
Abstract
Introduction
It is important to reduce foot problems by preventing the recurrence of ulcers in diabetes mellitus (DM) patients. In Indonesia, interventions for the prevention of ulcer recurrence remain scarce.
Objective
The present study aimed to evaluate the validity and efficacy of a proposed intervention model for preventing the recurrence of ulcers in DM patients.
Method
Sixty-four DM patients were selected to participate in this quasi-experimental study and divided into two groups: intervention (n = 32) and control (n = 32). The intervention group received preventive treatment while the control group received standard care. Two trained nurses supported this study.
Results
Of the 32 participants in the intervention group, 18 (56.20%) were male, 25 (78.10%) were non-smokers, 23 (71.90%) had neuropathy, 14 (43.80%) had foot deformities, four (12.50%) had recurring ulcers, and 20 (62.50%) had a previous ulcer < 12 months ago. Of the 32 participants in the control group, 17 (53.10%) were male, 26 (81.25%) were non-smokers, 17 (46.90%) had neuropathy, 19 (69.40%) had foot deformities, 12 (37.50%) had recurring ulcers, and 24 (75.00%) had a previous ulcer < 12 months ago. The mean (SD) age [62 (11.28) and 59 (11.11) years], ankle-brachial index [1.19 (0.24) and 1.11 (0.17)], HbA1C [9.18 (2.14%) and 8.91 (2.75%)], and DM duration [10.22 (6.71) and 10.13 (7.54)] of the intervention and control groups did not differ significantly. The content validity of the proposed intervention model was strong (I-CVI > 0.78). When the proposed screening tool for predicting the risk of ulcer recurrence in DM patients (NASFoHSkin) was used in the intervention group, its predictive validity, sensitivity, and specificity were 4, 100%, and 80%, respectively, while in the control group it was 4, 83%, and 80%, respectively.
Conclusion
Inspection/examination, foot care, and blood glucose control can decrease ulcer recurrence in DM patients.
Introduction
Patients with diabetes mellitus (DM) often have complications, one of which is ulcers. An ulcer is a serious complication that can increase patient morbidity and has a significant socioeconomic impact (Khan et al., 2017). In addition, patients with a history of wounds are more likely experience recurrent or repeated ulcers. One study found that about 40% of patients experience a recurrence of ulcers within 1 year, 60% within 3 years, and 65% within 5 years of an ulcer healing (Armstrong et al., 2017).
Two studies reported that the prevalence of ulcer recurrence in DM patients in Indonesia was 43% and 54.3%, respectively (Arisandi et al., 2016; Soewondo et al., 2017). The high incidence of ulcer recurrence in DM patients must be prevented because this group is prone to severe complications, namely infection and amputation. As such, there is an urgent need currently for structured services and prevention models in the management of patients with DM.
Review of Literature
A systematic review by van Netten et al. (2020) reported that the prevention of ulcer recurrence in DM patients includes:
Treatment: Interventions to improve care such as podiatry, chiropody, multidisciplinary care, integrated foot care, screening interventions to detect and treat patients at risk of diabetic foot ulcers, and education by health professionals. Self-management: Interventions for patient self-management such as patient education, monitoring of foot status at home, or lifestyle interventions. Medical: Hospital-based interventions such as surgery and therapeutic footwear.
The study then developed several components; namely, integrated foot care, self-management, patient education, therapeutic footwear, and surgical intervention (van Netten et al., 2020). Comparative studies between integrated foot care and standard care for reducing wound recurrence rates in DM patients varied depending on the study (22% vs. 38%; 30.4% vs. 58.4%; 38% vs. 57%; 5.4% vs. 81.8%) (van Netten et al., 2020) with one study reporting no significant differences (38% vs. 57%). Two studies used education programs to reduce ulcer recurrence rates and reported that there were no significant differences in the reduction of ulcer recurrence between the intervention and control groups (48% vs. 38%; 41.4% vs. 41.2%) (van Netten et al., 2020).
A comparative study of patients who used therapeutic footwear and those who were given standard care to reduce ulcer recurrence reported that there was a significant difference between the intervention and control groups (9.1% vs. 25.0%) (van Netten et al., 2020) while another study did not report any significant differences between the intervention and control groups (38.8% vs 44.2%) (van Netten et al., 2020). Similarly, another study reported that no statistically significant differences between those in the control group, who wore their own shoes, and those in the intervention group, who wore therapeutic shoes. The annual re-ulceration in the control groups of these studies ranged from 8.4% to 59.3% (Chantelau et al., 2004).
As the results of studies on this subject vary significantly, more studies are required to effectively reduce ulcer recurrence in DM patients as it is important. In Indonesia, the DM management model uses the five pillars; namely, diet, physical exercise, medication, glucose monitoring, and education. However, this model has not shown satisfactory results for the prevention of ulcer recurrence (Ernawati et al., 2016).
Strategies for the prevention of ulcer recurrence in DM patients have been explored. More specifically, the provision of suitable footwear, especially for plantar ulcerations; health education, which is believed to be an important part of secondary prevention; and daily monitoring of foot skin temperature (Jeffcoate et al., 2018). However, there is currently no good evidence that demonstrates the effectiveness of these interventions and there has been contrasting results regarding the daily monitoring of skin temperature by patients (Jeffcoate et al., 2018; Lavery et al., 2007). Nevertheless, these studies do reveal that conducting multiple and regular interventions such as foot inspection, blood sugar control, and foot care prevents ulcer recurrence (Hicks et al., 2019).
In Indonesia, there is a lack of studies on the use of multiple interventions to prevent ulcer recurrence in DM patients. The purpose of the present study was to develop prevention strategies using multiple interventions, including foot inspection, foot care, and blood sugar control. In developing the prevention strategy model, this study first reviewed its validity before a direct study was conducted to examine the efficacy of the ulcer recurrence prevention strategy model. Therefore, the objective of this study was to evaluate the validity and efficacy of a preventative intervention model that contains multiple interventions to prevent ulcer recurrence in DM patients.
Methods
Content Validity: The Development of an Ulcer Recurrence Prevention Strategy Model
To develop an ulcer recurrence prevention strategy model, a review was conducted of the literature and clinical experience used in the management of foot and wound problems in DM patients. The ulcer recurrence prevention strategy consisted of three components: foot inspection, foot care, and blood sugar control. A content validity study was carried out to enable a group consensus on the topic through agreement with experts in the field. The professionals who participated in the validity study did not have access to each other's responses, thereby minimizing the possibility of them influencing each other.
The content validity of this ulcer recurrence prevention strategy model for DM patients was checked by the item-content validity index (I-CVI) through a form that was completed by the experts. The ordinal scale was dichotomized to be relevant and irrelevant, with very relevant and quite relevant given a score of 1 and somewhat relevant and irrelevant given a score of 0. The CVI is the most commonly used method of validating the content in the development of instruments and can be calculated using the I-CVI (Polit & Beck, 2006). The I-CVI is calculated as the number of experts who gave a “highly relevant” rating for each item divided by the total number of experts. Values range from 0 to 1. If the I-CVI > 0.79, the item is deemed relevant while a score of 0.70 and 0.79 indicates that the item needs to be revised and an I-CVI of < 0.70 means that the item is omitted (Polit & Beck, 2006; Rodrigues et al., 2017).
Predictive Validity
A predictive validity study was conducted to develop a tool with which to predict which patients were at risk of DM wound recurrence. The aim of this predictive validity study was to determine the level of sensitivity and specificity in DM patients at risk of ulcer recurrence.
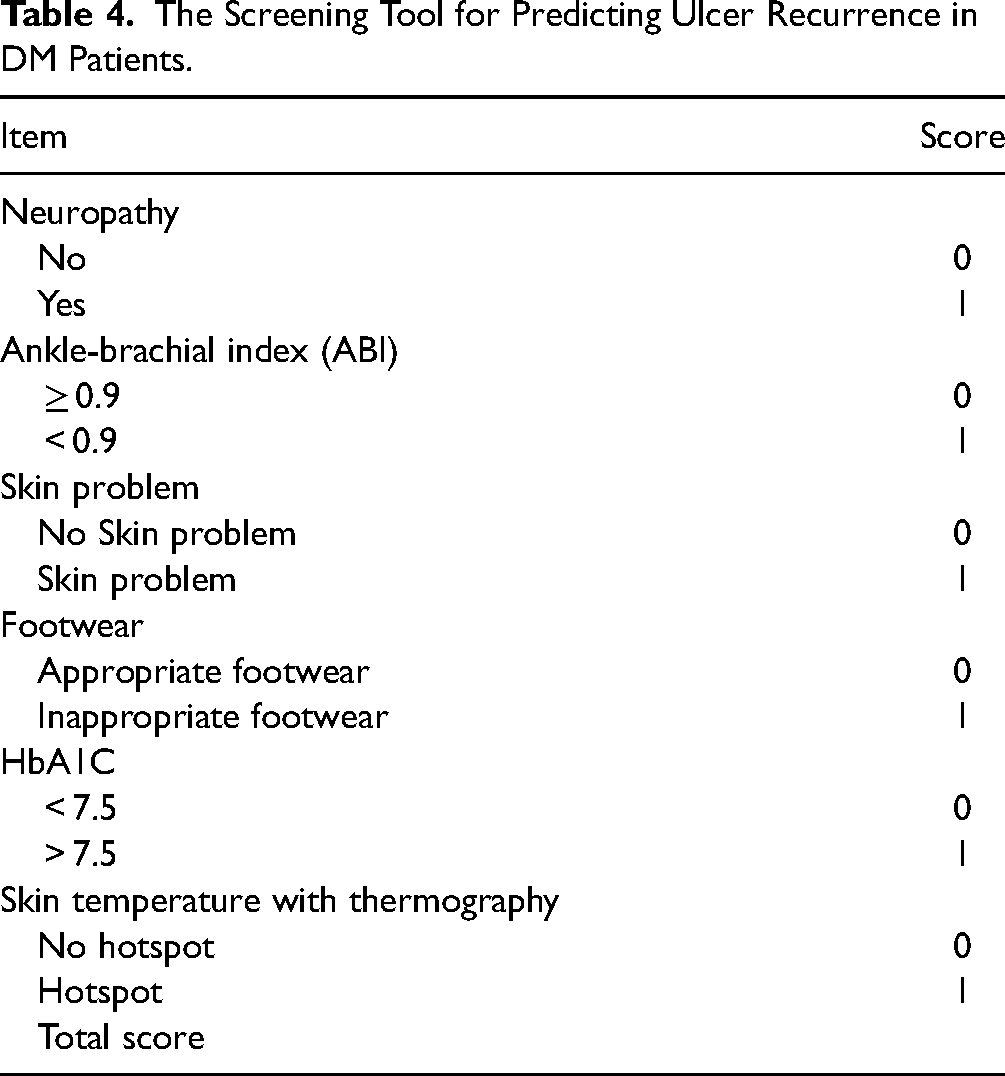
The assessment tool that was developed included components for neuropathy, ankle-brachial index (ABI), skin problems, shoes, HbA1C, and skin temperature, with scores ranging between 0 and 6. The higher the score, the higher the risk of recurrence. Six components were incorporated into a new risk screening tool for predicting ulcer recurrence in DM patients (NASFoHSkin) in Indonesia.
Participant Characteristics.

Two research assistants assessed the intervention and control groups at the beginning of the assessment before they were discharge and after six months of follow-up care.
Implementation of the Ulcer Recurrence Prevention Strategy Model
Design and Setting
This study used a quasi-experimental design. The study was conducted from August 2021 to July 2022 at the Kitamura Wound Clinic, two community health centers, and at the patient's homes in Pontianak City, Indonesia. The intervention and control groups consisted of patients who had been treated at the Kitamura Wound Clinic, two community health centers, and at their homes in Pontianak City and had recovered from their wounds.
Sample
Based on the calculated sample size, a total of 64 participants (two groups of 32 participants each) were recruited. The suggested sample size for comparing the two groups (considering = 0.05, = 0.95, p1 = 0.54.3 (Arisandi et al., 2016) and p2 = 0.11) was calculated using G*Power software.
Both groups were recruited through convenience sampling. The inclusion criteria were: healing from ulcer > 2 weeks, no complications from kidney and heart disease, able to perform daily activities, and able to carry out the instructions. The exclusion criteria were: foot infections, active foot ulcers, Charcot neuro-osteoarthropathy, chronic limb-threatening ischemia, currently using foot temperature monitoring, and severe disease or complications.
Data Collection
This study included two registered nurses with DM wound care nursing certification and more than 2 years of clinical practice experience. The participants were identified via a search of medical records followed by the investigators contacting the patients by telephone. The 32 patients contacted in the first stage were placed in the intervention group while the 32 patients contacted in the second stage were placed in the control group. The research assistants visited the 64 patients in their homes and offered interventions in-situ. Patients in the intervention group were given foot inspections, foot care, and taught methods of controlling their blood sugar while patients in the control group received follow-up care according to the standard services provided by health providers using a leaflet outlining the five pillars of DM management; namely, nutrition, pharmacological treatment, physical exercise, education, and blood sugar monitoring (Pratama et al., 2023).
The two research assistants followed the study protocol in carrying out the treatments for the intervention group with inspections of the skin on the legs and feet, especially the dorsal, plantar, medial, lateral, and posterior surfaces and toenails. The aim was to identify skin peeling and maceration or fissures in the interdigital skin and common skin disorders such as diabetic dermopathy, necrobiosis lipoidica diabeticorum, diabetic bullosa, calluses, and corns (Mooney, 2011; Pratama et al., 2023).
Bilateral pulse palpations were performed in the dorsalis pedis, posterior tibial, popliteal, and superficial femoral arteries and the skin temperature of the limbs was assessed using thermography. The filling of the subpapillary venous plexus was assessed by pressing the distal pulp of the toe until it blanched. ABI inspections were performed using a vascular Doppler (BT-200 vascular Doppler, Bistos Co. Ltd., Korea) while a monofilament test was performed to examine for peripheral neuropathy. The plantar pressure was checked with a plantar scan (Hospital Foot Imprinter Harris Mat Model FM1111, India) and the history of footwear use and of previous injuries was obtained. This was followed by a HbA1C test, the measuring of blood pressure, and a recording of the history of other diseases experienced. The final assessment was of the daily diet, history of medication (drugs/insulin), and follow-up care of the participants.
The foot care that was provided included cleaning the patient's feet using an appropriate soap, scrubbing the feet and between the toes at least five times, drying the feet with a soft cloth, using a suitable skin moisturizer (CeraVe cream) for skin conditions (not applied between the toes and plantar), using appropriate footwear according to the condition of the foot (distribution of pressure), and cutting the toenails horizontally (Pratama et al., 2023; Takehara et al., 2017). Attention was given to the presence of problems in the skin and foot deformities; such as dry and scaly skin, the presence of fissures, and foot shape such as hammer toe, claw toe, pes planus, pes cavus, crossover toe, hallux rigidus, hallux valgus, bony prominence, and metatarsal head. For the intervention to control blood sugar, the patients were given education on physical exercise, regular blood sugar control, diet, regular follow-up, proper use of DM medication, and stress management.
Data were collected during the 1- to 1.5-h intervention procedure. The data collection on the interventions was carried out once a month through inspection. Foot care and blood sugar control through education were provided at the start of the assessment. The patients were then followed up three to four times a month for up to six months.
Data Analysis
The data analysis included a descriptive analysis that was performed to determine the characteristics of the patients with and without ulcers, and the characteristic differences between patients in the two groups using a t-test (p < .05). The Statistical Package for the Social Sciences v. 22 (SPSS Inc., Chicago, IL, USA) for Windows was used in this study.
Results
The Ulcer Recurrence Prevention Strategy Model
There were 64 participants in this study, with 18 males (56.20%) in the intervention group, and 17 (53.10%) in the control group (Table 1). Most of the patients were non-smokers; 25 (78.10%) in the intervention group and 26 (81.25%) in the control group. There were 23 patients (71.90%) with neuropathy in the intervention group and 17 patients (46.90%) in the control group. In the intervention group, there were 14 patients (43.80%) with foot deformities and 19 patients (69.40%) in the control group. This study found that there were four (12.50%) ulcer recurrences in the intervention group versus 12 (37.50%) in the control group. As seen in Table 1, 20 (62.50%) participants in the intervention group and 24 (75.00%) participants in the control group had ulcer recurrence < 12 months from the previous ulcer.
There were no significant differences between intervention group and the control group with regard to the mean age (SD) [62 (11.28) and 59 (11.11) years], ABI [1.19 (0.24) and 1.11 (0.17)], HbA1C [9.18 (2.14%) and 8.91 (2.75%)], and duration of DM [10.22 (6.71) and 10.13 (7.54)], respectively of the participants, with a p-value of < .05 (Table 2).
A Comparison of the Clinical Characteristics of the Intervention and Control Groups.

SD = standard deviation.
*Significance level (p < .05).
Content Validity
This present study obtained a content validity that ranged between 0.80 and 1 (Table 3). A content validity index of the I-CVI with a value greater than 0.78 means that the tool has good content validity. The average values calculated for the components of inspection, foot care, and blood sugar control measures were 0.93, 0.96, and 1, respectively.
The Content Validity Index of the Strategy for Preventing Ulcer Recurrence of Each Model.

Predictive Validity Study
This study evaluated the predictive validity of a screening tool to predict which patients were at risk of diabetic ulcer recurrence. The NASFoHSkin screening tool that was developed had a rating range of 0 to 6 for its components and consisted of neuropathy, ABI, skin problem, footwear, HbA1C, and skin temperature (see Table 4). The higher the score, the higher the risk of recurrence.
The Screening Tool for Predicting Ulcer Recurrence in DM Patients.
The aim of the predictive validity study was to determine the sensitivity and specificity of patients at risk of ulcer recurrence. The predictive validity tests showed that the NASFoHSkin tool had a high sensitivity (100%) and specificity (80%) in the intervention group with a cut-off score of four whereas the control group had the best balance of sensitivity and specificity of 83% and 80%, respectively (Tables 5 and 6). As seen in Figures 1 and 2, the NASFoHSkin tool has an excellent AUC of 0.871 and 0.848 in the intervention and control groups, respectively.

Receiver operator characteristic curves of NASFoHSkin for with/without ulcer recurrence in the intervention group.
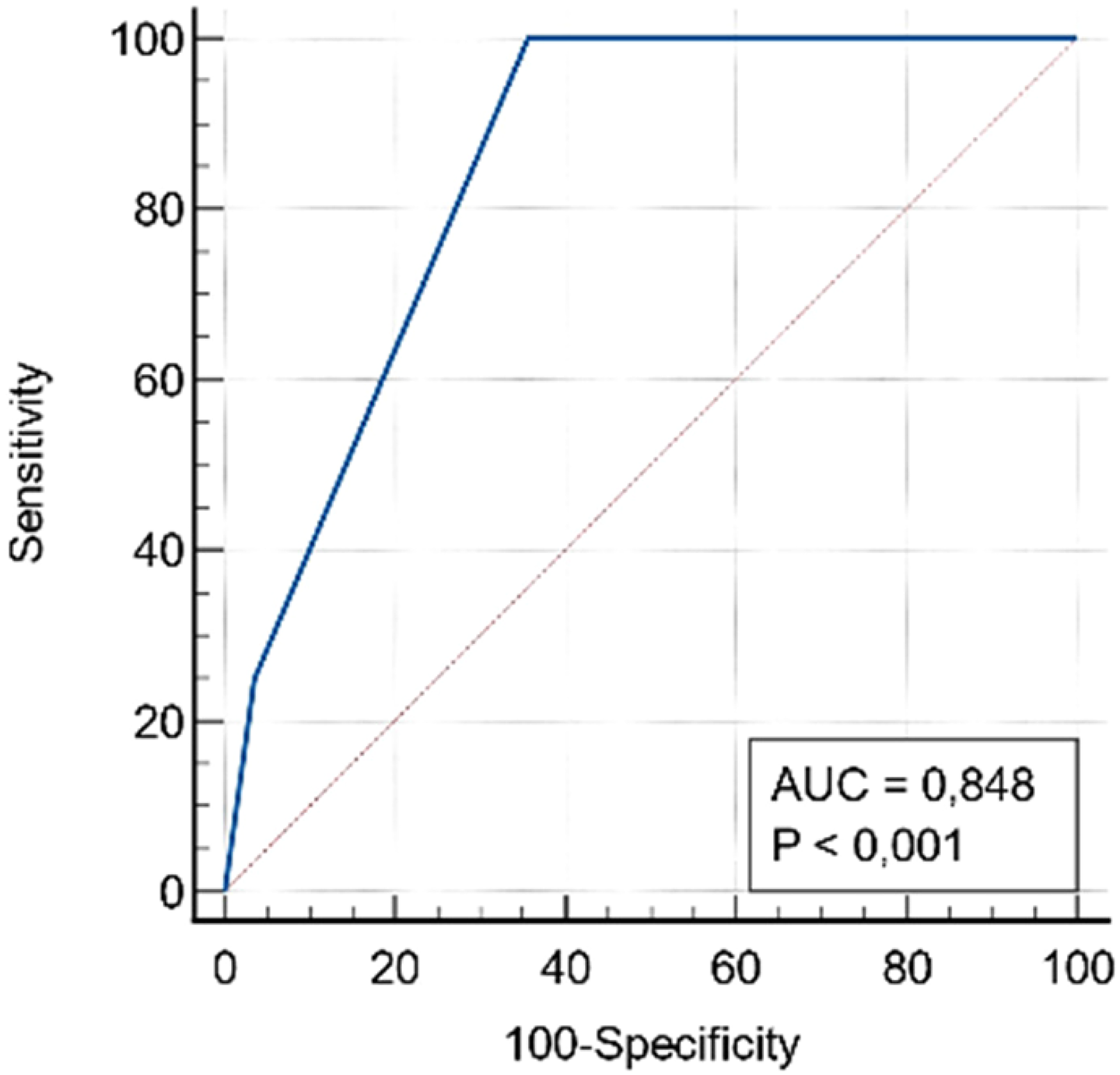
Receiver operator characteristic curves of NASFoHSkin for with/without ulcer recurrence in the control group.
The sensitivity and specificity of the NASFoHSkin scores of patients with/without ulcer recurrence in the intervention group.

The Sensitivity and Specificity of the NASFoHSkin Scores of Patients With/Without Ulcer Recurrence in the Control Group.

Discussion
This study developed a model for preventing ulcer recurrence in diabetic patients, and satisfactory results were obtained with an average content validity of 0.90 and above, which means that the developed model is very relevant (Polit & Beck, 2006).
A validity study of the NASFoHSkin tool indicated that 100% of the patients in the intervention group with a score of four or higher developed ulcer recurrence. On the other hand, the specificity was 82%, which over-predicted the development of ulcer recurrence by 18%. In the control group, the NASFoHSkin tool was able to positively identify wound recurrence 83% of the time, and under-predicted the progression of ulcer recurrence 17% of the time. In contrast, in the control group, the NASFoHSkin tool (specificity 80%) over-predicted the occurrence of ulcer recurrence by 20%.
This study demonstrated that the intervention group with a high NASFoHSkin score had ulcer recurrence, while the ulcer recurrence risk group with a high NASFoHSkin score but an over-prediction of 18% could avoid ulcer recurrence by implementing the prevention strategies developed in this study. In the control group, the non-risk group also experienced ulcer recurrence.
The study found that the model that was developed for the prevention of ulcer recurrence in diabetic patients using a combination of interventions was effective in reducing the incidence of ulcer recurrence by 12.50% compared to the control group (37.50%). Another study indicated that multiple interventions were effective in reducing the incidence of ulcers among patients with DM (0% recurrence) in the intervention group compared to the control group (24.14% recurrence) (Liang et al., 2012). Unfortunately, the study did not include patients with a history of ulcers, so it was impossible to make a comparison.
One strategy for preventing ulcer recurrence in diabetic patients is to educate them to recognize foot problems. In this study, the thermal inspection revealed an increase in the temperature of the skin of the feet, which could warn patients that the skin on their feet was prone to injury.
The research assistants followed up with the patients 3 to 4 times a month, either with a home visit or a phone call. This study seemed to support several others with regard to the strategies for preventing ulcer recurrence in patients with DM, but not across multiple interventions.
An interesting study was the daily monitoring of the skin temperature of the foot, and the resulting preventative actions. The study demonstrated a lower rate of ulcer recurrence in patients with DM (8.5%) in the intervention group compared to those who received the standard care (29.3%) (Lavery et al., 2007). However, this study was in contrast with other studies, where there was no significant difference between the monitoring of the skin temperature in the intervention group (29.1%) and the usual care group (37.3%) (Bus et al., 2021). The inspection of the feet of diabetic patients using a thermograph is crucial because it can alert patients to be careful when carrying out physical activities (Bus et al., 2021).
The incidence of ulcer recurrence in the intervention group in the current study was still relatively high compared to another study (one patient out of 41 in the intervention group) (Cisneros, 2010). The difference may be due to several factors such as the duration of DM (Cheng et al., 2021) and the HbA1C levels of > 7.5% in this study (Ata et al., 2015 ; Dubský et al., 2013).
Another possible factor could be the higher incidence of neuropathic disorder than in the comparison group in this study. A neuropathic disorder is one cause of ulcer recurrence (Li et al., 2019). Another reason may be that patients with DM are complex and need interdisciplinary management that includes DM nurse educators, psychologists, pharmacists, nutritionists, podiatrists, and endocrinologists to reduce ulcer recurrence (Mcgill et al., 2017).
In this study, patients with risks such as overpressure distribution on the plantar did not use therapeutic footwear, which is one of the measures that decreases the incidence of ulcer recurrence (Zhang et al., 2022).
Prevention efforts to reduce ulcer recurrence in diabetic patients remain a priority for healthcare providers in Indonesia, and there are already specialized clinics and polyclinics for diabetic feet. This is important because the incidence of ulcer recurrence in diabetic patients varies from 25% to 80% (Lavery et al., 2007), and thus, better prevention strategies and models are still needed (Bus & van Netten, 2016).
Practical Implications
This study developed a model for preventing ulcer recurrence in patients with DM through a content validity study. The implementation of the model can provide an evidence base for efficacy in reducing ulcer recurrence rates. The recurrence prevention model can be applied in a clinical setting, but with the condition that prior training is given to manage ulcer recurrence prevention in diabetic patients.
Strengths and Limitations
Since the prevention model developed in this study reduced the incidence of ulcer recurrence in patients with DM, it was concluded that the scientific evidence for its efficacy was satisfactory. However, studies with randomized controlled trials with an interdisciplinary team approach are needed to study the impact of the preventive model on reducing the incidence of ulcer recurrence in diabetic patients.
Conclusion
In Indonesia, there is still little evidence to support the use of multiple intervention models for the prevention of foot ulcer recurrence. The recurrence prevention model developed in this study showed that the prevention of recurring foot ulcers through inspection, foot care, and blood glucose control was effective. More high-quality controlled studies are needed in this area, particularly with regard to the prevention of diabetic foot ulcers, to better inform healthcare professionals about effective preventive treatment.
Footnotes
Acknowledgements
We express our gratitude and appreciation to the Minister of Research, Technology and Higher Education (Menristek-Dikti) who supported and staff participated in this study.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received financial support from the Minister of Research, Technology and Higher Education (Menristek-Dikti) with no. B/87/E3/RA.00/2020.
Ethical Statement
This study was approved by the Ethics Committee Board of the Institute of Nursing of Muhammadiyah Pontianak no. ((no.99//KEP/II).I/AU/D/2021).
Informed consent/Patient consent
Informed consent was obtained from all individual participants included in the study.