
Abstract
OBJECTIVES
Sex and gender have profound effects on disease prevalence, presentation, and outcome, but these issues are not covered in depth in standard medical school curricula. To improve understanding of women's health, an intensive 1-month class was offered to fourth-year medical students.
METHODS
The class combined background lectures on the biological and social determinants of women's health with presentations on specific medical conditions by practicing clinicians and students. Students’ anonymous responses to end-of-class evaluation used by Stony Brook University School of Medicine as well as pre- and post-class answers to the question “why are women twice as likely to go to the doctor” were analyzed using quantitative, descriptive, and qualitative approaches.
RESULTS
The class was given between 2017 and 2022 to a total of 154 students. Course evaluations were submitted by 133 students. Over 80% of responders ranked the class as good or excellent and many expressed surprise about how much sex and gender influence health. Furthermore, before taking the class responders favored gender stereotypes (82%) and OB/GYN visits (56%) as the main reasons why women utilize healthcare more often than men, whereas only 31% of post-class answers included these factors (p < .0001), which were replaced by others including misdiagnosis, high rate of adverse effects of medications, implicit bias, and longevity.
CONCLUSION
A dedicated class given to students at the end of their undergraduate medical training increased awareness and knowledge of the effects of sex and gender on women's health.
Introduction
The need to incorporate sex- and gender-based education into the medical curriculum has been recognized since the early 1990s after surveys requested by Congress found that only a very small proportion of schools include information on leading causes of death in women and on medical disorders that disproportionally affect women. 1 This situation has not changed substantially since then: a study using a centralized medical school curriculum database (CurrMIT) to assess the inclusion of women's health and gender-specific information in the curricula of US medical schools found that between 2003 and 2004 only a handful of medical schools offered an interdisciplinary women's health didactic or clinical learning experience. 2 In a 2011 survey that included the majority of medical schools in the US and Canada, 70% of responders reported not having formal gender-specific integrated medical curricula and that coverage of health topics including evidence of sex- and gender-based differences was minimal. 3 More recently, results of a national student survey suggest that while most medical students recognize the translational value of sex- and gender-based medicine (SGBM) in healthcare, students also reported that the current curricula fall short of providing adequate coverage of specific evidence-based health differences between men and women. 4 Failure to recognize SGBM as an integral part of medical education is also reflected in the scarcity of SGBM topics covered in learning materials commonly used by German and American medical students to prepare for standardized national medical exams. 5
Currently, there is no consensus on how to best incorporate information generated from the growing field of SGBM into educational and training programs.6,7 Recent efforts to advance sex- and gender-based health education have focused on the creation of teaching materials and tools geared toward integrating these concepts into undergraduate and post-graduate medical curricula.8–17 However, how to incorporate new data from the fast-growing field of SGBM remains a challenge. Here, we report on the design and implementation of a 1-month intensive course named “Issues in women's health and gender-based medicine,” offered to fourth-year medical students at the Renaissance School of Medicine at Stony Brook University. The class comprises lectures given by experts in different medical and related specialties and a “flipped classroom” approach in which students choose research, and present a topic related to women's health and SGBM, allowing for a flexible and multidisciplinary learning experience. We present qualitative and quantitative data showing our course significantly increased students’ appreciation and knowledge of how sex and gender impact women's health, clinical treatments, and outcomes.
Materials and Methods
To evaluate students’ experience with the class, we performed a cross-sectional, retrospective analysis of course evaluations provided anonymously by students at the end of the class per school requirements which are made available to instructors. To evaluate students’ knowledge gain, we analyzed students’ anonymous responses to a knowledge assessment question.
Course Design and Content
Fourth-year medical students at SBUMED are required to take 1 of 6–8 “selective” (required elective) classes on topics that are not covered in the standard curriculum. A full syllabus for a 4-week course on SGBM was discussed and approved by the School of Medicine Curriculum Committee in 2016. Students provided 3 top choices among all the selective classes offered and were assigned to 1 of these 3. All students who were assigned to and participated in the course were eligible to participate in the class evaluation. Students who did not participate were not eligible. Class size was capped at 24 students/iteration to ensure there was enough time for meaningful participation by all students.
The class met 3 times a week (2 h/session) over 4 weeks. The first week of the class was dedicated to introductory lectures. Students were directed to the websites of national and international databases (eg, the gender lens16,17,18–20) focusing on SGBM and instructed to choose a topic for their own research and presentation. In all content areas, we emphasized that “absence of evidence is not evidence of absence” and encouraged students to choose and explore topics not covered by lectures in class.
The first introductory lecture (“why SGBM”) described historical landmarks in the evolution of attitudes toward women's health within the broader perspective of the social attitudes toward women; from the description of hysteria by Hippocrates, 21 through the historical exclusion of women from medical schools and the practice of medicine, 22 the 1977 Food and Drug Administration (FDA)-mandated exclusion of women from clinical trials, the reversal of this ruling in 1993 23 and the more recent (2015) National Institutes of Health mandate to consider sex as a biological variable in biomedical research. 24 This introductory lecture chronicled how bias and paternalism perpetuated ignorance of the true nature of female physiology and medical needs. The class then transitioned into discussing how these views and attitudes toward women's bodies and health are being replaced by the recognition that sex and gender affect disease prevalence, presentation, and outcome as well as the response to pharmaceuticals and other medical interventions.25,26
Subsequent introductory lectures covered the genetic and biological mechanisms underlying sexual differentiation and examples of the effects of sex and hormonal environment on disease prevalence, presentation, and outcomes; including response to medical and surgical interventions. We introduced each content area with a general statement, that is, “sex and hormones affect disease prevalence,” followed by a partial list of diseases characterized by a large (>2-fold) difference in prevalence between men and women: starting with the letter A, attention deficit disorder and autism are more prevalent in men, while Alzheimer's disease (AD) and the absolute majority of autoimmune diseases are more common in women. We then followed up with a detailed analysis of factors contributing to sex differences in the epidemiology of AD.27,28 Similarly, we followed the observation of a generally higher rate of adverse drug effects in women with a review of sex differences in the response to common drugs for cardiovascular diseases (CVD), including statins, antiplatelet and antithrombotic agents, β-blockers, digoxin, vasodilator therapies, and drugs associated with the Long QT Syndrome.29,30 From this list, we chose aspirin and digoxin as specific “case studies.”31–34 This content area ended with a description of the many sex differences in—and gonadal hormone effects on—drug pharmacokinetics and pharmacodynamics, resulting in sex differences in safety and efficacy of drugs commonly prescribed to men and women.35–38 In this regard, we described the first example of incorporating data on increased risk to women into clinical guidelines, namely the FDA recommendation of an Ambien dose for women, which is half the recommended dose for men. 39
The rest of the course consisted of 2 h meetings with 1 h guest presentations that focused on best practices and ongoing research in diverse medical fields and disorders. Specific diseases (eg, multiple sclerosis and epilepsy) were addressed by clinical experts in interactive lectures including case presentations. During the second hour, students (1–3/group) presented a structured 20-40 min PowerPoint presentation that reflected a comprehensive literature review on the sex or gender differences in a disease or health-related area. Students introduced the topic, provided examples of clinical and/or pre-clinical research articles, and summarized relevant information. Students also discussed the gaps and limitations of the available research and provided possible future directions. Throughout their presentations and afterward, students answered questions from their peers and the course directors, providing space for discussion. The full syllabus which includes introductory lectures, lectures presented by guest speakers, and examples of the topics presented by the students is summarized in Table 1. A binary grading system of pass or fail based on students’ attendance and the completion of the class presentation assignment was used.
Syllabus: issues in women's health and gender-based medicine.a

Abbreviations: ADHD, attention deficit hyperactive disorder; CVD, cardiovascular disease; CNS, central nervous system; MI, myocardial infarction; MS: multiple sclerosis; PTSD, post-traumatic stress disorder; SLE, systemic lupus erythematosus.
Start date: April 4, 2017, 12 sessions (3/week), 2 h each.
Course Evaluation and Assessment
A retrospective analysis of course evaluations from 2017 to 2022, which encompasses 9 iterations of the class, was performed. Briefly, in agreement with Stony Brook University's end-of-course evaluation practices, all students are asked to complete a course evaluation anonymously and electronically (CBase). Responses are recorded on a 5-point Likert scale (strongly agree or excellent, agree or good, indifferent or average, disagree or poor, and strongly disagree or very poor). Narrative feedback from students was optional, including items such as “The best feature of the course” and “The aspect of the course most in need of improvement” (Supplemental file 1).
To determine whether the course enhanced students’ knowledge and appreciation of the importance of sex and gender in the clinic, we asked students to answer the question: why are women twice as likely to go to the doctor? before the start of the course and at the end of the course. Then, answers were compiled and deidentified for analysis. The use of this tool was initially piloted in the first 2 iterations of the class whereby the question was presented in the last hour of the class and students’ verbal responses were recorded on the blackboard. Subsequently, students were asked to compose their answers on their electronic devices (laptops or smartphones) and email them to the course directors before the first lecture and again at the end of the course.
Data Analysis
Evaluation scores were analyzed using descriptive statistics, expressed in percentages. Where appropriate, the mean and standard deviation of the mean were presented as well.
Qualitative data obtained from the narrative feedback provided by the students were combined and analyzed by thematic analysis.
40
Content analysis
41
was utilized to perform a systematic and quantitative description of students’ pre- and post-class answers to the knowledge assessment question. Inductive coding was used on all qualitative data to generate themes as well as to categorize the students’ pre- and post-class answers. In brief, 2 researchers (MAM and AB) read the students’ answers or comments separately and color-coded sentences they judged as belonging to different themes/categories (Supplemental Files 1 and 2). The researchers compared and discussed their codes until a consensus was reached. Themes or categories were identified by reading these codes (see Supplemental File 3 for additional details related to the qualitative analysis
Statistics
For figures and statistics, Graph Pad Prism 9 was used. The significance of differences between pre- and post-class responses to the knowledge assessment question was calculated using Fisher's exact test; with p < .05 considered statistically significant.
Ethical Approval
This study is exempt from Institutional Review Board approval under published US federal guidelines §46.104 Exempt research. Subpart d
Results
Overall Course Evaluation
A total of 154 students took the class between 2017 and 2022 (63% women). Of these, 133 (86%) answered the course evaluation questions provided by the School of Medicine. Course satisfaction was rated as good or excellent by 80% of responders, with mean Likert ratings of 4.1 out of 5 (4.1 ± 0.1), 17% ranked the class as average or with a neutral rating, and 3% rated the class as poor. The majority of students (84%) agreed that the course offered clear learning objectives that were met upon completion of the class. Importantly, more than 80% of students gave a good or excellent ranking (4.3 ± 0.1) to the course structure and its integration of basic science and clinical correlates.
Qualitative Analysis of Narrative Feedback
Sixty-eight students (51%) provided comments about “the best feature of this course” and qualitative thematic analysis identified 3 major themes. Representative students’ responses (verbatim) related to the various themes are captured in Table 2 and theme identification is illustrated in Supplemental File 1.
Examples of major themes in students’ comments.

The first theme identified pertains to the format and content of the course with students indicating that a combination of guest lectures and the opportunity to present to their peers about a topic they were interested in was the feature of the class they liked the most. Students’ comments also expressed satisfaction with the topics covered and the engagement in the discussion they provided.
The second major theme identified was that the class increased students’ knowledge and awareness of the importance of sex and gender in the clinic and research and that this knowledge will significantly influence their future clinical practice. Students stated that prior to taking this class, they were not aware of the material and expressed surprise at the extent to which both sex and gender can influence and often determine clinical outcomes. In this regard, students also stated that the course should be mandatory or be part of the undergraduate medical curriculum.
The final major theme was students’ appreciation of the inclusion of lectures and discussions incorporating lesbian, gay, bisexual, transgender, and queer or questioning (LGBTQ) individuals’ health and related societal issues.
It is important to point out that students’ choice of topics was autonomous and often related to the student's residency choices. In addition, student presentations included topics inspired by medical health issues of current public interest. For example, as a result of the current US opioid epidemic, pain management is a topic that is now at the forefront of medicine. 43 While our class did not have a guest lecturer with expertise in pain, thanks to student presentations on this topic, important gender differences in presentation, pain sensitivity, and treatment of different types of pain and treatment responses were presented and discussed. Other students’ presentations reflected the class's interest in areas not covered during their undergraduate education. For example, medical treatments related to gender transition and transgender health were among the topics chosen by students on more than 1 occasion (Table 1).
Analysis of students’ comments on “the aspect of the course most in need of improvement” revealed 2 prevalent themes. The first was an interest from students in having more clinically focused presentations including discussion of cases and the second was more time for discussion. These suggestions prompted the course directors to shorten the background lectures during the first week of the class to allow for a 30–40 min free discussion period addressing controversial subjects. The free discussion topics included clinical trials in pregnant women, sex assignment surgery (ie, surgeries performed on newborns with ambiguous genitalia), and treatment of gender dysphoria, among others. Judging by the comments on subsequent class iterations (from 2018 onward), students expressed appreciation for the opportunity to discuss contentious issues. However, even after these changes, some students expressed their desire for more discussion time on topics presented by guest lecturers.
Quantitative and Qualitative Knowledge Assessment
We hypothesized that taking this class would increase students’ knowledge about the underlying sex- and gender-specific causes responsible for ill health being more common in women, including higher prevalence of chronic (eg, autoimmune) incurable diseases, longevity, higher prevalence of adverse effects of medications and caregiver bias, which is reflected (among other things) by a higher number of office and outpatient clinic visits by women relative to men.44–48 Hence, answers to the pre- and post-class question, why are women twice as likely to go to the doctor? were analyzed. A total of 65 students gave answers both before and after the completion of the class. Two students answered the question only once, before the first lecture, whereas 3 students answered the question once after taking the class.
Analysis of pre- and post-class students’ answers resulted in the identification of 9 major categories: societal expectations or gender stereotypes (eg, men are expected to be strong and ignore discomfort or pain, women are more “in touch with their bodies” and more prone to ask for help), visits to OB/GYN (women have reproductive health problems that men do not have), safety and efficacy of interventions (ie, side effects or lack of effectiveness), missed/late diagnosis (explained as due to the atypical presentation of some disorders in women), effects of hormonal changes, physician implicit bias (leading to under diagnosis, under treatment and ignoring complaints about adverse effects), lack of research studies that include and analyze the effects of gender, higher prevalence of chronic diseases among women, and longevity (see Supplemental file 2 for examples). Before taking the class, 82% (56 of 68) of responders wrote that differences in societal expectations or gender stereotypes explain why women utilize healthcare more often than men, whereas post-class answers showed that only 31% (21 out of 68) of participants identified these as an explanation (p < .0001).
Furthermore, after completion of the class, students’ answers were more multifaceted and nuanced relative to their pre-class answers (Figure 1). For example, 85% of pre-class responses included only 1 or 2 items, mostly concerning gender stereotypes and/or OB/GYN visits. In contrast, most post-class responses (79%) included 3 or more categories. Importantly, after taking the class, a substantial percentage of responders (30%) included the historical exclusion of women from clinical trials as a factor contributing to poor clinical outcomes, acknowledging the need for more research that includes gender. Furthermore, while higher prevalence of chronic diseases and differences in disease presentation comprised only 9% and 10% of the pre-class answers, their percentages among post-class responses increased to 64% and 37%, respectively. Similarly, physician implicit bias and longevity comprised 6% and 2% of pre-class answers but accounted for 24% and 16% of the students’ responses after class completion. Other reasons given in post-class answers included: lack of education among healthcare providers, women's primary role as caregivers, and physical and verbal intimate partner violence.
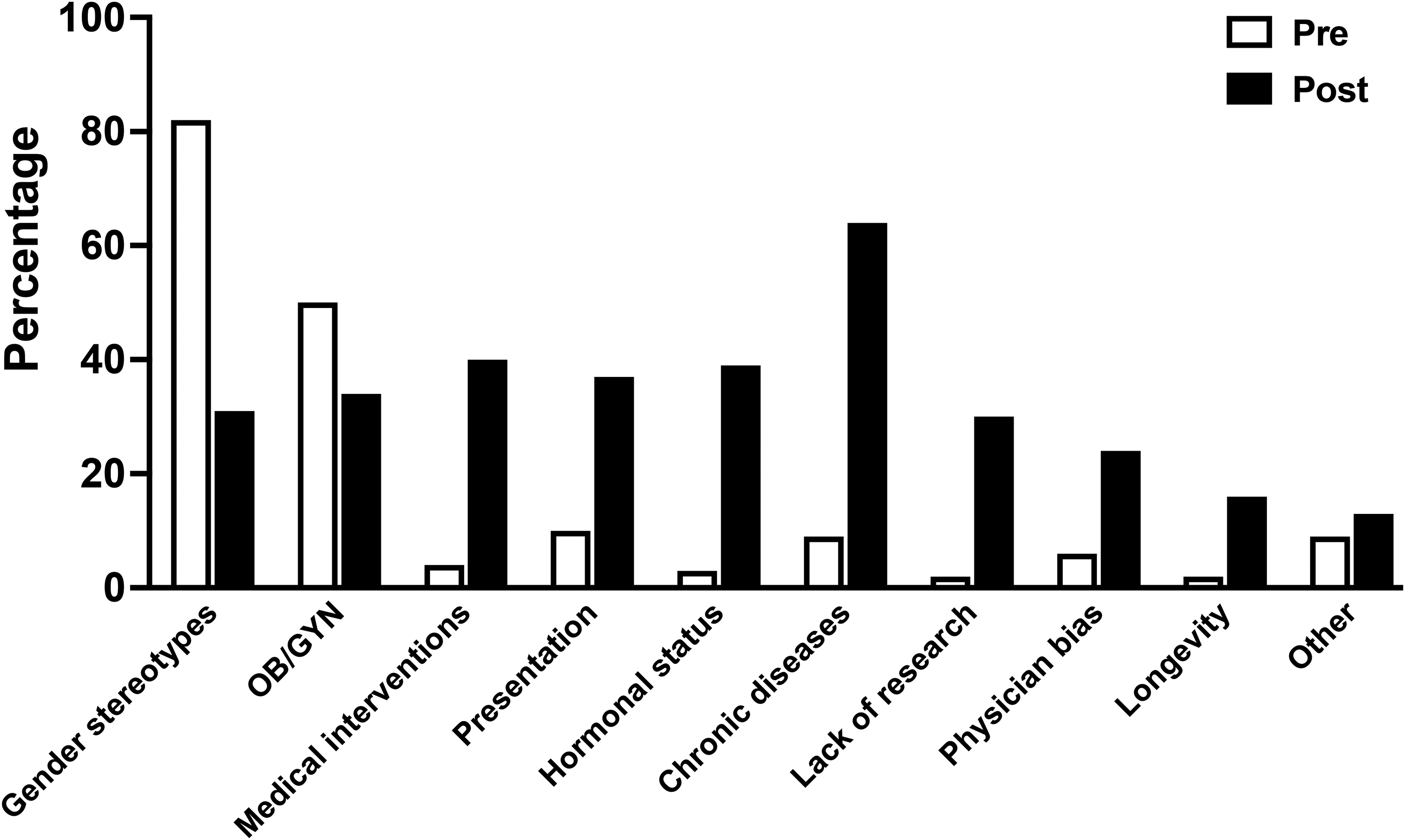
Percentage of students who included category in pre- and post-class answers to the question “why are women twice as likely to go to the doctor?
Discussion
Education about the importance of sex and gender throughout medical training is an indispensable tool to close the gaps that exist in clinical care for women. We report on the implementation of an intensive, 1-month course designed to expand the understanding of women's health beyond reproduction. 49 The flexible nature of the course is conducive to constant adaptation to new information, a challenge unlikely to disappear for this fast-growing field. For example, our speakers are chosen such that they are active in SGBM in their field,28,50–53 hence, students benefit from up-to-date information including unpublished data. In addition, the subjects of one-third of the sessions are chosen by students, ensuring the inclusion of topics not covered by faculty which tend to be new and recent. Notably, the course appears to have achieved its goals repeatedly over the years despite changes in topics and speakers, supporting the idea that this course could be easily adopted by other schools. This is supported by qualitative and quantitative analysis of data obtained from students’ anonymous survey responses and from a knowledge assessment tool showing that learners leave the course with an appreciation of the large knowledge gap pertaining to women's health. Importantly, the vast majority indicated that the class will influence the way they practice medicine in the future.
A few national and international efforts to implement SGBM in undergraduate medical training have focused on the systematic integration of sex and gender knowledge throughout the medical curriculum, a task requiring a significant amount of time as well as the commitment of institutional resources.11,14,15,54,55 For example, after identifying the content gaps within the basic science medical curriculum, a year-long process, Texas Tech University Health Science Center integrated SGBM into their existing medical curriculum via the creation of several educational tools including a slide library of peer-reviewed lectures, interactive online modules, and clinical cases.56,57 In other instances, centers for “women's health” such as the Mary Horrigan Connors Center for Women's Health at the Brigham's and Women's Hospital have served as bridges that bring sex- and gender-informed medicine into the undergraduate medical curricula. 58 Other strategies employed by institutions include lecture series centered on SGBM themes offered throughout the academic year and open to medical students as well as to trainees from other health professions such as nursing and pharmacy. 59 However, due to the diverse and nascent nature of SGBM education, a clear picture of the effectiveness of these educational strategies is still evolving. 6
Our educational intervention strategy has been to offer a dedicated class on issues in women's health and gender-based medicine, combining lectures given by experts in different fields and students’ presentations about a topic of their choosing. Even though the implementation of dedicated courses about SGBM in medical schools has been reported,60,61 an important distinction between ours and similar reported efforts is the targeted learner audience. Our class is intended for fourth-year students when they have completed their pre-clinical coursework and most clinical rotations and are on the brink of residency. While some studies suggest that integration of SGBM concepts into the curriculum should start from the beginning of medical school, 62 an advantage to offering a dedicated course at the end of their medical school training, as opposed to the first year, is that it allows students to better appreciate the complexity of themes and makes them reflect on the applicability of what they have learned to their future interests in the clinic.
Our approach resonates with a recent study, in which the sex- and gender-based content of the medical curriculum at Yale School of Medicine was evaluated by medical student audits. 63 Responders noted that only a few sessions included an in-depth discussion of sex and gender differences, and when included, these were limited to basic physiology and prevalence and/or incidence of disease, with the influence on diagnosis, treatment, prognosis, and drug effects barely discussed. The authors further recommended content on the historical implications of gender bias in research and how to design research studies that adequately analyze sex and gender differences. Improved coverage of sex and gender differences beyond presentation of disease that includes diagnosis, pharmacology, and prognosis of disease was also advocated. Our class has elements of these didactic recommendations. For instance, the introductory session of our course addresses the historical bias and the detrimental consequences of excluding women from the practice of medicine and clinical trials; moreover, the presentations by our guest lecturers and students inform the class of up-to-date research that includes both men and women with results stratified by sex as well as research targeting gender minorities.
Our class was conceived with the premise that a knowledge gap on sex and gender differences in health and disease exists in our medical school curriculum. Students’ pre-class answers to the question why women are twice as likely to visit a doctor? confirmed this knowledge gap and uncovered the existence of possible gender bias among students. In medicine, gender biases are caused by gender blindness and by stereotyped preconceptions about men and women. 64 Gender stereotypes are acquired in society and are based on perceived gender roles, identities, and portrayals64,65; which may have a negative impact on diagnosis and management because they lead to differences in treatment between women and men patients that are not clinically justified. Gender blindness, on the other hand, is the inability to recognize differences that are clinically pertinent, such as by assuming that the research findings obtained using only male subjects can be applied to women.64,65 Before completing our class, most students saw societal expectations and OB/GYN visits as primarily responsible for women's more frequent visits to the doctor. Societal expectations referred to a “macho attitude” explaining men's reluctance to go to the doctor, unless conditions or symptoms are hard to ignore, while women are more likely to admit weakness and are more “attuned to their bodies” and hence more prone to visit their doctor. While it is true that gender differences influence men's and women's behaviors within the healthcare system, 66 they should not be the only cause considered by future clinicians to explain health inequities. Similarly, while pregnancy, childbirth, fertility treatments, and birth control do require women to see doctors and undergo procedures that men generally do not require, this difference alone cannot account for the difference in healthcare utilization, which is seen across medical specialties.44–48 In contrast, post-class answers showed that students’ attitudes toward the subject changed after taking the class; notably, post-class answers indicated a broadening of students’ definition and understanding of women's health beyond reproduction, with student's answers now including noncommunicable diseases and the acknowledgment that women are preferentially affected by chronic illness beyond their reproductive years.
Our study has several limitations. It is based on the results from a single US institution and therefore may not be generalizable to other institutions and parts of the world. As we did not have a prior validated tool to measure the impact of the education, we created a tool de novo, which may need further validation. We did however pretest the tool to ensure that it was relevant to the stakeholders. Given the relative paucity of reports of such curricula in undergraduate medical education, we used an open-ended qualitative approach to understand the evolution in learner attitudes and knowledge. We were rigorous in our qualitative analysis to ensure that there was internal consistency and trustworthiness of data.
Similar to what has been reported by others, 6 challenges pertaining to broader impact and long-term sustainability exist. Initial attempts to integrate SGBM into all years of the required curriculum in our school were met with resistance from senior faculty; the majority of whom thought this approach was too radical. The limited time eventually allotted to the course made it challenging to encompass the full impact of sex and gender on health and the practice of healthcare. In an attempt to meet this challenge, didactically, we used a limited number of specific “case studies” as examples of an underlying concept or theme. Additionally, identifying and recruiting practicing clinicians who are both willing and able to contribute is an ongoing challenge that is likely to be encountered at most institutions. Finally, institutional funds for outside experts to expand the range of topics are important but difficult to obtain. We were able to invite an outside speaker with expertise on lesbian health in the Fall 2017 and Spring 2019 semesters using a one-time presidential grant for diversity, but this is not a viable long-term solution to resource constraints.
Conclusion
In conclusion, we show that exposing senior medical students to an intensive course on SGBM increased awareness and knowledge about women's health. Importantly, learners were able to examine their assumptions about gender and stereotyped generalizations, which might help reduce gender biases in their future practice. Additionally, learners leave the course with a more diverse understanding of what constitutes women's health. Our next steps include creating a more robust set of data related to learner performance in simulated environments with SGBM as a key theme in standardized patient encounters to see if changes in attitudes and knowledge translate to observable behaviors. The ultimate goal of medical education is to affect practitioner behaviors toward their patients and observation in simulated environments is a practical way to assess change in behaviors. We also believe elements of our class could be utilized by other medical institutions and might offer a platform for future integration of SGBM in the undergraduate medical curriculum. To this end, we plan to make class materials more widely available by featuring presentations on virtual platforms, such as a recent conference we organized on “The long road to equity for women in medicine” (https://youtube.com/playlist?list=PLlDSLa2SrI-ZkioweZq6Rvsp3D6t5SEis). We hope that our and others’ continued work on this topic will improve equity in healthcare for all patients.
Supplemental Material
sj-docx-1-mde-10.1177_23821205231203783 - Supplemental material for Design, Implementation, and Evaluation of an Intensive Course on Issues in Women's Health and Gender-Based Medicine
Supplemental material, sj-docx-1-mde-10.1177_23821205231203783 for Design, Implementation, and Evaluation of an Intensive Course on Issues in Women's Health and Gender-Based Medicine by Maricedes Acosta-Martínez, Latha Chandran, Siobhan Cohen and Anat Biegon in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205231203783 - Supplemental material for Design, Implementation, and Evaluation of an Intensive Course on Issues in Women's Health and Gender-Based Medicine
Supplemental material, sj-docx-2-mde-10.1177_23821205231203783 for Design, Implementation, and Evaluation of an Intensive Course on Issues in Women's Health and Gender-Based Medicine by Maricedes Acosta-Martínez, Latha Chandran, Siobhan Cohen and Anat Biegon in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205231203783 - Supplemental material for Design, Implementation, and Evaluation of an Intensive Course on Issues in Women's Health and Gender-Based Medicine
Supplemental material, sj-docx-3-mde-10.1177_23821205231203783 for Design, Implementation, and Evaluation of an Intensive Course on Issues in Women's Health and Gender-Based Medicine by Maricedes Acosta-Martínez, Latha Chandran, Siobhan Cohen and Anat Biegon in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The authors thank the guest speakers and students for their participation in the class, which made this research study possible.
Author Contributions
MA-M: Data collection, data analysis, writing of all manuscript sections, and revisions. LC: Manuscript revisions. SC: Data collection and data analysis. AB: Design of course, data analysis and manuscript revisions. All authors discussed the results and contributed to the final manuscript.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.