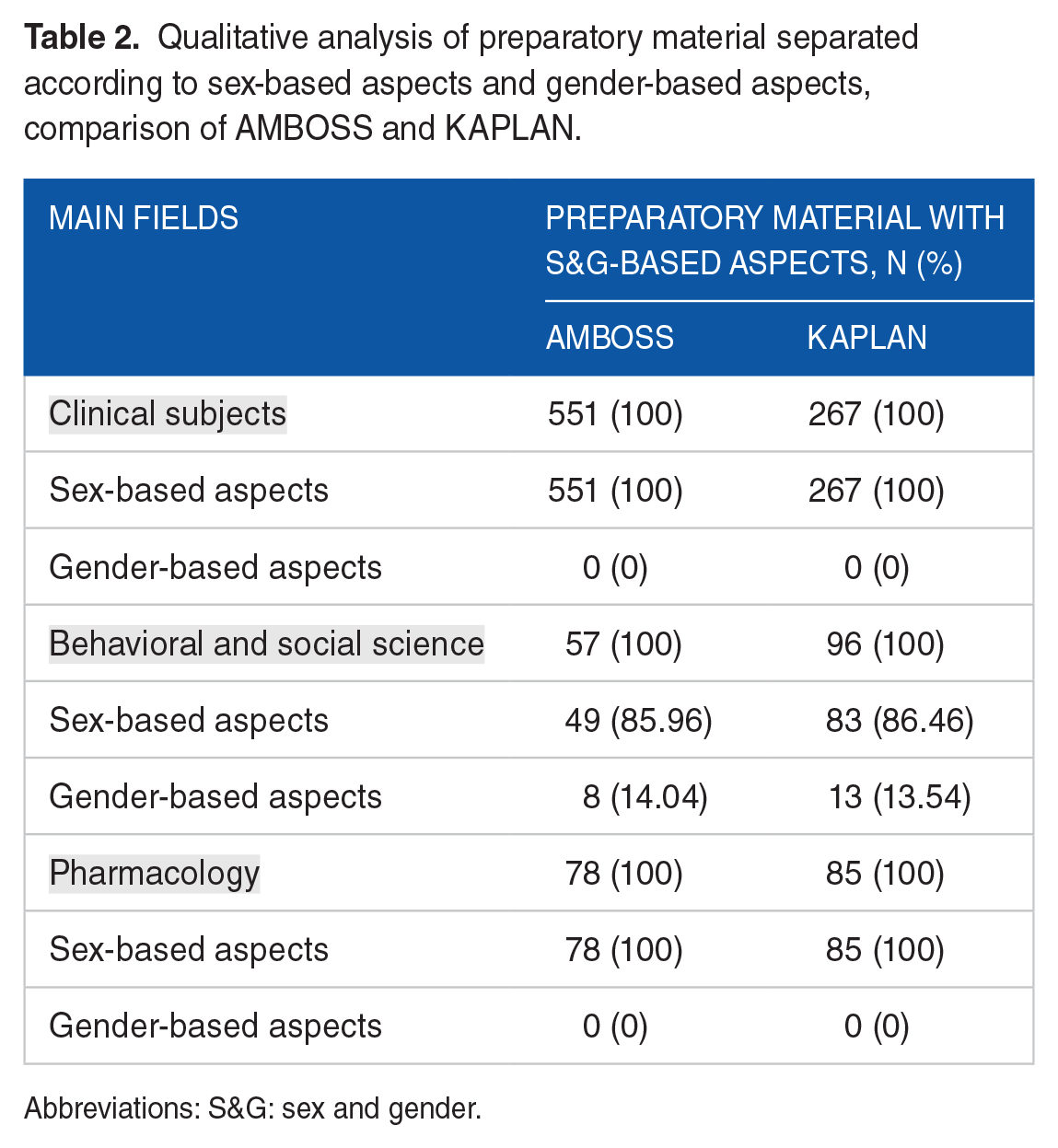
The overwhelming majority of the sex- and gender-related content in the preparatory material covered sex-based and therefore biological aspects (Table 2). Neither the clinical subjects nor the pharmacology content of either learning resource contained a single gender-based aspect. With 86.0% and 86.5%, sex-based aspects also predominated in the behavioral and social science content of AMBOSS and KAPLAN.
Qualitative analysis of preparatory material separated according to sex-based aspects and gender-based aspects, comparison of AMBOSS and KAPLAN.
Abbreviations: S&G: sex and gender.
Most learning cards and texts did not include a detailed pathophysiological explanation for sex or gender differences with a similar distribution pattern between the learning resources (Table 3). The pharmacology content contained the biggest share of explained sex- and gender-based aspects with 34.6% for AMBOSS and 23.5% for KAPLAN.
Qualitative analysis: list of two educational levels of the preparatory material with sex- and gender-related content: (1) with pathophysiological explanation and (2) with no pathophysiological explanation.

Abbreviations: S&G, sex and gender.
Discussion
The results indicate that the preparatory materials frequently used for preparing for the German and the American national medical exams contain sex- and gender-related content. Nevertheless, there is a lack of quantity and quality in regard to covering SGBM topics.
The main findings of the data analysis are as follows: (1) the overall lack of explicitly gender-related content in AMBOSS and KAPLAN, (2) the lack of a higher educational level regarding the comprised sex- and gender-based aspects in both preparatory materials, and (3) the significantly higher share of sex- and gender-related content incorporated in the main field behavioral and social science in KAPLAN compared to AMBOSS.
The vast majority of the included SGBM aspects in both learning materials comprised sex differences. This imbalance between biological facts (sex) and gender-based content (sociocultural aspects) could be explained by the challenge of measuring gender accurately. The study by Pelletier et al 6 laid the groundwork for the objective measurement of gender. They ranked patients having suffered from premature acute coronary syndrome on a masculinity/femininity-continuum according to their answers to a detailed questionnaire on sociocultural (gender) determinants (eg, income, education, social networks, environment, health literacy, cultural values), thus determining an individual’s gender score in addition to an individual’s biological sex. When implemented in clinical trials, this questionnaire will support and advance further research on sociocultural risk factors for diseases, and the obtained findings could lead to new gender-based preventive approaches.
Nevertheless, there are already sex- and gender-based facts that should be added as soon as possible to the exam questions pool. For example, atrial fibrillation increases embolic risk in women more than in men. Thus, at a societal level, women bear a greater burden of stroke than men.14-16 Heart failure (HF) is commonly associated with reduced ejection fraction (HFREF). However, this connection is predominantly found in men, whereas women more often suffer from HF with preserved ejection fraction (HFPEF).17-19 These symptoms occur based on diastolic dysfunction. Increased arterial pulse wave velocity (PWV ⩽ 9.7 m/s) and waist circumference >80 cm in postmenopausal women are associated with an increased risk of myocardial diastolic dysfunction. 20 Peripartum cardiomyopathy is a potentially life-threatening condition with multiple predisposing factors. 21 Therefore, it should be added to the exam topics as well. Diabetes is a stronger risk factor for vascular disease in women than in men. 22 Clinical presentation of systemic lupus erythematosus differs between women and men.23-25 Women present with earlier onset of disease and more frequent relapses of multiple sclerosis (MS). However, progression is faster, and outcome is worse in men with MS.26,27 A lot more evidence-based facts should be included in the exam questions pool. For additional information and literature on these facts, please refer to Table 4 highlighting knowledge gaps by way of example.
Examples of sex- and gender-related content identified in selected sections, facts not included in the learning materials, and knowledge gaps identified for future research.

Abbreviations: BMI, body mass index; F, female; M, male; ml, milliliter; S&G, sex & gender; SSc, systemic sclerosis.
Epidemiological sex- and gender-based aspects accounted for a large number of the total amount of detected data. The predominant absence of pathophysiological explanations for sex and gender differences supports the conclusion that sex- and gender-related content only serves as additional information. This could be caused by a lack of scientific evidence in regard to the pathophysiological mechanisms underlying the influence of sex and gender on health and disease or a lack of prioritization of sex- and gender-related knowledge in the preparatory materials and the respective standardized examinations.
Medical curricula emphasize so-called “hot topics” (areas considered of special importance by the accrediting body for medical schools in the United States and Canada), defined by the Liaison Committee on Medical Education. 38 In Germany, medical curricula should be based on the National Competency–based Learning Objective Catalog Medicine (NKLM). It is a competence-based core curriculum with a recommendation character (https://review.nklm.de/zend/).
Hochleitner et al 39 observed a discrepancy between the amount of evidence provided by sex- and gender-based research and its integration into conventional learning resources, which still consider the male body and physiology as the norm. Lack of support and guidance on an institutional (ie, medical faculties) and a governmental level (ie, compulsory guidelines) were considered influencing factors on the failure of a systematic SGBM implementation in medical education.
In accordance with the predominantly epidemiological data findings in this study, Song et al 40 found most of the sex- and gender-related content in their analysis on sex and gender of the Texas Tech University Health Sciences Center™ School of Medicine’s curriculum to be either of epidemiological nature or anatomy- and physiology-related. They discovered only incomplete coverage of many of the sex- and gender-based topics, which correlates with our finding that the analyzed preparatory materials rarely offered pathophysiological explanations for sex- and gender-based aspects. In a national student survey conducted by Jenkins et al, 41 clinical subjects such as endocrinology, rheumatology, cardiology, and pulmonology were considered to be covered moderately to extensively in regard to SGBM. However, more than half of the participants did not feel well prepared for transferring this sex- and gender-related knowledge into clinical practice.
As long as the implementation of sex- and gender-based medicine knowledge is not systematically integrated into the training and is not sufficiently taken into account in the exam questions, the students could only turn to alternative resources such as eGender, a web-based interactive knowledge sharing platform for sex- and gender-based medical education. 42
The comparison of the preparatory materials provided evidence to support the conclusion that KAPLAN had a significantly higher share of sex- and gender-related content in the main field behavioral and social science, probably due to the two countries’ differing approaches for addressing socioeconomic aspects within the medical curriculum. In the United States, behavioral and social science is considered an independent subject within medical education. In contrast, German medical curricula often integrate socioeconomical aspects of health and disease into a clinical subject’s syllabus, reflected in the lack of sex- and gender-related content in the main field behavioral and social science in AMBOSS.
Limitations
This study only investigated two distinct preparatory materials. While they are popular among medical students, there are also other commercial learning resources available. Nevertheless, AMBOSS and KAPLAN aim to offer a comprehensive preparation for the German state examination and the USMLE Step 1, respectively, and are both geared toward those standard examinations. Furthermore, we focused on a selection of subjects and did not include all subjects in our analysis to increase comparability between the two preparatory materials.
Conclusions
The sex- and gender-related content of the preparatory materials focuses almost exclusively on biological sex differences. Gender is an important influencing factor on health and disease that should be further integrated into the preparatory materials for national medical exams. The supplemental character of the gender-based content in learning resources fails to reflect the importance of SGBM as an integral component of patient-centered medicine.
Supplemental Material
Supplementary_Table_1_xyz27983efeaabf5 – Supplemental material for Quantitative and Qualitative Analysis on Sex and Gender in Preparatory Material for National Medical Examination in Germany and the United States
Supplemental material, Supplementary_Table_1_xyz27983efeaabf5 for Quantitative and Qualitative Analysis on Sex and Gender in Preparatory Material for National Medical Examination in Germany and the United States by Helena Schluchter, Ahmad T Nauman, Sabine Ludwig, Vera Regitz-Zagrosek and Ute Seeland in Journal of Medical Education and Curricular Development
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Society of Gender in Medicine (DGesGM®). We acknowledge support from the German Research Foundation (DFG) and the Open Access Publication Funds of Charité-Universitätsmedizin Berlin.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
US and HS conceived of the presented idea and developed the theory. HS and SL performed the analysis. ATN and US verified the analytical methods. VRZ supervised the findings of this work. All authors discussed the results and contributed to the final manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.