
Abstract
OBJECTIVES
The objective of this article is to describe the design and implementation of a multimodal, student-driven, sex- and gender-based women's health (SGBWH) elective with a curricular focus on patient and legislative advocacy. In this single arm, pre/post design, interventional study, we detail and evaluate the use of social media, newsletters, and round-table discussions in conjunction with a traditional lecture-based educational format to engage medical students in a virtual learning environment.
METHODS
We developed a 22-week SGBWH curriculum for pre-clinical and clinical medical students, which included a series of lectures on multi-specialty and gender-inclusive topics related to SGBWH, small group discussions with community leaders and legislators involved in women's health advocacy, and other self-directed resources such as social media, a website, and digital newsletters. Students were surveyed before and after completing the curriculum to assess for increases in self-reported confidence in advocating for their female and gender minority patients.
RESULTS AND CONCLUSION
One hundred and one students completed the anonymous pre- and post-elective surveys. There was statistically significant improvement in 8 of the 12 self-reported confidence measures. Eight (8%) participants identified their sex as male. Fifty-five (55%) participants stated future interest in primary care specialties (Internal Medicine, Family Medicine, Obstetrics and Gynecology, and Pediatrics). Our curriculum improved medical students’ self-reported confidence in advocating for their female and gender minority patients when controlling for sex and specialty interest of participants. The success of our multimodal approach demonstrates the value in incorporating resources such as social media as tools for education and advocacy in the evolving landscape of medical education.
Keywords
Introduction
Bias and discrimination on the basis of sex and gender manifest in medicine as gender disparities in healthcare outcomes,1–4 the underrepresentation of female participants in clinical trials, 5 and the inadequate coverage of gender-inclusive care in medical education. 6 Although strides have been made to increase female representation in clinical trials, 7 a recent analysis of female enrollment in US clinical trials suggests female participants remain underrepresented in research within the fields of oncology, cardiology, pediatrics, and infectious disease. 5 Furthermore, a 2008 survey of 125 allopathic US medical schools suggests medical students perceive their schools’ curriculum coverage of sex- and gender-based women's health (SGBWH) to be inadequate. 6 The consequences of these disparities are profound, resulting in differential health outcomes on the basis of sex and gender.8–10 The field of medicine does not exempt itself from a long history of the systematic marginalization of women.
In an effort to address gender and sex disparities in healthcare, medical education institutions have taken steps to amplify the teaching of SGBWH with ample room for improvement remaining. In 1995, the Office of Research on Women's Health at the NIH collaborated with the Association of American Medical Colleges (AAMC) in distributing a survey designed to assess the extent of women's health content taught at medical schools. 11 Results indicated of the 107 medical schools who responded to the survey, only 18 reported that they had implemented curriculum material specific to women's health. 12 Since this initial survey, subsequent surveys have shown that progress in developing SGBWH curricula has been slow. A 2006 study 12 analyzed curricula stored within a centralized medical school curriculum database, CurrMIT, and designated courses as “women's health courses” based on a variety of requirements: interdisciplinary approach, substantial content outside the reproductive tract, focus on women's health beyond reproductive-aged women, and focus on psychosocial factors. Using this more refined definition of women's health education, the study found that only 9 US medical schools offered designated women's health courses. More recently, a 2016 study employed a national student survey to assess sex and gender in medical education. 13 Their findings indicate current medical school curricula continue to be insufficient in covering sex- and gender-based health. A 2023 study reported a comprehensive assessment of sex and gender medicine topics in preclinical education at one medical school in Wisconsin, also concluding that medical students may not be receiving sufficient education to adequately treat all patients. 14
Many health education programs have made efforts to close the gaps in SGBWH education at the medical school level and to overcome the barriers that may hinder this process. Examples of these efforts include case-based discussions or modules 15 and incorporating women's health topics into concise real-world examples. These efforts aim to include content beyond the reproductive sciences and take an interdisciplinary approach to women's healthcare, representing a move away from the traditional approach to teaching women's health in medical schools.
Furthermore, student-led extracurricular electives and organizations exist at many medical schools for the purpose of supplementing medical education with focused lectures and events specific to student interests. In this paper, we share a framework by which other student organizers can design SGBWH curriculum content with a focus on patient and legislative advocacy to supplement medical education at their institutions. We will discuss the creation of a student-driven “Women's Health Elective” course offered to medical students at McGovern Medical School with the goal of expanding women's health educational topics beyond the scope of Obstetrics and Gynecology student interest groups. The primary focus of the elective was to equip students pursuing any specialty with the knowledge to adequately advocate for their female and gender-non binary patients. The elective was made available to all medical students, and our advertising content emphasized the importance of recruiting an audience that was neither gender- nor specialty-specific. As an equally emphasized goal, we aimed to equip students with legislative advocacy skills, given that there are opportunities to advocate for women and gender minorities in every field. We created advocacy opportunities that primarily focused on maternal mortality and morbidity reduction in Texas, with additional intersectional advocacy opportunities in partnership with other student organizations. In addition to a lecture series covering various aspects of women's health, we hosted roundtable discussions with legislators, community organizers, and scientific experts to educate students about the maternal mortality and morbidity crisis and opportunities for students to advocate for improved access and quality of women's healthcare in Texas.
Additionally, given the timing of the elective's implementation during the COVID-19 pandemic, we utilized a multimodal approach to education, incorporating social media, newsletters, and a website to maintain participant engagement throughout the lecture series. We employed anonymous pre- and post-elective surveys to assess knowledge gaps pertaining to women's health and evaluate the efficacy of an elective program that addresses the intersection of women's health, social justice, and a variety of medical specialties.
While the title of the elective in its inaugural year was “The Women's Health Elective,” we include the updated terminology of “sex- and gender-based medicine (SGBM)” and “sex- and gender-based women's health (SGBWH)” throughout this article for inclusivity. The term “women” was used in this elective to describe all individuals who identify as women. However, many individuals who are gender non-binary or are transmen require the same healthcare services that women do. To ensure inclusivity, we routinely referenced gender-minority considerations in the elective's curricular content and aimed for intersectionality in our language and framing.
Methods
This is a single arm, pre/post design, interventional study from August 2020 through April 2021 assessing the efficacy of a student-designed SGBWH elective curriculum for medical students. We created this elective with an innovative multimodal remote learning structure designed to enhance students’ self-reported confidence in women's health literacy and advocacy. Due to the fact that the elective's inaugural year was 2020 and in-person restrictions were in place for the COVID-19 pandemic, all events that took place were virtual. The curriculum was offered as an optional elective course within McGovern Medical School at the University of Texas Health Science Center at Houston to both pre-clerkship students and clerkship students. Students voluntarily enrolled in the elective and a power calculation was not performed to determine sample size.
Ethics approval and consent to participate
All participants were administered the anonymous pre- and post-elective surveys as per the requirements of the McGovern Center for Humanities and Ethics and Blue Book Elective requirements. A waiver of consent was approved by the UTHealth Houston Institutional Review Board. The IRB reference number is HSC-MS-20-0816.
Educational objectives
The objectives of this elective are to:
Educate an audience of medical students that is neither specialty- nor gender-specific on topics related to SGBWH. Highlight the gaps in medical research and pre-clerkship didactics in addressing SGBWH concerns, and provide students with supplemental knowledge to fill those gaps. Equip medical students to advocate for their patients who identify as women or gender-minorities, with special attention to addressing disparities in quality of care and access on the basis of sex and/or gender. Create opportunities for students to become advocates for SGBWH issues in the state of Texas through open discussion with state lawmakers and community leaders.
Implementation
After perceiving the need for additional advocacy training among medical students, the 4 medical student co-authors designed and implemented a voluntary “Women's Health Elective” available to all students at McGovern Medical School. The elective included a lecture series, round table discussions, social media, and newsletter in order to enhance engagement and reach.
Lecture series
In its inaugural year, the elective included 7 1 h lectures given by expert guest speakers that were held virtually via the WebEx platform. The lecture topics were selected by the student organizers and elective co-founders according to interest and availability of expert speakers. The elective content was intentionally designed to vary from year-to-year with a new annual cohort of officers determining which lecture topics would be best for the course for that year.
Each lecture was followed by a “Call to Action” related to the topic of the lecture. These calls to action included signing petitions, writing letters to elected officials, among other forms of advocacy. Lectures were also followed by supplemental readings to further enhance students’ understanding of lecture topics. These post-lecture materials were designed to provide students with tools to advocate for the specific issues addressed in the corresponding lecture.
Additionally, in order to enhance reach and affirm that there are opportunities to advocate for women and gender-minorities in any specialty of medicine, we collaborated and co-hosted events with other student organizations and interest groups to highlight the intersectional and multidisciplinary approach to SGBM. Table 1 includes the lecture topics addressed in the inaugural year of the elective and the other student organizations with whom we collaborated.
Lecture topics and co-sponsoring organizations.

Round table discussions
One major component of this elective included a 4-part round table discussion series to supplement the traditional lecture series. For each iteration of the elective, the round table discussions are meant to address one particular theme for the year. This theme, within the scope of SGBWH, varies from year-to-year depending on student body interests and current events. In the inaugural year of the elective, our round table discussions primarily addressed the maternal mortality and morbidity crisis in Texas. Central to the discussions were our invited guest participants, advocates for and experts in maternal healthcare. These guests included state representatives, committee members of the Texas Maternal Mortality and Morbidity Review Committee, physicians, other healthcare providers, lobbyists, researchers, and community organizers. We invited 3 to 4 guest participants to speak at each round table discussion.
In order to allow as many students to participate in the discussions as possible, we utilized the traditional question and answer format for the discussions, encouraging student participants to submit questions to the elective student organizers in advance. Up to 2 weeks prior to each discussion, a Google form was sent out to the students enrolled in the elective detailing the role of each guest participant and their roles in advocating for maternal health. Through the form, students were given the opportunity to submit questions addressed to a particular guest participant. These pre-written questions were sent to the guest participants several days prior to the discussion so they could prepare their responses.
The discussions took place over WebEx and lasted approximately 1 h. The discussions were moderated by the elective organizers. Each guest participant shared their role in combating the maternal mortality crisis, then they were asked to answer the pre-submitted questions from student participants. Each discussion specifically addressed the ways in which medical students could best advocate for maternal health. As the discussion progressed, student participants were encouraged to utilize the WebEx chat box to send additional questions.
Social Media
To supplement elective discussions and lectures, we utilized social media platforms as a tool to educate participants in real time. In particular, we created an Instagram account 16 and a Wix website 17 to reach a wider audience and continually engage our student participants in the elective content.
The utility of the Instagram account was 2-fold: we were able to present complex SGBWH topics in an easily digestible infographic format, and to reach a wider audience through the networks of students participating in our elective program. The content of our Instagram posts primarily included simplified legislative updates in addition to summaries of government reports, advocacy resources, and statistics related to SGBM. Additionally, we shared highlights of our elective events. For example, after every discussion or lecture, we transcribed impactful quotes from the guest speakers and shared them as timeline or story posts.
Using the Wix website platform, we uploaded and archived video recordings of all elective events with guest speaker permission. Students who were not able to attend events in real-time were then able to view the content asynchronously. Links to the videos could be shared to those outside the elective if a particular topic interested a student, and they felt compelled to share within their own network.
In addition to video recordings, we summarized legislative updates pertinent to the elective's scope and consolidated them on the elective's Wix website. During the Texas legislative session, each bill that was written related to women's health was categorized by topic. Categories include topics such as Postpartum Medicaid Expansion, Medicaid Coverage of Doula Services, Postpartum Mental Healthcare, Feminine Hygiene Products, Fertility, and others. Each bill was briefly summarized and linked to its full text. Updates were added in real-time as the bills advanced within committees and chambers throughout the session. This regularly updated website worked in tandem with the legislative updates in our newsletter and Instagram page to keep elective participants and their networks updated on health policy impacting women and gender-minorities in Texas.
Newsletter
Newsletters were sent to all of the elective's participants on a bi-weekly basis in order to keep participants up-to-date on SGBWH current events, legislative updates, and advocacy opportunities. Additionally, the newsletter served as an effective learning tool for the dissemination of factual information pertaining to women's health.
For example, each newsletter included a section titled “Everything You Need To Know About,” in which a relevant topic was broken down into key facts and made more digestible for readers. Examples of selected topics included introduced legislation, presidential memorandums, and published government reports. Furthermore, each newsletter included a section titled “Know Your Legislators.” In this section, factual and impartial information was shared about the state legislators who make policy decisions that directly impact healthcare for women and gender-minorities in Texas. This section included the legislator's roles in their specific chamber, provided a brief synopsis of the relevant bills they introduced, and summarized their voting history on issues impacting healthcare for women and gender-minorities. The purpose of this section was not to endorse or reject any specific legislator, but to provide students with the information to make informed decisions about legislators and the policies they promote.
An additional section titled “Legislative Updates” was included while the Texas legislature was in session. In this section, updates were provided about each bill related to women's healthcare. Along with bill updates, a brief synopsis of the bill and the bill's authors were outlined. The purpose of this section was not to endorse or reject any specific legislation, but to aid students in making informed decisions about policies and to aid them in their advocacy efforts.
Each newsletter also included a section of advocacy resources, which varied from specific opportunities for students to advocate for a variety of bills or causes to educational resources, such as videos, books, or articles. This section of the newsletter provided students with the opportunity to educate themselves beyond the newsletter (Appendix A).
Evaluation
Each participant was required to complete an anonymous pre-elective survey in order to enroll in the course. To earn credit for course completion, participants were required to attend 5 of the 7 lecture sessions and 1 of the 4 round table discussions along with the completion of a post-elective survey. Credit included documentation that the student completed the course on the Dean's letter sent with residency applications. Both surveys included the same 12 items for pre- and post-elective comparisons, which were written by the medical student co-founders of the elective. The questionnaire addressed self-reported women's health literacy and advocacy confidence measures. The questionnaire also assessed the participants’ beliefs regarding the current presence and importance of women's health in medical education using a sliding scale with options ranging from “0 = strongly disagree” to “100 = strongly agree.” The questions included in the anonymous pre- and post-elective surveys were written by the co-founders of the elective and are included in Table 2. The anonymous pre-elective survey did not include an option for participants to self-identify their sex assigned at birth, but this component was added to the post-elective survey to assess the demographics disparities in confidence measures on the basis of sex upon completing the elective.
Pre- and post-elective questionnaire items.

Statistical analyses
Data from the survey is presented as frequencies (with percentages) for categorical data and as medians and interquartile ranges (IQR) for continuous data. To assess the difference in pre- and post-survey responses as well as difference in subgroups results in the post surveys, a Mann–Whitney U-test was conducted using SPSS (version 26, SPSS Inc., Chicago, Ill., USA) with the results in Tables 1 to 3.
Pre- and post-elective survey results.

Rows in bold text indicate statistically significant findings (P-value < .05).
Scores are based on a 100-point scale (“0 = strongly disagree” to “100 = strongly agree”).
Results
Pre-elective survey and enrollment
A total of 144 students completed the anonymous pre-elective survey, thus enrolling in the course for the 2020-2021 academic year. According to the responses, pre-elective survey respondents strongly agreed with the statements that women's health is important in every medical specialty (median [IQR], 98 [86-100], Table 3), women's health extends beyond reproductive health (98 [89-100]), and physicians can advocate for their future female and gender minority patients in any specialty (98 [86-100]). Of note, pre-elective survey respondents self-reported relatively low confidence in the following advocacy-related skills: naming current legislation related to women's health (31 [17-50]), naming at least 2 avenues to effect change in local policy to better support female patients (33 [20-53]), and naming at least 2 avenues to effect change in local policy to better support gender-minority patients (30 [16-50]).
Student attendance
There were a total of 7 lecture sessions and 4 round table discussions offered by the elective. Each lecture/discussion was advertised directly to a total of 175 students who requested to be notified of events via email. However, each event was open to all 960 pre-clerkship and clerkship students at McGovern Medical School. The average attendance for lecture sessions was 68 participants, ranging from a minimum of 65 to a maximum of 102 attendees, and the average attendance for roundtable discussions was 45.5 participants, ranging from a minimum of 31 to a maximum of 60 attendees. One hundred seventy one students attended at least 1 event (lecture or discussion), and the average attendance of any event per student was 5 events, ranging from a minimum of 1 event per student to a maximum of 11 events per student.
Post-elective survey
A total of 101 students completed the post-elective survey. Questions in the anonymous pre- and post- surveys were designed to be grouped in 1 of 3 categories—evaluating the importance of women's health, the confidence students have in meeting the needs of their women and gender minority patients, and their confidence in policy and knowledge of avenues to effect change through advocacy. All of these realms yielded an increase in response ratings. Compared to the pre-elective survey responses, there were statistically significant increases in the mean ranks of self-reported confidence for questions 5, 6, 8, 9, 10, 11, and 12, as shown in Table 3.
Social media and newsletter engagement
Throughout the elective, 16 Mailchimp newsletters were sent to 184 recipients with an average of 83 participants opening each newsletter and a mean engagement rate of 45%. Between August 2020 and March 2021, 58 posts were added to the elective's Instagram account. Each post received an average of 29 interactions, which include likes, comments, shares, and saves. By March 2021, there were 351 followers of the Women's Health Elective Instagram account. The average number of impressions, defined as the number of times users saw the post, was 295 per post. The average number of accounts reached per post was 212, and the average number of non-follower accounts reached per post was 21.
Course completion
A total of 92 students completed the requirements of the elective during its inaugural year, starting in Fall 2020 and ending in Spring 2021. All were students in the School of Medicine's MD program. Of these, 28 were first-year medical students, 59 were second-year medical students, one was a third-year medical student, and there were no fourth-year students. Student retention between enrollees and those who completed all course requirements was about 65%.
Sub-group analysis
Of the 101 students who completed the post-elective survey, 93 participants identified their sex assigned at birth as female (92%), while 8 participants identified their sex as male (8%) as seen in Table 4. There were no statistically significant differences in the mean ranks of post-elective survey responses between male and female participants except question 10. The responses to this question indicate that upon completing the Women's Health Elective the self-rated ability to name at least 2 avenues to effect change in local policy to support their future gender minority patients was slightly higher in male compared to female participants (72 [62.5-86.25] vs 62 [39-76.5], respectively, P = .045).
Subgroup analysis of post-elective survey results: sex assigned at birth.
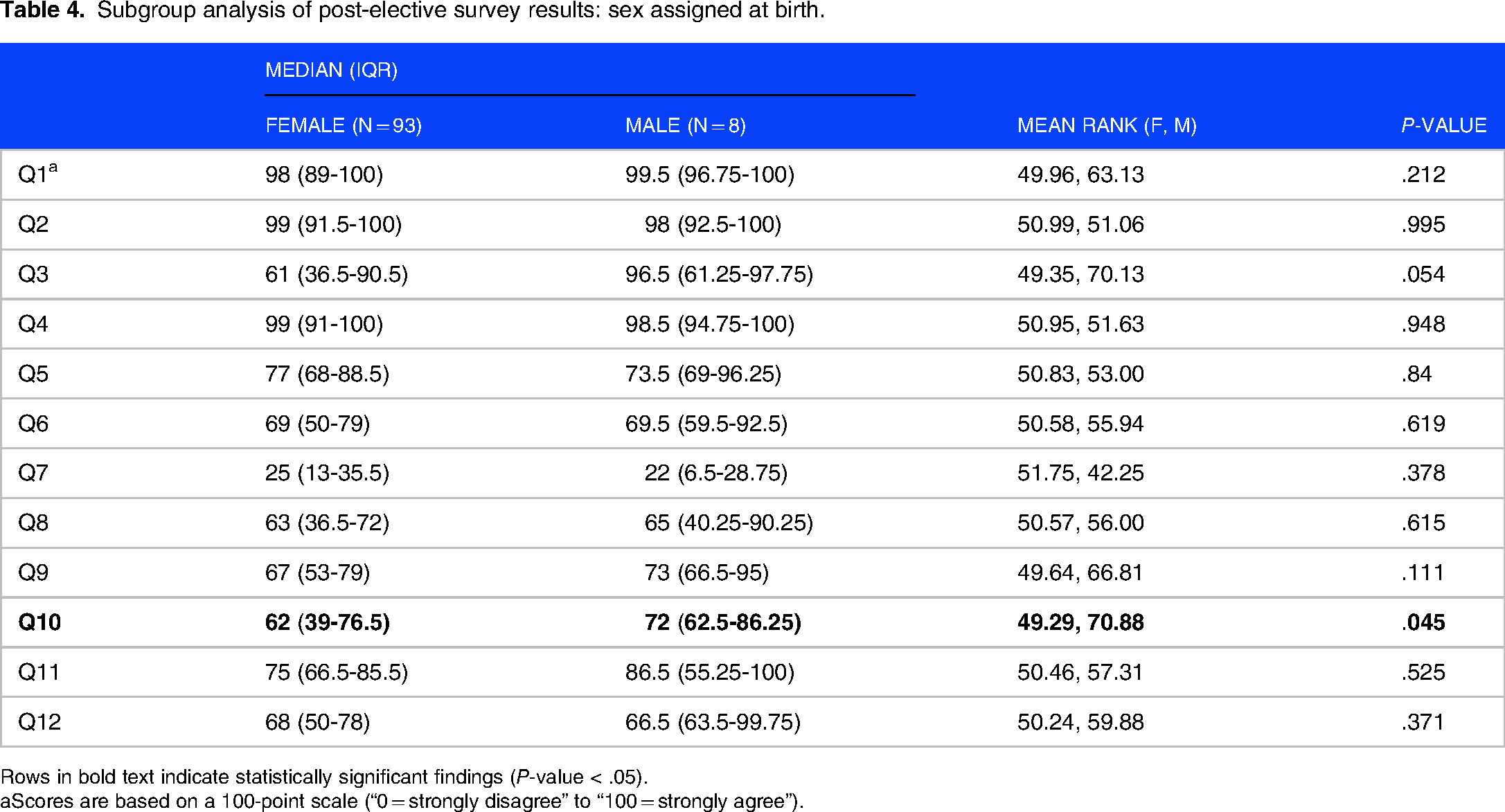
Rows in bold text indicate statistically significant findings (P-value < .05).
Scores are based on a 100-point scale (“0 = strongly disagree” to “100 = strongly agree”).
Students participating in this elective were interested in a wide variety of specialties (n = 17, Figure 1). Specialty interests were categorized into primary care and non-primary care specialties, as categorized by the AAMC. The primary care category includes Internal Medicine, Family Medicine, Obstetrics and Gynecology, and Pediatrics.

Participating students’ specialty interests.
Nearly half of the post-elective survey respondents indicated an interest in a primary care specialty (n = 55, Table 5), and there was no statistical significance in the mean ranks of their responses compared to those of students interested in non-primary care specialties.
Subgroup analysis of post-elective survey results: specialty interest.

Scores are based on a 100-point scale (“0 = strongly disagree” to “100 = strongly agree”).
Discussion
Our 22-week, student-run Women's Health elective improved participants’ self-reported confidence in advocating for their future female and gender minority patients when comparing pre-elective survey responses to post-elective responses. We observed that these findings were the same when controlling for variables such as sex of the participant and specialty interest. The questions that resulted in no significant change were broader statements about the importance of women's health. The responses to these questions in the anonymous pre-elective survey reflected that students entered the elective with a predetermined interest in providing quality care to female and gender minority patients, as evidenced by their high self-reported value of women's health.
The lack of statistically significant differences in the mean ranks of responses from students interested in pursuing primary care specialties versus non-primary care specialties was another notable finding. These responses corresponded to questions related to the value of women's health in every medical specialty and the role physicians play in advocating for female and gender minority patients. Prior to the start of the elective, we hypothesized that students primarily interested in Obstetrics and Gynecology would be the predominant participants; however this was not found in the survey results, as evidenced by the variety of specialty interests among elective participants. These results are in line with findings from a 2016 national survey study indicating the majority of medical students agree SGBM should be formally incorporated in medical school education. 13
Although the data analyses suggest statistical significance in post-elective survey responses between male and female participants, the study was not powered to detect statistical significance along this dimension with only 8 male participants. The low sample size also hinders any generalization of the results to male medical students at large. A 2008 study assessing medical students’ self-reported preparedness demonstrated women rated women's health curriculum content lower and felt less prepared than men in addressing topics related to women's health in the clinical setting. 6 It is possible that more female medical students sought to participate in our elective for similar reasons.
Strengths
The multimodal format of the elective offered a variety of avenues for participants to learn about SGBWH (ie, the newsletter, social media, recorded lectures, live lectures), which may have enhanced student engagement with the curriculum content. Other studies in the literature have demonstrated success in meeting educational objectives with multimodal approaches to the delivery of curricular content.18,19 In addition, students maintained the autonomy to decide when they wanted to engage with the elective's materials or lectures, an imperative component in engaging medical students with often demanding and rigid schedules. In order to receive credit for the elective, students had to meet a minimum number of lecture and discussion requirements but could decide which sessions best aligned with their schedules. Over the 22-week course of the elective, their requirements were a maximum of 2 h per month. Opportunities for additional asynchronous learning were made available through the website, Instagram page, and newsletter, the incorporation of which may have encouraged participant engagement. A 2023 cross-sectional study suggests medical trainees may prefer asynchronous learning to in-person didactics when managing work/life balance. 20 Moreover, the use of the WebEx platform for synchronous learning eliminated logistical barriers to attendance, including transportation time, parking, and reserving physical space for events. Both participants and guest speakers were able to attend lecture events and round table discussions without having to consider travel logistics.
Challenges
While the use of a video conferencing platform may have been a convenient alternative to in-person lectures, it did come with challenges. With the exception of 2 to 3 students per event, all student participants viewed the events with their cameras and microphones off. In live events student engagement can be gauged through non-verbal cues, such as eye contact and body language. However, via Webex, chat participation during the lectures/discussions was the sole indicator of participant engagement aside from self-reported survey feedback completed at the end of the course. A suggestion for monitoring engagement could include requiring that video cameras are turned on when logged into a Webex session in order to receive credit for attendance.
The recruitment of male participants in the elective was another challenge. We do not have data on the students who did not participate in the elective, so the reasons for this can only be assumed. “Women's health” is historically considered synonymous with the female reproductive tract and Obstetrics and Gynecology, an increasingly female-dominant specialty. 21 While we did emphasize that this elective was not specialty-specific, we also understand that many students not interested in reproductive healthcare may automatically assume “women's health” is not of interest to them. A suggestion for increasing gender diversity among participants in an SGBWH elective could include specifying the multi-specialty overlap in the elective's content when disseminating advertising materials. There is also room to further diversify the topics covered in the elective to include those within the scope of male-dominated specialties (eg, Interventional Radiology 22 and Surgery 23 ), given that 4 of the 7 lectures and all round table discussions were focused on reproductive healthcare.
Terminology presented another challenge in the presentation of gender-inclusive materials, as “women's health” and “maternal health” can exclude those who are gender non-binary or transmen. While the language of the elective's objectives incorporates patient advocacy goals for gender minorities, many of the research and policy resources developed by third parties and shared with participants do not.24,25 The survey responses from elective participants further highlights this challenge. There was a lack of consensus with respect to terminology, which was reflected in participant agreement to the statement that the term “women's health is inclusive to gender minorities.” The degree of agreement to the statement spanned across nearly the entire range of the measurement scale. In addition, there was minimal change in the distribution from the pre- to the post-elective survey suggesting that exposure to the elective material and concomitant increase in knowledge and/or confidence did not provide clarity on the issue of terminology.
Limitations
The voluntary nature of elective enrollment increased the likelihood of selection bias in the analysis of the elective's efficacy. The students who enrolled were likely motivated by a prior interest in SGBWH and some degree of understanding of the challenges and unique features related to the healthcare of gender minorities, as evidenced by the finding that the majority of participants “strongly agreed” that “women's health is important in every medical specialty” on the anonymous pre-survey. A more accurate measure of the efficacy of the elective would include students with limited knowledge of, or interest in, SGBWH.
Additionally, no power calculations were conducted prior to the study, and sample size was determined by the number of students who voluntarily enrolled in the elective. The survey questions used in the study were not previously validated, as they were written by the co-founders of the elective based on the curricular objectives.
Although the aim of the elective was to highlight SGBWH topics beyond the scope of Obstetrics and Gynecology, most of the advocacy-related content was focused on maternal health. The reason for this focus within Obstetrics and Gynecology was the emphasis of postpartum Medicaid expansion in Texas as a legislative priority during the legislative session that coincided with the elective's inaugural year. 26 Future iterations of this elective should broaden the advocacy scope to incorporate intersectionality within different areas of healthcare.
Conclusion
SGBWH remains an important and underrepresented topic in medical school curricula. Many efforts to enhance the representation of these topics have proven to be worthwhile. Our pilot Women's Health elective demonstrates the efficacy of a student-driven elective in improving students’ self-reported confidence advocating for their female and gender-minority patients in any specialty. Our multimodal approach to SGBWH education also demonstrates the value of incorporating social media, mailing newsletters, and websites as tools for education and advocacy in the ever-changing landscape of remote learning. We hope that the work presented here will help to further the progress of SGBWH representation in medical education.
Footnotes
Author's contributions
LC, DG, MN, and HS developed the elective, designed and administered the survey, and wrote the main manuscript text. RL provided guidance throughout the development of the elective and survey, as well as reviewed the manuscript. SN and SH analyzed and interpreted the survey data. All authors read and approved the final manuscript.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
All participants were administered the anonymous pre- and post-elective surveys as per the requirements of the McGovern Center for Humanities and Ethics and Blue Book Elective requirements. A waiver of consent was approved by the UTHealth Institutional Review Board. The IRB reference number is HSC-MS-20-0816.