
Abstract
Background
Diabetic foot ulcers (DFUs) impose a substantial burden on healthcare systems worldwide, leading to a diminished health-related quality of life (HRQoL) characterised by reduced productivity and limited mobility.
Objectives
The aim of this cross-sectional and longitudinal study was to compare the HRQoL in patients with both healed and non-healed ulcers over 12 months.
Methods
We recruited a prospective cohort of 257 patients from the Diabetic Foot in Primary and Tertiary (DEFINITE) Care program. We assessed their HRQoL using the EuroQol Five- Dimensional Questionnaire (EQ5D) and Diabetic Foot Ulcer Scale-Short Form (DFS-SF) at baseline and at 3-month intervals. Additionally, we collected patients’ health states according to a nine-state Markov model.
Results
At baseline, the mean EQ5D utility value was 0.736 ± 0.240. For DFS-SF, mean scores were as follows: Leisure 73.8 ± 34.0, Physical health 84.6 ± 19.1, Dependence/daily life 89.5 ± 20.3, Negative emotions and Worry 81.0 ± 21.1, Bothered by ulcer care 85.4 ± 19.5, and Total 82.5 ± 16.9. As ulcers healed, there was a significant improvement in the EQ5D utility value, increasing from 0.807 ± 0.194 to 0.903 ± 0.171 (p < .001). Similar improvements were observed across most DFS-SF domains, apart from the ‘bothered by ulcer care’ domain.
Conclusions
Within a multi-ethnic population in Singapore, patients with DFU experienced a diminished HRQoL at baseline. Expectedly, as ulcers healed over the 12-month period, there was a notable improvement in HRQoL. These findings highlight the substantial impact of DFUs on patients’ lives and underscore the importance of timely wound management in improving HRQoL.
Introduction
Diabetes mellitus (DM) contributes a significant clinical and economic burden to healthcare systems globally, resulting in a corresponding rise in diabetes-related complications such as diabetic foot ulcers (DFUs). 1 Literature suggests that approximately 18.6 million patients with diabetes develop DFUs each year; the lifetime risk has been reported to be around 34%.2,3 Ulceration portends a poor prognosis, with DFUs preceding almost 85% of all amputations performed for diabetic patients. 4 The risk of mortality amongst patients with DFU is also substantially higher than that of the general population - the 5-year mortality rate is an estimated 40%, and there is a reduced life expectancy of 14 years. 5
In Singapore, more than 700,000 patients were affected by diabetes mellitus in 2021 6 and this number is expected to surpass one million by 2050 if left unchecked. 7 Approximately 1036 lower limb amputations are performed annually as a consequence of DFU, costing an estimated SGD$14,845 per minor amputation and SGD$42,730 per major amputation in public healthcare institutions. 8 This, along with prolonged and multiple hospital stays, has meant that DFU treatment costs approximately SGD$4776 per ulcer. 9 Taking into account the strong evidence for a multidisciplinary team (MDT) approach to DFU management, the Diabetic Foot in Primary and Tertiary (DEFINITE) Care, an inter-institutional and multi-disciplinary health systems innovation programme, was established in June 2020. 10 Results were encouraging: compared to a retrospective cohort from 2013 to 2017, both 1-year minor and major amputation rates were significantly lower, and there was an improvement in glycaemic and lipid control. 10 Apart from tangible outcomes, there are also significant impacts of DFU on patient’s quality of life which are not quantifiable by these measures, including poor productivity, loss of mobility as well as associated feelings of anxiety and depression. Hence, it is essential to evaluate patient reported outcome measures (PROMs) to deliver patient-centric care.
Various instruments - such as the generic EuroQol five-dimensional questionnaire (EQ5D) and Research and Development 36-item Form (RAND-36), as well as the specific Diabetic Foot Ulcer Scale (DFS), NeuroQoL and Carrington foot questionnaire - have been found to be equally appropriate in determining PROMs. 11 Of note, a systematic review of the literature reported that the DFS was the most validated PROM amongst patients with DFU, with the DFS Short Form (DFS-SF) demonstrating similar robustness yet greater utility in clinical practice. 12 More generic PROMs, such as the EQ5D, are also useful in identifying changes in health- related quality of life (HRQoL). 13 A combination of both disease-specific and generic PROMs has been deemed to be the most useful in providing information on HRQoL outcomes. 12
In this study, we aim to analyse the HRQoL of a multi-ethnic cohort of patients with DFUs in Singapore over a 12-month period measured using the EQ5D and DFS-SF.
Methods
Study subjects
We performed a cross-sectional and longitudinal study on a prospective cohort of patients within DEFINITE Care: patients that presented with DFU to primary care polyclinics, multidisciplinary Lower Extremity Amputation Prevention Programme (LEAPP) clinics or DFU-related inpatient wards were recruited, with their Lower Extremity Amputation (LEA) and survival rates monitored over a period of time. Patients with DFUs – defined as patients with DM and with tissue loss (anatomically at or distal to the malleolus), ulcer, gangrene, abscess, osteomyelitis or cellulitis with or without neuro-arthropathy – were randomly sampled.
Exclusion criteria included patients with DM but with ulcers proximal to the malleolus (mixed arterio-venous aetiology), patients with callus only, patients with cellulitis only, patients with peripheral arterial disease without tissue loss and patients who have pre-diabetes.
Baseline patient demographic data was collected, including age, ethnicity, comorbidities and the number of DFU-related procedures performed.
Health-related quality of life measurements
HRQoL was measured using EQ5D and DFS-SF. EQ5D and DFS-SF questionnaires (Supplementary Appendix 1 and 2) were administered primarily in English (or translated to the patient’s mother tongue if required) by trained diabetic foot coordinators over phone, on recruitment (first presentation of DFU) and subsequently at 3, 6, 9 and 12 months. The recruiters and administrators of the questionnaires were different from those directly providing care to the patients.
EQ5D is a generic measure of HRQoL and has five domains: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. 11 Each domain has five response options, including no problems, slight problems, moderate problems, severe problems and extreme problems. The scores obtained were attached to an EQ5D profile according to a set of weights based on data from the United States, with values anchored at 0 (a state as bad as being dead) and 1 (full health). A sixth question (EQ6) assessed perceived health on a scale of 0 to 100, where 100 represents the best health they can imagine and thus a better HRQoL.
The DFS-SF is a disease-specific instrument that measures specific factors impacting patients’ lives as a result of their DFU. 14 The following six conceptual domains are evaluated: leisure, physical health, dependence/daily life, negative emotions, worried about ulcers/feet and bothered by ulcer care. Each item has five response options from 1 to 5. All DFS scales are then scored from 0 to 100 after reverse-coding the responses, with higher scores indicating a better HRQoL. The scores are added up to give a total score ranging from 29 to 145.
Health states
Patients’ health states were also collected according to the nine-state Markov model (Figure 1) for diabetic foot disease.
15
Health states were determined from case note reviews by diabetic foot coordinators. A nine-state Markov model for diabetic foot disease.
Patients with healed ulcers were defined as those who transitioned from health states 1/3/5/7 at baseline to 2/4/6 within the 12-month period assessed, while patients who transitioned from health states 1/3/5/7 at baseline to health states 1/3/5/7/8 were deemed to have non-healing ulcers.
Statistical methods
Continuous variables are presented using mean and standard deviation or median and interquartile ranges depending on the distribution of the parameters. After the normality of the data was evaluated using the Shapiro-Wilk test, non-parametric tests such as the Mann- Whitney U test were carried out to compare HRQoL between healed and non-healed ulcers. The significance level was pre-determined at p < .05 for all tests. All statistical analyses were performed using Microsoft Excel 2016 and SPSS Version 29.
This study had been approved by the institution ethics review board (National Healthcare Group Domain Specific Review Board 2021/01154).
Results
Baseline characteristics of participants.


Study flowchart.
Analysis of HRQoL at baseline using EQ5D
EQ5D utility values and EQ5D domain of perceived health in patients with diabetic foot ulcer.

Abbreviations: SD, standard deviation; IR, interquartile range. P values in bold are statistically significant (p < 0.05).
Analysis of HRQoL over time using EQ5D
The EQ5D utility value of patients with DFU is depicted in Table 2 and Figure 3(a)–(b). There was a statistically significant improvement in utility value between baseline and month 3 (p < .001), baseline and month 6 (p = .008), baseline and month 9 (p < .001) and baseline and month 12 (p < .001). (a) EQ5D utility value and (b) EQ6 (perceived health) over time.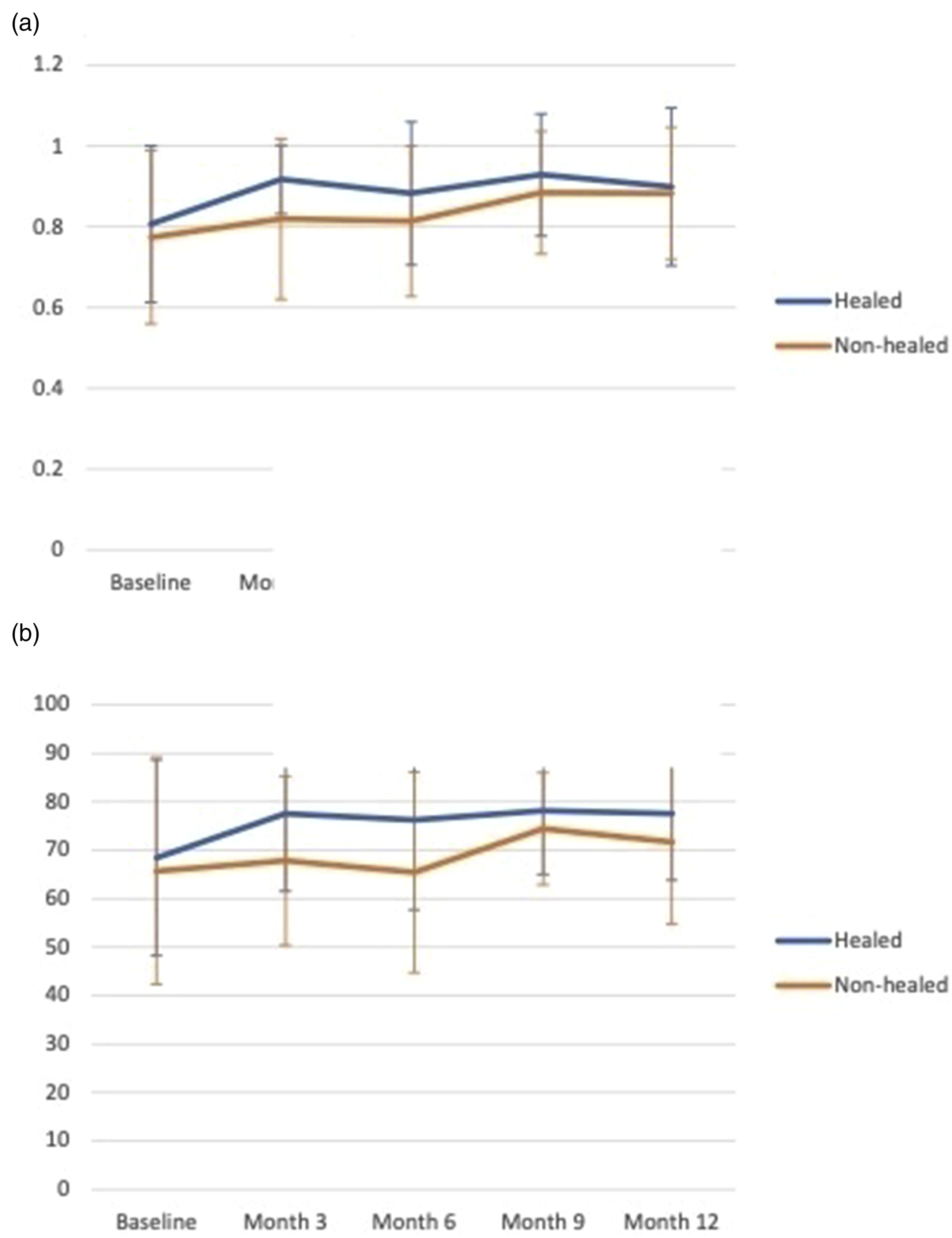
There were also significant improvements in patients’ perception of their health between baseline and month 3 (p = .012), baseline and month 9 (p < .001) and baseline and month 12 (p = .004) as shown in Table 2.
Analysis of HRQoL at baseline using DFS-SF
DFS-SF domains of HRQoL in patients with DFU over 12 months.

Abbreviations: SD, standard deviation. P values in bold are statistically significant (p < 0.05).
Analysis of HRQoL over time using DFS-SF
DFS-SF domains of HRQoL in patients with DFUs over time is shown in Table 3 and Figure 4(a)–(f). For the leisure domain in DFS-SF, HRQoL displayed a statistically significant improvement between baseline and month 3 (p = .007), baseline and month 6 (p = .003), baseline and month 9 (p = .002) and baseline and month 12 (p = .003) (Supplementary Figure 3). Regarding physical health, all 3-month intervals assessed demonstrated statistically significant improvement in HRQoL - between baseline and month 3 (p < .001), month 6 (p < .001), month 9 (p < .001) and month 12 (p < .001) (Supplementary Figure 4). The domain of dependence/daily life also reflects statistically significant improvement in HRQoL between baseline and month 3 (p = .018), baseline and month 6 (p = .018), baseline and month 9 (p = .028) and baseline and month 12 (p = .002) (Supplementary Figure 5). Statistically significant improvements in HRQoL were noted for the domain of negative emotions between baseline and month 6 (p = .033), baseline and month 9 (p < .001) and baseline and month 12 (p < .001) (Supplementary Figure 6). Unlike for the previous domains, no statistically significant change in HRQoL from baseline to month 3, 6, 9 or 12 was found for the domain of being bothered by ulcer care (Supplementary Figure 7). When comparing the total score across all domains, there were statistically significant improvements in HRQoL between baseline and month 3 (p = .002), baseline and month 6 (p < .001), baseline and month 9 (p < .001) and baseline and month 12 (p < .001) (Supplementary Figure 8). DFS-SF score for (a) leisure, (b) physical health, (c) dependence/daily life, (d) negative emotions & worry, (e) bothered by ulcer care and (f) total score over time.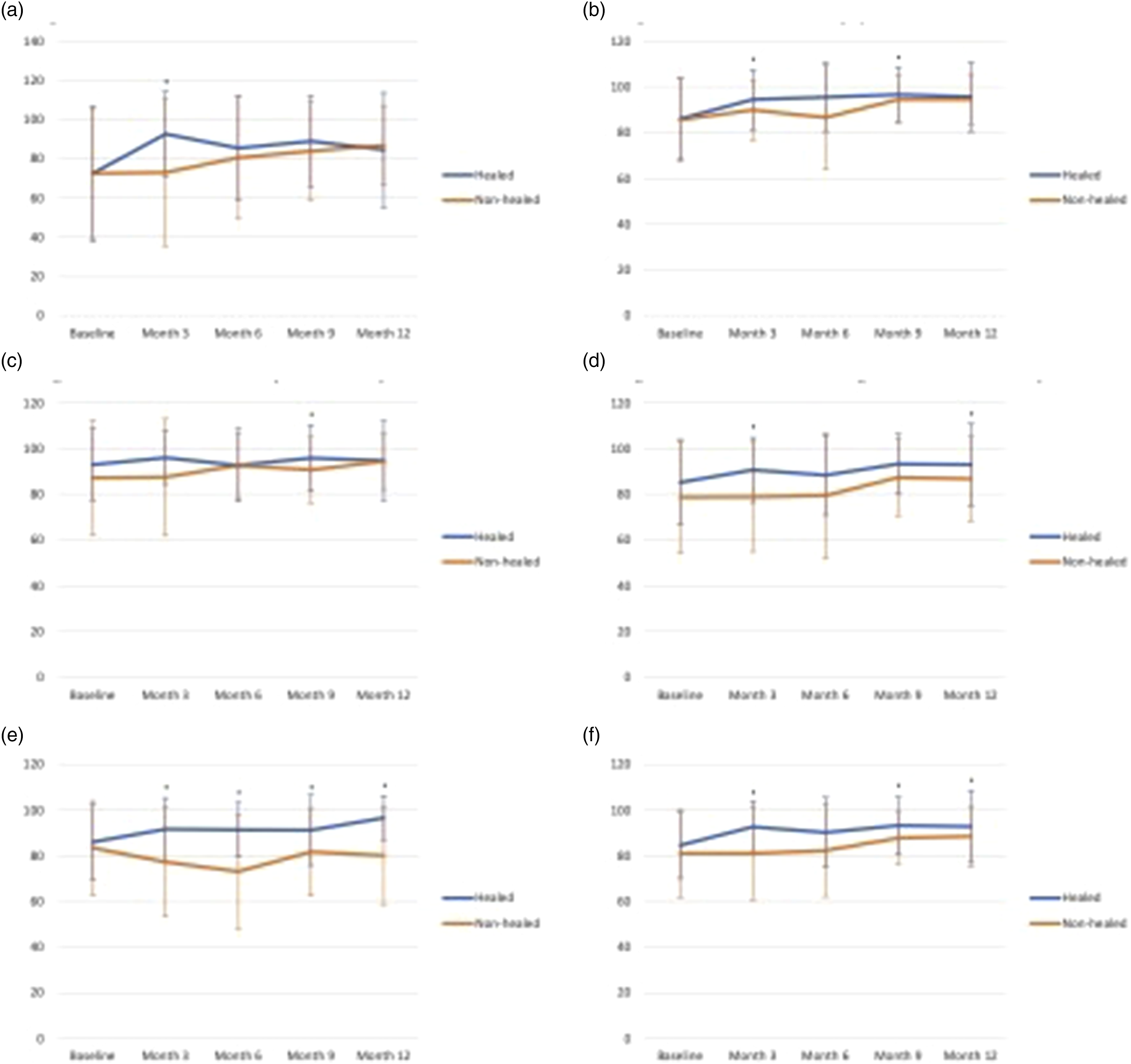
HRQoL of healed and non-healed ulcers
At the end of 12 months, a total of 49 healed patients and 56 non-healed patients completed the EQ5D and DFS-SF questionnaires; over this time frame, three patients had recurrent ulcers in month 3, while two and four patients had recurrent ulcers in months 6 and 12 respectively. Patients without any recorded health states – due to incomplete information in the case notes reviewed – were not included in the analysis.
With reference to Table 2, for patients with healed ulcers, the EQ5D utility value increased significantly from 0.807 at baseline to 0.903 when the ulcer was healed (p < .001). For patients with non-healing ulcers, the utility value also increased non-significantly from 0.770 at baseline to 0.831 (p = .101). Comparing healed and non-healing ulcers, the utility value was significantly higher for healed ulcers compared to non-healed ulcers (p = .015).
Patients’ perceived health (Table 2) also demonstrated a significant improvement from baseline to when the ulcer healed (p = .017). For non-healing ulcers, there was no significant difference in patients’ perceived health (p = .309). Similarly, patients with healed ulcers were noted to have a significantly higher perceived health compared to patients with non-healing ulcers (p = .015).
With regards to DFS-SF, for patients with ulcers that eventually healed during the 12-month period, it was observed that there was a statistically significant improvement in HRQoL from baseline for all domains (Table 3). Conversely, patients with ulcers that did not heal during the same time frame only demonstrated significant improvement for the domain of physical health (p = .028). HRQoL of healed ulcers were also statistically greater than that of non-healed ulcers in all domains.
Discussion
EQ5D and DFS-SF scores across various studies (mean ± standard deviation).

Abbreviations: EQ5D, EuroQol five-dimensional questionnaire; DFS-SF, diabetic foot ulcer scale-short form.
Over the 12-month study period, DFU patients within DEFINITE Care experienced an improvement in HRQoL across almost all domains assessed, suggesting that patients learn to accommodate their healed or non-healed DFUs when performing activities of daily living. 29 Interestingly, from month 9 to month 12, there was a slight decrease in HRQoL for EQ5D and most domains of DFS-SF. In contrast, there were no significant changes in HRQoL for the domain of being bothered by ulcer care. As all patients - regardless of whether their ulcer healed were included in the temporal analysis, the significant increase in HRQoL for healed ulcers could have been balanced by the decrease in HRQoL for non-healed ulcers.
Regarding ulcer healing, healed ulcers demonstrated improvements in all domains and had better HRQoL scores as compared to ulcers that did not heal during the 12 months assessed. Other studies have reported equivalent findings: in a cohort of 294 patients, healing of DFUs resulted in a marked improvement in SF-36 while HRQoL declined amongst non-healed ulcers. 30 Less reliance on off-loading devices, decrease in pain sensation and reduced need for wound management may be some of the reasons why healed ulcers are associated with higher HRQoL.31,32
A major limitation of this study was the loss to follow-up, with the number of patients remaining at 12 months being less than at baseline. This could have contributed to lower-than- expected HRQoL scores as the study progressed: patients whose ulcers had already healed may not have scheduled another appointment, resulting in relatively more patients with non-healing ulcers at month 12. Although demographic data were collected, the lack of integration or mapping of these variables to DFS-SF or PROM scores significantly hindered the ability to perform rigorous analyses to mitigate this bias, as most analytical methods rely on such mapping for accurate interpretation and adjustment. In addition, HRQoL measurements may exhibit floor and ceiling effects wherein patients’ baseline HRQoL measurements may be too high or too low, resulting in changes over time that go undetected. 33 Response shifts may also have occurred in which an individual’s opinions, values and expectations change over time, rendering it difficult to compare HRQoL measurements at different time points. 34
In conclusion, our study revealed significant insights into the health-related quality of life (HRQoL) of patients with diabetic foot ulcers (DFUs). We observed that patients experienced a diminished HRQoL at baseline, as indicated by lower EQ5D utility values and various domains of the DFS-SF. However, as ulcers healed over the 12-month period, there was a notable improvement in HRQoL, as evidenced by increased EQ5D utility values and improvements in most DFS-SF domains. As compared to international literature, patients with DFU in Singapore have a better HRQoL at first presentation. These findings highlight the substantial impact of DFUs on patients’ lives and underscore the importance of timely and effective wound management in improving HRQoL. Overall, our research contributes to the growing body of knowledge on the assessment and management of DFUs, with potential implications for healthcare strategies aimed at enhancing the well-being of individuals affected by this condition. Future studies could include data stratifying our findings by the number of comorbidities, complications or level of care received. Presence of any adverse outcomes (such as amputations) for patients that reported non-healed ulcers should also be explored.
Supplemental Material
Supplemental Material - Health-related quality of life of patients with diabetic foot ulcers in Singapore: A cross-sectional and longitudinal analysis
Supplemental Material for Health-related quality of life of patients with diabetic foot ulcers in Singapore: A cross-sectional and longitudinal analysis by Betty Jia Wen Lam, Petrina Yew Faye Lee, Huiling Liew, Enming Yong, Malcolm Mak, Tiffany Chew, Elaine Tan, Donna Tan, Yi Bing Loh, Xiaoli Zhu, Jeremy Hoe, Claris Shi, Dexter Yak Seng Chan, Chelsea Law, Gary Ang, Lixia Ge, Hui Yan Koo, Kai Qiang Low, Julia Choo, Cin Yee Tan, Jaime Lin, Jo Ann Lim, Shaun WY Chan, Sadhana Chandraskear and Zhiwen Joseph Lo in Proceedings of Singapore Healthcare
Footnotes
Acknowledgments
Not applicable.
Author contributions
All authors were involved in conceptualisation of the research aims, data collection and development of methodology. BJWL and PYFL performed a formal analysis of the study data and wrote the original draft. The final manuscript was reviewed, edited and approved by all authors.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Skin Research Institute of Singapore, Agency for Science, Technology and Research (A*STAR) under its Industry Alignment Fund – Pre-Positioning Programme (IAF-PP) grant number H17/01/a0/0Y9 as part of Wound Care Innovation for the Tropics (WCIT) Programme, National Healthcare Group Population Health Grant PHG20/S/X/1/1 and NMRC Research Training Fellowship FLWSHP19nov-0015.
Availability of data and materials
The datasets generated and/or analysed during the current study are available from the corresponding author.
Ethical approval
Ethical approval for this study was obtained from the institution ethics review board (National Healthcare Group Domain Specific Review Board 2021/01154).
Consent to participate
Written informed consent to participate was obtained from all participants.
Consent for publication
Not applicable.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial Registration
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.