
Abstract
Introduction
Diabetic foot ulcer is a common complication of diabetes that significantly impacts the quality of life of individuals.
Objective
This study aimed to assess patients’ knowledge and attitudes on the prevention of diabetic foot ulcers and identify their predictors among adult diabetic patients at selected hospitals in Ethiopia.
Methods
Institution-based cross-sectional study design was employed among 374 patients selected by simple random sampling in three selected hospitals from February to June 2024. Data were entered using EpiData version 3.1 and exported to SPSS version 25 for analysis. Bi-variable and multivariable logistic regression were employed at 95% confidence intervals to identify significant predictors for knowledge and attitude toward the prevention of diabetic foot ulcers.
Results
Out of 380 study participants, 374 completed the study, giving a response rate of 97.4%. The mean age of participants was 46.06 (SD,13.5) years. Of the total participants, 226 (60.4%, 95% CI: 55.3%–65.4%) had good knowledge about diabetic foot ulcer prevention. About 294 (78.6%, 95% CI: 74.0%–82.7%) patients had positive attitudes. Residence, age, educational status
Conclusion
Nearly half of the participants had good knowledge, and about three-fourths had a positive attitude toward diabetic foot ulcer prevention. Factors such as older age, higher education, urban residence, being married, and a history of foot problems were significantly associated with good knowledge. Similarly, good knowledge and being married were linked to a positive attitude. Although the attitude level is relatively high, the gap in knowledge highlights the need for targeted educational interventions, especially for individuals with a lower educational level and those residing in rural areas.
Background
Diabetes mellitus (DM) is a chronic and complicated metabolic disease that needs ongoing, proper care to maintain normal blood glucose levels and reduce complications (Cefalu et al., 2018). Continuous clinical training for handling, avoiding, and educating diabetic patients is important for controlling their severe and persistent consequences (Gerber & Sharp, 2013). In Southern Ethiopia, diabetes has emerged as a major public health issue, leading to an increasing number of patients visiting diabetic clinics for continued care (Demisse Andarge et al., 2024; Zekewos et al., 2018).
Although diabetic patients face numerous challenges, diabetic foot ulcer (DFU) stands out as a particularly serious complication (Mariam et al., 2017). DFUs represent one of the most prevalent and serious complications associated with diabetes, leading to considerable suffering and mortality around the globe (Mekonnen, 2024). The worldwide occurrence of DFUs is estimated to range between 4% and 10%, with the rate rising as the population ages and more individuals are diagnosed with diabetes (Zhang et al., 2017).
The prevalence of diabetes mellitus in Ethiopia ranges from 2.0% to 6.5%, and the overall prevalence of diabetic foot ulcer was 12.98% (Bishu et al., 2019; Tolossa et al., 2020).
Also, there has been an increasing number of diabetic patients visiting follow-up clinics; however, the rate of DFUs in the area remains elevated, with numerous individuals suffering from serious foot issues like infections and amputations (Abate et al., 2020). Common clinical symptoms of DFU include pain in the foot, loss of feeling in the foot, ulceration, loss of joint motion, development of an abscess, and changes in color and temperature of the foot as gangrene progresses (Armstrong et al., 2017). Peripheral artery disease(PAD) is the most frequent cause of DFU. Risk factors include poor blood glucose control, poor metabolic control, foot abnormalities, advanced age, peripheral vasculopathy, lack of diabetes education, shoe pressure, smoking, and peripheral neuropathy (Shamim et al., 2021).
Globally, DFU could be a major medical, social, and financial issue. In most developed nations, the yearly rate of foot ulceration among individuals with diabetes is about 2% (Wild et al., 2004). Diabetic foot injury may be a devastating condition since it increases the rate of disability and even death of diabetic patients. In severe circumstances, foot ulcers might result in limb amputation, further bacterial infections of the lesions, and recurrent hospital stays (Azene et al., 2020; Driver et al., 2010; Khanolkar et al., 2008). Not only is it linked to a high risk of mortality, morbidity, and disability, but it also negatively affects diabetic people psychologically. According to research in Ethiopia, 15% of diabetes people may experience diabetic foot lesions at some point during their disease (Amogne et al., 2011).
Various factors impact diabetic patients’ knowledge and attitude toward foot care. Demographic attributes like age, gender, educational attainment, and socioeconomic background significantly contribute to forming a patient's awareness and perceptions (Alharbi & Sulaiman, 2022). For instance, elderly patients with less education frequently exhibit a limited understanding of foot care related to diabetes and are less inclined to engage in preventive practices (Bhattacharya et al., 2021). Likewise, those with fewer financial resources might encounter obstacles in accessing health education, necessary resources, and appropriate footwear, which can lead to unfavorable perceptions about foot care (Carvalho Neto et al., 2022).
One of the key elements in preventing DFUs is the knowledge and attitude of individuals with diabetes concerning foot care. Research has indicated that a significant number of diabetic patients lack knowledge about the significance of routine foot examinations, appropriate footwear, and the urgency of addressing any cuts or injuries swiftly (Aljaouni et al., 2024; Metwally et al., 2023).
DFU is avoided with sufficient understanding of the condition and consistent evaluation of the foot (Adeyemi et al., 2021). More than 40% of people with diabetes and foot ulcers require enough knowledge and training on proper foot care techniques. The fast-expanding rate of foot ulcers requires productive preventive and administrative measures for the decrease and care of diabetic foot ulcers (Buchanan et al., 2023).
High-risk patients can be identified early if the causes of foot problems in diabetics are known. Therefore, attaining good glycemic control in individuals with DM requires knowledge and attitude concerning infections, drugs, and lifestyle (Navaneeth et al., 2017).
In Sudan, 56.5% had good foot care knowledge, while 70.5% had a poor attitude (Mohammed & Rahman, 2018). A study in North China found that only 51.6% and 63.9% of participants had moderate knowledge and a positive attitude toward foot care prevention, respectively (Jia et al., 2022). A study in Eastern Ethiopia revealed that only 52.5% of patients had adequate diabetes knowledge (Letta et al., 2023). Lack of knowledge and negative perceptions regarding foot care significantly influence the emergence and advancement of DFUs. Insufficient knowledge of foot care leads to the neglect of vital practices like consistent foot examinations, proper hygiene, and wearing suitable footwear (Jia et al., 2022).
Diabetic individuals who do not recognize the dangers of foot ulcers are less inclined to participate in preventive actions, such as inspecting their feet daily or consulting healthcare professionals when they observe irregularities (Bossman et al., 2021). The lack of knowledge and attitude regarding DFU prevention among diabetic individuals in Ethiopia is a key factor exacerbating this problem. Research indicates that a considerable number of diabetic patients in Ethiopia are unaware of the necessity for daily foot checks, appropriate footwear, and the possible dangers linked to untreated foot injuries (Belsti et al., 2020; Letta et al., 2023).
Although follow-up clinics exist for individuals with diabetes, there is a lack of extensive research regarding their knowledge, attitudes, and factors influencing foot care practices within this group in the area of studies. Therefore, this study aimed to fill this gap by assessing diabetic patients’ levels of knowledge, attitude, and their predictors toward the prevention of DFU among adult patients attending a diabetic follow-up clinic at public hospitals.
Review of Literature
Several studies across different countries have assessed diabetic patients’ knowledge and attitudes toward the prevention of diabetic foot ulcers. In Thailand, a 2014 study reported a moderate level of knowledge among diabetic patients (66%) (Phoosuwan et al., 2022). Similar cross-sectional and observational studies in India from 2015 to 2019 revealed that knowledge varied widely, with good knowledge ranging from 31% to 58% and some participants lacked satisfactory awareness (Maniktalla et al., 2025). A 2020 qualitative study in Tobago highlighted poor knowledge but good awareness of specific foot care practices, like inspection and appropriate footwear (Vincent-Edinboro & Onuoha, 2022). In Sudan, only 46.7% of participants had good knowledge of diabetic foot self-care (Ahmed et al., 2019). In Ethiopia, studies conducted in Bahir Dar and Dessie reported knowledge levels ranging between 43.8% and 68.3%, with one study finding that over 61% of participants had good knowledge of diabetic foot self-care (Tuha et al., 2021a; Yohanis et al., 2020). These findings suggest significant variation in knowledge levels, influenced by location and study design.
Regarding attitude, studies from Thailand, India, Saudi Arabia, Brazil, Ghana, Indonesia, and Ethiopia present mixed findings. In Thailand (Phoosuwan et al., 2022), 75.3% of participants had a high attitude score, while in Saudi Arabia (Almaghrabi et al., 2024), a study reported that 86.4% had poor attitudes toward diabetic foot care, whereas another showed favorable attitudes among educated individuals. In India and Brazil, most patients exhibited a positive attitude, with some studies showing up to 89% holding a positive view (Chellan et al., 2012). Despite poor knowledge, Tobago's participants demonstrated good attitudes (Bahall & Legall, 2017).
Objectives of the Study
To determine patients’ knowledge toward prevention of diabetic foot ulcer among adult diabetic patients attending a diabetic follow-up clinic in Gurage zone, Southern Ethiopia, 2022.
To assess patients’ attitudes toward the prevention of diabetic foot ulcer among adult diabetic patients attending a diabetic follow-up clinic, in Gurage zone, Southern Ethiopia, 2022.
To assess the predictors of knowledge and attitude toward prevention of diabetic foot ulcer among adult diabetic patients attending a diabetic follow-up clinic, in Gurage zone, Southern Ethiopia, 2022.
Methods
Study design: Institutional-based cross-sectional study design was employed.
Study Setting and Period
The study was conducted at three selected hospitals in Gurage zone, Ethiopia, which are Wolkite University specialized teaching hospital, Attat primary hospital, and Butajira primary hospital. The capital of the Gurage zone is a town located 158 km southwest of Wolkite, the capital city of the country. It is a densely populated zone with a total population of 3,567,377 and an area of 5,893.40 km² according to the 2015 census. The zone has one general hospital, seven primary hospitals, 72 health centers, and 412 health posts. The study was conducted at randomly selected hospitals in the Gurage zone from February 1 to June 1, 2024.
Source population: all adult diabetic patients attending diabetic follow-up clinics in the Gurage zone were the source population.
Study population: all selected adult diabetic patients who were attending diabetic follow-up clinics in selected hospitals during the data collection period were the study population.
Eligibility criteria: The study included all type one and type two diabetic patients over the age of 18 who were visiting a diabetic follow-up clinic and were willing to take part. Whereas patients who were critically ill and unable to communicate during data collection were excluded from the study.
Sample Size Determination
The sample size was calculated by using a single population proportion formula with the assumptions of a 95% confidence interval (CI), a 5% margin of error, and the proportion of the population in the previous study was 66% (Bekele & Berhanu, 2021).
n = sample size
p = 66%, the maximum estimated population proportion taken from patients who had competent practice from the previous study.
d = 5% (margin of error)
Z = 1.96 (standard normal deviation value corresponding to 95% confidence level)

Therefore, by adding 10% for the possible non-response rate, the final sample size was 380.
Sampling Technique and Procedure
The three hospitals (Wolkite University Specialized Teaching Hospital, Attat Primary Hospital, and Butajira Primary Hospital) were selected by a lottery method. A simple random sampling technique was also employed to select the study participants. The proportionate allocation formula was then used to distribute the sample size across the selected hospitals (Figure 1).

Schematic Presentation of Selecting Study Setting and Sample on the Knowledge, Attitude, and Their Predictors Toward Prevention of Diabetic Foot Ulcer, 2024
Data Collection Tool and Procedure
An interview-administered structured questionnaire was used to collect data. The structured questionnaire includes four sections: the first section is on socio-demographic profile with eight questions, the second is clinical characteristics with seven questions, the third is knowledge related to the prevention of diabetic foot ulcers with 10 questions, and the fourth is attitude-related with sixteen questions. Internal consistency of the knowledge and attitude sections was assessed using Cronbach's alpha, and the results were 0.79.
The diagnosis of diabetes mellitus was verified by reviewing the patients’ medical records. Trained BSc nurses were responsible for recruiting participants by approaching them after their clinical care. The same nurses conducted face-to-face interviews with the participants and collected the necessary data using a structured questionnaire. The data collection process was supervised by an additional team of BSc nurses to ensure adherence to the study protocol and maintain data quality.
Dependent Variable
The dependent variables were knowledge (Good/Poor) and attitude (Positive/Negative) toward preventive measures for diabetic foot ulcers.
Independent Variables
The independent variables were: age, gender, ethnicity, place of residence, religion, educational level, marital status, occupation, type of diabetes, foot ulcer information, disease duration, and physician foot examination were independent variables.
Operational Definitions
Diabetic foot ulcer: a diabetic foot ulcer is defined as any necrosis, gangrene, or full-thickness skin defect occurring distal to the ankle in diabetic patients (Al-Hariri et al., 2017).
Knowledge level: knowledge of patients about diabetic foot ulcers and foot care prevention was assessed by using 10 closed-ended questions with two options. A correct answer was coded as “1” and an incorrect answer as “0”; then a score was computed. Patients were labeled as having good knowledge of diabetic foot ulcers if the score was greater than or equal to the mean and had poor knowledge if the score was less than the mean (Bago, 2017). The mean score of the participants’ knowledge was 5.05.
Attitude level: the attitude of patients regarding diabetic foot ulcer and foot care prevention was assessed by using 4 closed-ended questions with two options. Patients were classified as having a positive attitude toward diabetic foot ulcers if their score was greater than or equal to the mean, and having a negative attitude if their score was lower than the mean (Bago, 2017). The mean score of the participants’ attitude was 2.83.
Data Quality Assurance and Control
Training for supervisors and data collectors was provided over one day, covering sample size, data extraction, ethical issues, and methods of supervision. Before entering data, the collected data was reviewed and checked for completeness, and any incomplete data was discarded. Furthermore, a pre-test was done on 5% of study participants at a Primary Hospital to check the reliability of the questionnaire (Cronbach's alpha of 0.79). This pretest also aimed to assess the clarity of the data collection tools and estimate the average time required for each respondent to complete the questionnaire. Epi Data was used for data entry to prevent data entry errors.
Ethics Approval and Participant Informed Consent
Before conducting the study, the proposal was presented and defended at Wolkite University College of Health Sciences. Ethical clearance was obtained from the Institutional Review Board (IRB) of Wolkite University. The IRB reviewed the study protocol and approved it. Written informed consent was taken from the participants. The data were not disclosed to any person other than the principal investigator. Confidentiality of the information was maintained throughout the study.
Data Processing and Analysis
After data collection, each questionnaire was checked for completeness, and a code was given before data entry. Data cleaning was done by the software. Frequency, percentage, cross-tabulation, and descriptive summaries were used to describe the data. Data were exported and analyzed using SPSS version 25. The model fitness test was checked by the Hosmer-Lemeshow test, and it was well fitted with a p-value of 0.44. Multicollinearity was checked by using variance inflation factors, with a maximum of 1.55 variance inflation factors. The association of dependent and independent variables was assessed by using binary logistic regression. Those independent variables with a p-value of 0.25 with a 95% confidence interval in bivariable logistic regression were chosen as candidates for the multivariable logistic regression model. The adjusted odds ratio (AOR) with a p-value of 0.05 and 95% confidence interval (CI) was used to declare significant factors.
Results
Characteristics of Study Participants
Out of 380 study participants, 374 completed the study, giving a response rate of 97.4%. Among them, 212(56.7%) were males. The age of participants ranged from 20 to 88 years old, with a mean age of 46.06. A total of 99 (26.4%) of the study participants were in the 40–49 age range.
Out of the total participants, 166 (44.4%) patients were from rural areas, while 208 (55.6%) were from urban). The Majority of the participants, 269 (71.9%), were from
Characteristics of Adult Diabetic Patients Attending a Diabetic Follow-Up Clinic in Gurage Zone on Knowledge, Attitude, and Predictors Toward Prevention of Diabetic Foot Ulcer, 2024 (N = 374).

Knowledge of Patients on Prevention of Diabetic Foot Ulcer
In general, 148 (39.6%, 95% CI: 34.6%–44.7%) had poor knowledge and 226 (60.4%, 95% CI: 55.3%–65.4%) of participants had good knowledge about diabetic foot ulcer prevention.
Associated Factors of Knowledge on Prevention of Diabetic Foot Ulcer
Age, marital status, level of education, rural residence, and history of diagnosed foot ulcer were found to be significantly associated with knowledge of diabetic foot ulcer prevention in the multivariable analysis. This study found that increasing patients of the age were nearly four times more likely to have good knowledge of diabetic foot ulcer prevention. Moreover, age group of 30–39 had about 3 times (AOR 2.97, 95% CI 1.12–7.87), age group of 40–49 had about 6 times (AOR 6.34, 95% CI 2.17–18.17) and age ≥50 had 3 times (AOR 3.11, 95% CI 1.03–9.43) more likely had good knowledge of diabetic foot ulcer prevention compared to those with age group of 18–29.
Patients widowed on marital status were 10 times more likely to have good knowledge (AOR 10.4, 95% CI 1.48–13.3) than married. Additionally, patients with a college education or higher demonstrated significantly better knowledge of diabetic foot ulcer prevention compared to those who were uneducated (AOR = 0.07; 95% CI: 0.02–0.21), had only completed primary school (AOR = 0.16; 95% CI: 0.06–0.44), or secondary school (AOR = 0.21; 95% CI: 0.08–0.55), respectively.
This study revealed that diabetic patients living in rural areas were twice as likely (AOR = 0.5, 95% CI: 0.29, 0.86) to have poor knowledge of diabetic foot ulcer prevention compared to those residing in urban areas. Furthermore, patients with a history of foot problems had 26% lower odds of having good knowledge of diabetic foot ulcer prevention compared to those without a history of foot problems (AOR = 0.74, 95% CI: 0.16–0.78) (Table 2).
Associated Factors of Knowledge Toward Prevention of Diabetic Foot Ulcer at Selected Hospitals, 2024.

COR: crude odds ratio, AOR: adjusted odds ratio, DM: diabetes mellitus, and any p-value calculated as 0.000 is rounded and presented as <0.001. Bold indicates significant var.
Attitude of Patients on the Prevention of Diabetic Foot Ulcer
About 294 (78.6%, 95% CI: 74.0%–82.7%) patients had positive attitudes toward the prevention of diabetic foot ulcers, whereas 80 (21.4%, 95% CI: 17.3%–26.0%) had negative attitudes. More than half of patients, 222 (59.4%), agreed that regular exercise prevents further complications in diabetic patients, about 217 (58.0%) of patients agreed that dietary modification is important to prevent diabetic foot ulcers, and about 217 (58.0%) agreed to use special footwear advised by the foot-care specialist.
Associated Factors of Patients’ Attitudes on the Prevention of Diabetic Foot Ulcer
Multivariable logistic regression analysis showed that individuals exhibiting suboptimal levels of knowledge had 63% lower odds of possessing a positive attitude compared to those with adequate knowledge [AOR = 0.37; 95% CI: 0.18–0.73]. Furthermore, individuals within the age bracket of 30–39 years were approximately 12.7 times more likely (AOR 12.72, 95% CI 3.26–49.57), individuals aged 40–49 were about 8 times more likely (AOR 8.45, 95% CI 2.08, 34.37), and individuals aged 50 years and above were 14 times more likely (AOR 14.0, 95% CI 2.98, 66.15) to exhibit a positive attitude toward the prevention of diabetic foot ulcers in comparison to those aged 18–29 years. Patients with a marital status of divorced had 81% lower odds of possessing a positive attitude compared to those who were married (AOR = 0.19; 95% CI: 0.05–0.66) (Table 3).
Associated Factors of Attitude Toward Prevention of Diabetic Foot Ulcer Using Binary Logistic Regression, 2022.
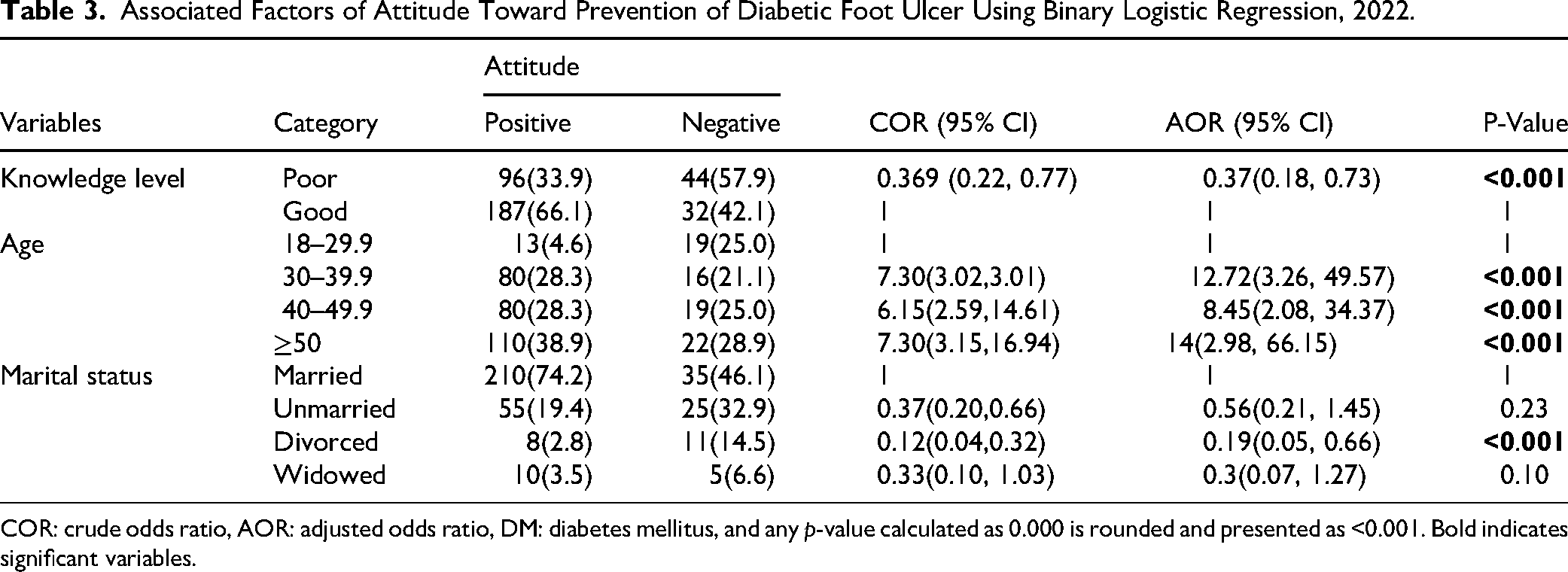
COR: crude odds ratio, AOR: adjusted odds ratio, DM: diabetes mellitus, and any p-value calculated as 0.000 is rounded and presented as <0.001. Bold indicates significant variables.
Discussion
This study was conducted to assess knowledge, attitude, and their predictors toward the prevention of diabetic foot ulcers among adult diabetic patients in Gurage zone, Ethiopia. The result from the study expands existing reports and could serve as a footnote for further studies on related subjects.
This study revealed that nearly two-thirds of the patients, 226 (60.4%), with 95% CI (55.3, 65.4%) had good knowledge of diabetic foot ulcer prevention. This is in line with other studies done in northeast Ethiopia (61.3%) (Tuha et al., 2021b), Felege Hiwot referral Hospital (56.2%), Bahir Dar, Ethiopia, respectively (Navaneeth et al., 2017), Dessie referral hospital (61.3%) (Jia et al., 2022), and another hospital-based prospective observational study in India showed that the majority (58%) of patients had good knowledge (Zekewos et al., 2018)
In contrast, this study was found to be higher than studies done in India (4%) (Mulki et al., 2019), Sudan (46.7%) (Metwally et al., 2023) The possible reasons for the variation in the report might be due to differences in the socio-demographic characteristics of the patients and access to information regarding diabetes and its complications.
In this study, age, marital status, level of education, rural residence, and history of foot problems were significantly associated with knowledge regarding the prevention of diabetic foot ulcer.
In this study, increasing age was significantly associated with better knowledge of DFU prevention. Older participants, particularly those in the 40–49 age group, demonstrated a higher level of knowledge. This pattern suggests that increased age may be associated with greater exposure to relevant information, accumulated life experience, or a heightened sense of responsibility that contributes to better understanding. Such findings highlight the importance of considering age-related factors when designing educational interventions or awareness programs, as younger populations may require more targeted efforts to improve knowledge levels.
This finding is consistent with previous research, which suggests that older patients tend to have better knowledge about diabetes-related complications due to longer exposure to healthcare services and more frequent interactions with healthcare providers (Truong, 2022). The higher knowledge in older age groups may also be attributed to accumulated experiences and healthcare education over time, reinforcing the importance of age in patient education.
Marital status also appeared to influence DFU knowledge, with widowed individuals demonstrating notably better understanding compared to those who were married. This is an intriguing finding and contrasts with some studies that have shown no significant correlation between marital status and health knowledge. However, it could be hypothesized that widowed individuals may have a greater need for self-care and education due to the absence of a primary caregiver, possibly leading to greater awareness of diabetic complications and foot care (Karimi et al., 2025). On the other hand, married individuals may have more direct support and reliance on spouses for information, which could influence their perceived need to learn more about DFU prevention.
Educational level also emerged as a key factor in knowledge levels, with individuals having a college education or higher exhibiting significantly better knowledge compared to those with lower levels of education. This finding is consistent with several studies, which have shown that higher educational attainment is strongly associated with improved health literacy and self-care behaviors in diabetes management (Chen et al., 2022; McGowan, 2011). This relationship highlights the importance of incorporating educational programs that are accessible to individuals of all educational backgrounds to ensure effective disease management and prevention of complications like DFU.
The study also found that diabetic patients living in rural areas were more likely to have poor knowledge of DFU prevention. Patients residing in rural areas may face challenges such as limited access to healthcare services, lower health literacy, and fewer educational resources, all of which may contribute to poorer health outcomes and less knowledge about diabetes care (Ma et al., 2023). This finding underscores the need for targeted health education interventions in rural areas to bridge the knowledge gap.
Interestingly, patients with a history of foot problems were less likely to have good knowledge about DFU prevention, which may suggest gaps in patient education or missed opportunities for targeted counseling during previous healthcare encounters. This result is somewhat surprising given the assumption that individuals with a history of foot issues might be more vigilant about foot care. However, it could suggest a level of complacency or inadequate management of foot care in individuals who have already experienced complications, a phenomenon observed in other chronic conditions where previous adverse experiences do not always lead to improved preventative behaviors (Ababneh et al., 2023). It may also reflect a need for more tailored education for these patients to emphasize the importance of prevention even after experiencing foot issues.
On the other hand, the study found that a large majority of patients demonstrated a positive attitude toward the prevention of diabetic foot ulcers, indicating generally favorable perceptions and awareness of the importance of preventive measures. The findings of this study reveal that a significant proportion of diabetic patients exhibited positive attitudes toward the prevention of diabetic foot ulcers, while a smaller portion held negative attitudes, highlighting the overall encouraging mindset among patients but also suggesting the need for targeted interventions to address remaining gaps. Also, this is nearly similar to a study done in India (76.2%) (Wankum et al., 2014). However, it is higher than a study conducted in northwest Ethiopia (65.2%) (Tuha et al., 2021b). The revealed difference in reporting among the studies could be attributed to differences in socio-demographic background, knowledge differences, and access to health education regarding the subjects. The positive attitudes observed in this study underscore the importance of fostering a proactive approach to DFU prevention, which could be further enhanced through education and intervention.
One key finding of this study was the significant association between knowledge and attitudes, where patients with limited knowledge were notably less likely to exhibit a positive attitude toward DFU prevention. This underscores the importance of educational interventions in shaping favorable attitudes and promoting preventive behaviors. This is in line with previous studies, which have shown that better knowledge of diabetes complications correlates with more positive health behaviors and attitudes (Chiwanga & Njelekela, 2015; Ramirez-Perdomo et al., 2019). These studies have highlighted that diabetic patients with a higher level of knowledge regarding foot care are more likely to engage in preventative actions and have a more proactive attitude toward managing their condition. This emphasizes the critical role of patient education in shaping attitudes and preventing complications such as DFUs.
Age also emerged as a significant factor influencing attitudes toward DFU prevention. Patients aged 30 years and older were more likely to exhibit a positive attitude toward DFU prevention compared to younger individuals, with the strongest association observed among those aged 50 and above. This may reflect increased health awareness or greater exposure to diabetes-related education and care with advancing age. This finding supports the results of several studies, which suggest that older individuals, with their longer duration of diabetes, often develop a stronger sense of responsibility for their health and are more likely to adopt health-promoting behaviors (Abdissa et al., 2020; Ramirez-Perdomo et al., 2019). The increased experience with diabetes management and healthcare interactions likely contributes to a more knowledgeable and proactive approach to foot care in older populations.
In contrast, marital status showed a distinct influence on attitudes, with divorced individuals being notably less likely to exhibit a positive attitude toward DFU prevention. This may indicate that social or emotional factors related to marital status affect patients’ engagement with preventive measures. This result aligns with some previous studies that have suggested marital status may influence health outcomes, with married individuals generally demonstrating better health behaviors due to the support provided by their spouse (Trief et al., 2004). The lack of a spouse may reduce the emotional and social support necessary for effective disease management, which could explain the less favorable attitudes observed in divorced individuals.
Implications for Research and Practice
Implications for research: This study underscores the need for further research to explore the behavioral and systemic factors influencing foot care practices among diabetic patients. Specifically, we recommend prospective cohort studies to identify causal relationships and determinants of self-care practices related to DFU prevention. Future research should also explore intervention-based studies that test the effectiveness of structured foot care education programs in improving patients’ knowledge, attitudes, and practices. Additionally, qualitative research could help uncover the cultural, psychological, and health system barriers that hinder effective foot care among diabetic individuals in Ethiopia and similar settings.
Implications for practice: The findings of this study highlight an urgent need to strengthen diabetic foot care education, especially among vulnerable subgroups such as patients with low educational attainment, those residing in rural areas, and individuals with a history of foot complications. These groups demonstrated comparatively lower levels of knowledge and awareness regarding diabetic foot ulcer (DFU) prevention. Healthcare providers, particularly those working in diabetic follow-up clinics, should be supported to integrate structured and regular foot care counseling into routine consultations. Educational strategies should emphasize early identification of foot problems, proper hygiene, appropriate footwear, and the importance of daily foot inspection. Additionally, health authorities and policymakers should consider implementing community-based diabetes education programs tailored to low-literacy populations.
Implications for nursing practice: The findings of this study highlight the crucial role of nurses in preventing diabetic foot ulcers through patient-centered education and support. Limited knowledge and unfavorable attitudes among diabetic patients indicate a need for nurses to strengthen health education programs focusing on foot care practices, early detection of complications, and lifestyle modifications.
Strengths and Limitations of This Study
This study presents both strengths and limitations that are important to consider. It focuses on the prevention of diabetic foot ulcers, a significant health concern among diabetic patients, thereby addressing a critical aspect of diabetes management. The study provides valuable baseline data on patients’ knowledge and attitudes at a specific point in time, offering insights that can inform targeted interventions. Conducted within a healthcare facility, its findings are directly applicable to clinical settings, enhancing their practical relevance. However, the cross-sectional design limits the ability to establish causality or observe changes over time. Additionally, the reliance on self-reported data may introduce recall bias or inaccuracies, potentially affecting the validity of the findings.
Conclusion
Nearly half of the study participants had good knowledge and good practice, and a fourth of the participants had positive attitudes toward diabetic foot ulcers. Age, marital status (widowed), level of education, occupation (NGO employed), rural residence, and history of diagnosed foot ulcer are found to be significantly associated with the knowledge of participants. Knowledge level, age, and marital status (divorced) were found to be significantly associated with a patient's attitude toward the prevention of diabetic foot ulcer. Similarly, knowledge level, age, marital status, and history of patients who had foot examinations are also found to be significantly associated with practice.
Footnotes
Abbreviations and Acronyms
Acknowledgments
First, we would like to thank Wolkite University for giving us the chance to conduct this work. Second, we would like to thank the Gurage Zone Hospital staff working at the DM Clinic. We would also like to give our appreciation to the data collectors and supervisors for their efforts.
Ethics Approval and Participant Consent
Before conducting the study, the proposal was presented and defended at Wolkite University College of Health Sciences. Ethical clearance was obtained from the Institutional Review Board (IRB) of Wolkite University. The IRB reviewed the study protocol and approved it. Written informed consent was taken from the participants. The data were not disclosed to any person other than the principal investigator. Confidentiality of the information was maintained throughout the study.
Consent to Publication
Although photographs or videos linked to an individual's recorded data are not included in the study, there is no dispute about consent to publish other data obtained.
Authors’ Contribution
BTA: conceptualization, data curation, formal analysis, investigation, methodology, software, validation, resources, supervision, writing—original draft, review and editing, MK: conceptualization, formal analysis, methodology, resources, software, supervision, TTT: conceptualization, resources, formal analysis, investigation, methodology, software, visualization, writing—review and editing and preparing the manuscript, DT and FAG: conceptualization, formal analysis, investigation, methodology, resources, software, supervision, validation, writing—review and editing. All authors reviewed, discussed, agreed to their contributions, and read and approved the final draft of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The data set used and analyzed during the current study is available from the corresponding author upon reasonable request.
Patient and Public Involvement
Study participants WERE NOT involved in the design, conduct, or reporting, or dissemination plans of our research.