
Abstract
Background
A woman can have fewer children when intervals between consecutive births are optimal. This has great importance for the well-being of women, pregnancy outcomes, and the long-term health of children under the age of five. We can save 2millon of the 11 million deaths of children under the age of five per year by avoiding short birth intervals. It is affected by the knowledge and attitude of women, particularly rural women, who had a high fertility rate. To our deep review, this is the first study done in Ethiopia. Hence, this study aimed to assess knowledge and attitude towards short birth intervals and associated factors among rural women who gave birth in the last three years at Dembecha district, northwest Ethiopia.
Method
A community-based cross-sectional study was conducted from September 20 to October 20, 2019. A cluster sampling technique was employed to select the study participants and data were collected using a pre-tested, semi-structured, interviewer-administered questionnaire. Bivariable and multivariable logistic regression model was fitted to identify factors associated with knowledge and attitude towards short birth interval. The level of significant association was declared using the adjusted odds ratio (AOR) with 95% confidence interval (CI) and a p-value of <0.05.
Result
From the total study participants, 66.4% (95% CI: 63.0–70.0) had good knowledge and 45.9% (95% CI: 42.3–49.8) had a positive attitude towards short birth intervals. In multivariable logistic regression: marital status, antenatal care follow-up, maternal occupation, and wealth status were significantly associated with knowledge. In addition, antenatal care follow-up and maternal occupation were significantly associated with attitude.
Conclusion
Majority of the participants had poor knowledge and a positive attitude towards short birth intervals. Hence, interventions should be done to optimize women's knowledge and attitude towards short birth intervals by enhancing antenatal care utilization.
Introduction
Birth interval is defined as the time interval between two consecutive live births (USAID, 2020). Birth interval between two consecutive live births less than 33months is called short birth interval (World Health Organization [WHO], 2005). Studies showed that birth intervals should be spaced for three to five years to make sure maximum health benefits for mothers and newborns (Ejigu et al., 2019; Yadav, 2018). World health organization (WHO) recommends that attempting another pregnancy at least two years apart after a live birth is important (Begna et al., 2013; Powell, 2014; Van Soest & Saha, 2018). In addition, according to Ethiopian national family planning guidance, spacing childbirth at intervals of three to five years is recommended to reduce adverse feto-maternal and neonatal complications (Federal Ministry of Health [FMOH], 2019).
Short birth interval is mostly familiar among mothers in low-income countries (Pimentel et al., 2020). According to the population reports from 55 countries, 26% of women gave birth within 2 years of their previous birth, and 31% were born within 2–3 years of their previous birth (Perin & Action, 2015). More than half of Ethiopia's pregnancies occur within three years of their previous births (Ethiopian Demographic and Health Survey [EDHS], 2016).
Having a short birth interval is an important public health concern, as it comes with a host of adverse effects on mothers and their children (Thapaliya et al., 2015). The majority of neonatal and maternal deaths occurred in sub-Saharan Africa and South Asia, which comprised 3.1 million neonatal deaths and 287, 000 maternal deaths (Thapaliya et al., 2015; WHO, UNICEF, UNFPA, 2019).Ethiopian mini Demographic and Health Survey (EDHS) showed that there is still a high (59%) under-five mortality rate and 33% neonatal death (Mini EDHS, 2019). Moreover, there are 412 maternal deaths per 100,000 live births women (EDHS, 2016).
Scholars revealed that maternal mortality and adverse pregnancy outcomes increase with short birth intervals (Barclay & Kolk, 2018; Biradar et al., 2019; Kozuki et al., 2013; Yang et al., 2019). These adverse outcomes are obstetrical and neonatal, some of the obstetrical complications are uterine rupture, premature rupture of membranes, anemia (Kozuki et al., 2013), gestational diabetes, precipitate labor (Pimentel et al., 2020), and the most common neonatal adverse effects are small for gestational age, preterm delivery, low birth weight (Dadi, 2015; Kozuki et al., 2013), abortion, stillbirth, wasting and congenital anomaly (Gebrehiwot et al., 2019; Shahjada et al., 2014)
Studies showed that when the length of the birth interval is increased to two years or more, infant mortality is reduced by 50% and fertility is reduced by 43% (Biradar et al., 2019). Furthermore, the likelihood of developing toxemia and anemia, as well as the risk of third trimester bleeding, is decreased by 2.5 times, as compared with birth intervals less than 24 months (Perin & Action, 2015). Along with the health implications, a short birth interval increases population growth, lowers the productivity of women, and forces families to invest more resources in child care (Cherie & Mebratu, 2017; Tsegaye et al., 2017).
Study conducted in Dessie city, Ethiopia showed that women who have good knowledge about optimal birth interval could reduce short birth interval by 55% (Hailemeskel et al., 2020). Another study showed that positive attitude of women towards short birth interval increase its magnitude and complications (Dehne, 2015). Scholars also revealed that knowledge gap among women and socio-cultural and demographic variations within countries affect birth interval practice (Nti et al., 2014; Yadav, 2018; Yang et al., 2019). Moreover, maternal education and rural residence were factors affecting mothers’ knowledge level (Yadav, 2018).
As short birth intervals can be modified, it is imperative and essential to understand women's knowledge and attitudes to improve maternal and neonatal health through specific interventions (Class & Rickert, 2018). Therefore, assessing the knowledge and attitude of rural women towards short birth interval and its associated factors will help to develop and implement different means of promoting childbirth intervals and to curb the adverse effects of maternal and child health. This also supports the national recommendations of optimal birth spacing and reduction of high fertility rate which is the current agenda of Ethiopian government (Ayele, 2015; EDHS, 2016). Moreover, it is reasonable to suppose these rural women because they had not easily accessed to health care facility and media. To the best of our knowledge, there is no prior study conducted on knowledge and attitude of rural women towards short birth interval in Ethiopia. Hence, the current study focused on knowledge and attitude towards short birth interval and associated factors among rural women who gave birth in the last three years at Dembecha district, northwest Ethiopia.
Methods and Materials
Study Area and Design
A community-based cross-sectional study was conducted from September 20 to October 20, 2019, in the rural part of Dembecha district. Dembecha district is located 350 km away from Addis Ababa, the capital city of Ethiopia, and 215 km away from Bahir Dar, the capital city of Amhara regional state. It has 35 kebeles (31 rural and 4 urban). According to the Dembecha District health office report, the total population in the District is 151,023 where 75,464 were females. Regarding health infrastructures, there are seven health centers and 34 health posts that serve the community in the district.
Populations
All women of reproductive age who experienced at least two successive deliveries and the last deliveries were within the last three years before the data collection were the source population. The research participants were all women of reproductive age who experienced at least two successive deliveries and the last deliveries were within the last three years in the selected kebeles during the study period.
Eligibility Criteria
All women of reproductive age who experienced at least two successive deliveries and the last deliveries were within the last three years in the selected kebeles during the study period and reside for 6months in the study area. women who had a history of abortion between the last two consecutive live births and seriously ill were excluded from the study.
Sample Size Determination and Sampling Technique
The sample size was determined using single population proportion formula with the following assumptions: The proportion of knowledge, attitude, and associated factors among mothers was taken-50% since no previous study was done on the source population at 95% level of confidence, and a 5% margin of error. After using design effect 1.5 (since cluster sampling) and by considering none response rate of 10%, the final sample size was 634.
In Dembecha district, there are 31rural kebeles, from which 25% of the total kebeles (eight kebeles) were selected by the lottery method. A house-to-house visit was carried out in the selected kebeles (clusters) to find eligible women for the study. All eligible participants in the selected kebeles were included in the study, making the sample size 695. Of the total eligible women, 6 participants have failed to complete the questionnaire and 5 participants have refused to participate in the study, the response rate of the study was 98.4% and the final sample size was 684.
Variables of the Study
Maternal knowledge and attitude towards short birth interval were the outcome variables whereas age, religion, marital status, maternal education, maternal occupation, husband education, husband occupation, wealth index quantile, parity, number of alive children, age at first marriage, antenatal care (ANC) follow up, number of ANC follow up, place of delivery, gained birth interval information during ANC, planned last-child, who decide birth interval, want other child and time interval for other child were independent variables.
Operational Definitions
Data Collection Tool and Procedure
The data collection tool for the assessment of knowledge and attitude towards short birth interval was adapted from different published articles (Albin et al., 2013; Hailu & Gulte, 2016; Nti et al., 2014; WHO, 2005; Yadav, 2018; Yohannes et al., 2011). The questionnaire includes socio-demographic characteristics, obstetric characteristics. knowledge items (8questions) and attitude items (17 questions) of rural women. The questionnaire used to assess knowledge was answered on true/false or I don’t know options. Each response was scored as “0” for the incorrect or I don’t know the response, and “1” for the correct response. The attitude is also measured by the Likert scale and each Likert scale has different scoring methods, which range 1–5 based on the question type either negative or positive. For negative questions, the Likert scale scoring was, 1 = strongly agree, 2 = agree, 3 = no idea, 4 = disagree, 5 = strongly disagree, and for the positive questions scoring system, the vise verse of negative questions applied. Individual knowledge and attitude scores were added together to get a total knowledge and attitude score, respectively. To classify participants as having good knowledge, those study participants who scored at least 60% of the knowledge questions and study participants who scored less than the mean were considered as having a positive attitude towards short birth interval.
The data were collected using a pre-tested, semi-structured interviewer-administered questioner. The questioner was prepared first in English and translated to the local language (Amharic) with the assistance of language experts to make it simple and understandable. Eight BSc midwives were involved in the data collection while two MSc midwives supervised the data collection process. Data collectors and supervisors were trained for half-day about the techniques of data collection and supervision. First, data collection instruments were pretested on 5% of the sample from the non-selected study kebeles, and corrections were taken accordingly. Throughout the course of the data collection, regular meetings were held among the data collectors, supervisors, and the principal investigator. The collected data were reviewed and checked for completeness before data entry and the incomplete data were discarded.
Data Processing and Analysis
Data were coded and entered into Epi info version 7.1.5.2 and exported to Statistical Package of Social Science (SPSS) version 20 for analysis. Descriptive analysis such as mean and standard deviation was used to summarize numerical data and categorical variables were summarized in frequency, percentage, figures, and tables. The bivariable and multivariable logistic regression model was fitted to identify factors associated with good knowledge and positive attitude towards short birth interval. Variables with a P-value of less than 0.2 in the bivariable analysis were included in the multivariable logistic regression to adjust for possible confounders. Both crude and adjusted odds ratio were used to measure the strength of association between independent and dependent variables. Finally, a p-value <0.05 with a 95% confidence interval for the adjusted odds ratio was used to determine the level of significance.
Results
Socio-Demographic Characteristics of Study Participants
Out of 695 study participants, 684 were involved in this study and the response rate was 98.4%. Nearly one-third (30.6%) of study participants were found between 35–39 years age group. The mean age of study participants was 34 ± 5.5 (µ ± SD) years and almost all (99.1%) study participants had followed orthodox Cristian in religion. Of the total study participants, six hundred sixty- two (96.8%) study participants were married and more than half of the study participants (58.3%) were unable to read and write. Also, more than three-fourths 550 (80.4%) of study participants were farmers and one hundred sixty-two (23.7%) study participants were in the lowest wealth status (Table 1).
Socio-Demographic Characteristics of Women in Dembecha District, Northwest Ethiopia, 2019 (n = 684).

Reproductive Characteristics of Study Participants
From the total study participants, four hundred thirty-three (63.3%) had given birth more than four times and more than half (59.9%) of study participants were first married at age of 15–17 years’ group. In addition, six hundred ten (89.2%) women had antenatal care (ANC) follow-up during their index child pregnancy. Of these, five hundred five (92.6%) had less than five times ANC follow up and five hundred eighty-seven (96.2%) had gained birth interval information during their ANC follow-up. Also, more than three fourth (81.1%) of study participants were decided on a birth interval by discussing with their husband and nearly half (47.2%) of study participants want to give birth after waiting 24–36 months (Table 2).
Reproductive Characteristics of Women in Dembecha Districts, North West Ethiopia, 2019 (n = 684).

Knowledge Toward Short Birth Interval and Associated Factors
Out of the total study participants, 66.4% (95% CI: 63.0–70.0) had good knowledge to ward short birth interval with a knowledge mean score of 7.65 ± 2.08 (µ ± SD). Six hundred one (87.9%) study participants had heard about short birth interval and two thirds (66.6%) of participants knew 3–5 months’ birth interval has health advantage. Besides, almost all 675 (98.7%) women want to practice optimal birth interval and majority (96.6%) of women knew methods of contraceptives that used for birth interval. Also, more than two-thirds (67.4%) of study participants mentioned that short birth interval is less than 33months (Table 3).
Knowledge Items Toward Short Birth Interval among Women who Gave Birth in the Last Three Years at Dembecha District, Northwest Ethiopia, 2019 (n = 684).

The bivariable analysis showed that marital status, husband education, ante natal care (ANC) follow up, age at first marriage, place of delivery, parity, number of children, maternal occupation and wealth status were significantly associated with the knowledge of participants at p < 0.2. In multivariable logistic regression: marital status, ANC follow-up, maternal occupation, and wealth status were significantly associated with the knowledge of participants toward short birth intervals. Accordingly, married study participants were 2.82 (AOR = 2.82; 95% CI: 1.11–7.13) times more knowledgeable compared to unmarried study participants. In addition, women who had ANC follow-up during their index child pregnancy were 4.82 (AOR = 4.82; 95% CI: 2.82–8.20) times more knowledgeable compared with those study participants who had no ANC follow-up. Moreover, study participants being housewives were 59% less likely to have good knowledge about short birth interval than study participants being a farmer (AOR = 0.41, 95% CI: 0.26–0.64). Lastly, participants having wealth status of middle, fourth and highest were 2.29 (AOR = 2.29; 95% CI: 1.36–3.85), 2.37 (AOR = 2.37;95% CI: 1.39–4.02), and 3.02 (AOR = 3.02; 95% CI: 1.76–5.19) times more knowledge compared to those participants whose wealth status was lowest, respectively (Table 4).
Sources of Information About Short Birth Interval
Health care providers were the main sources of information for about 481(70.3%) study participants followed by family and friends (16.5%) and mass media (3.5%).
Types of Contraceptives Mentioned by Study Participants Used for Birth Interval
The most common type 584 (85.4%) of contraceptives mentioned by study participants was Depo-Provera (Figure 1).

Types of contraceptives mentioned by women that used for birth interval in dembecha district, northwest Ethiopia, 2019 (n = 684).
Attitude Toward Short Birth Interval and Associated Factors
According to the current study, the prevalence of a positive attitude toward short birth interval was found to be 45.9% (95% CI: 42.3–49.8). More than two-thirds (66.2%) of study participants agree that optimal birth interval is important. Four hundred forty-nine (65.6%) women agree that having three years birth interval between the last and preceding child is the recommended one. More than one-third (33.3%) of study participants believe that husband willingness is a must to practice optimal birth interval and more than two-thirds (62.6%) of study participants disagree that having many children proves women's fertility (Table 5).
Bivariable and Multivariable Analysis of Factors Associated with Knowledge Toward Short Birth Interval among Women who Gave Birth in the Last Three Years, at Dembecha District, North West Ethiopia, 2019 (n = 684).

COR-crude odds ratio AOR-adjusted odds ratio, CI-confidence interval, 1-reference category *p < 0.05, **p < 0.001.
In bivariable analysis maternal education, husband education, maternal occupation, maternal age, ANC follow up and wealth status were found to be significantly associated with attitude toward short birth interval. Multivariable logistic regression analysis revealed that the odds of having a positive attitude towards short birth interval was 4.62 times higher among farmers than employed women (AOR = 4.62; 95% CI: 1.11–19.1). Moreover, study participants who had noANC follow-up had 2.19 (AOR = 2.19; 95% CI: 1.27–3.75) times higher positive attitude towards short birth interval than those women who had ANC follow up (Table 6).
Attitude Items Toward Short Birth Interval among Women who Gave Birth in the Last Three Years at Dembecha District, Northwest Ethiopia, 2019 (n = 684).

Discussion
Short birth intervals are associated with adverse obstetrics complications which leads to maternal and neonatal deaths (Kopp et al., 2018; Mahande & Obure, 2016)
Bivariable and Multivariable Analysis of Factors Associated with Attitudes Toward Short Birth Interval among Women who Gave Birth in the Last Three Years at Dembecha District North West Ethiopia (n = 684).
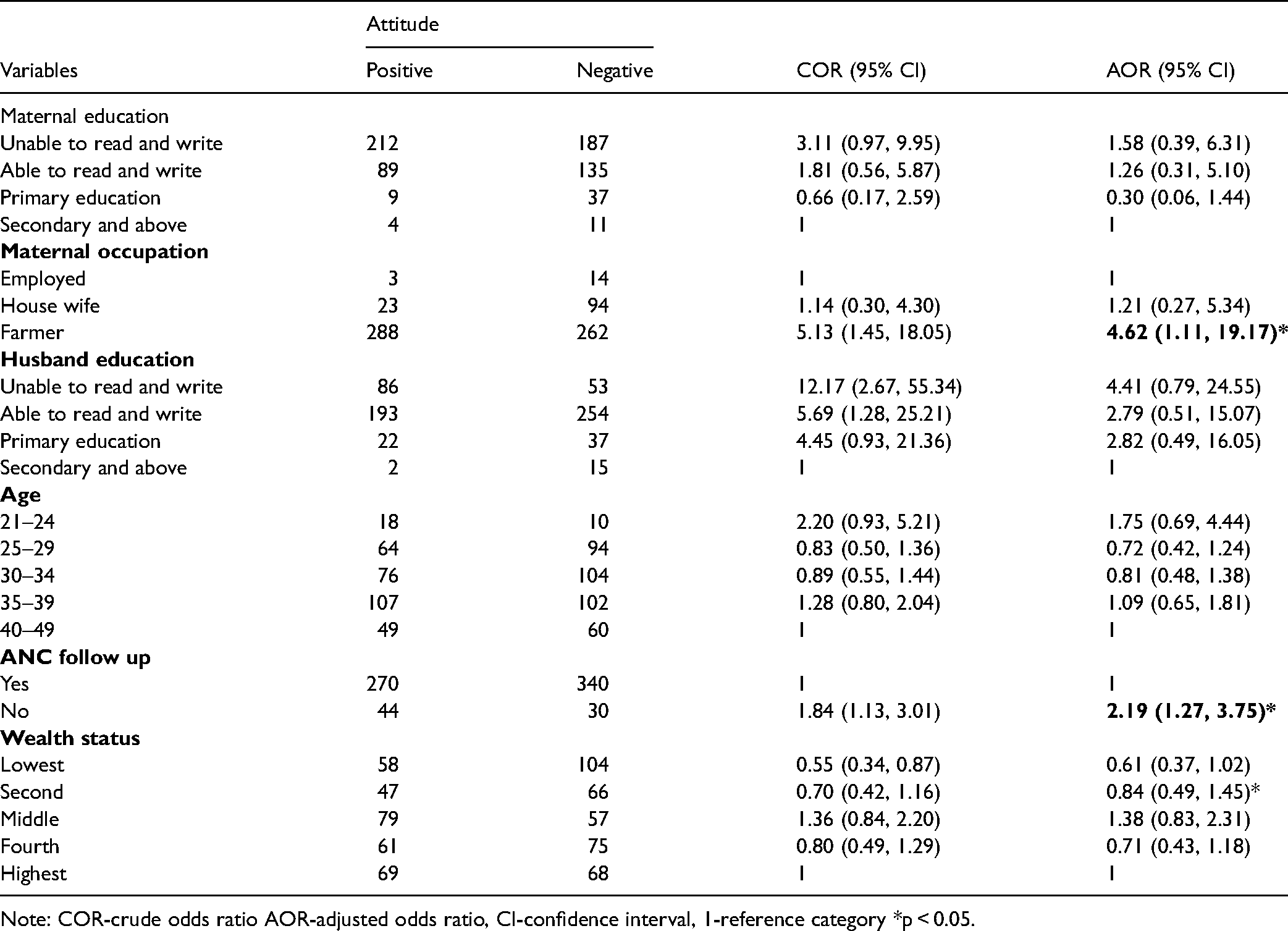
Note: COR-crude odds ratio AOR-adjusted odds ratio, CI-confidence interval, 1-reference category *p < 0.05.
Almost two-thirds of the study participants (66.4%) had a good knowledge toward short birth intervals. This finding was higher than studies done in Hosanna, Ethiopia (60%) (Yohannes et al., 2011), Gahanna (10%) (Nti et al., 2014), and Myanmar (43.9%) (Nyein et al., 2014). The discrepancies might be the differences in socio-demographic factors like occupational status, study population, and sample size. In this study, only 17.1% of women were housewives whereas 89.6% of study participants were housewives in the hosanna study. Moreover, the difference might be the variation in the time of study, and this study was conducted later after the information was disseminated through different media and health care providers. These might have brought the magnitude difference between the current study and fore mentioned studies.
This study finding was lower than the result of study conducted in India (73.8%) (Yadav, 2018). The possible reason for the difference might be socio-demographic factors such as maternal education status. In the current study, only 8.9% of participants were educated while in India 77.4% of participants had completed primary and secondary education. It is fact that educated people have deep knowledge about short birth interval and its complications. In addition, the source population of this study was all reproductive age multipara women whereas, in India, the source population was all married reproductive-age women.
Marital status was significantly associated with the knowledge of participants toward short birth interval. Married participants were 2.82 times more knowledgeable compared to unmarried study participants. This might be due to the fact that married participants could exchange information about short birth interval and its outcomes with their husbands. Furthermore, the absences of motivation, responsibility, and shared information from their partners in unmarried women may have a negative effect on the level of knowledge about short birth interval.
In addition, participants who had antenatal care follow-up during their index child pregnancy were 4.82 times more knowledgeable compared to those participants who had no antenatal care follow-up. This may be due to the fact that participants who had ANC follow-up would be more likely to receive updated and reliable information from health care providers. Access to updated information could help to avoid misinformation and increase the knowledge level of participants toward short birth intervals.
The odds of having good knowledge was 59% less likely among housewives’ women compared to farmer women. The probable reason might be farmer women may get different individuals in their working area and may share or get information about short birth interval than housewives’ women.
Moreover, the odds of good knowledge in the middle, fourth and highest group of wealth status women were 2.29, 2.37 and 3.02 times higher compared to the lowest group of wealth status women, respectively. This could be explained by the fact that socio-economically disadvantaged women may not be able to access health care utilization, health information and have little knowledge about family planning services (Shifti et al., 2020). These factors could result poor knowledge.
This study revealed that 45.9% of women had a positive attitude towards short birth interval. This finding was higher than the study in Myanmar (40.0%) (Nyein et al., 2014) and India (29.4%) (Yadav, 2018). This might be the differences in socio-economic factors like educational status. In the current study, only 2.2% of women had secondary and above education level whereas in India 46.6% of women had college educational level. Individuals who had higher education levels had different sources of information and better knowledge about the consequences of short birth interval. This might be the reason why the prevalence of positive attitudes towards short birth interval was low in India. In addition, the difference might be the difference in study setting; The current study was a community-based study whereas, the study in Myanmar was institutional. Participants who had ANC follow-up had a better understanding and information about short birth interval than their counterparts.
The maternal occupation was significantly associated with the attitude of participants towards short birth interval. Being farmer women were 4.62 times more likely to have a positive attitude towards short birth interval compared to being employed women. The possible reason might be employed individuals are mostly educated and had better knowledge about the recommended and short birth intervals than farmer women. It is fact knowledge is a key instrument to do any activity and to modify the attitude of individuals that is the reason why employed women had a negative attitude towards short birth interval than farmer women.
In addition, the odds of having a positive attitude towards short birth interval were 2.19 times higher among women who had no ANC follow-up compared to women who had ANC follow up. This might be due to the fact that ANC follow-up provides an opportunity to promote healthy behaviors and planning for optimal birth intervals through health education by health care providers. Moreover, ANC is the main modifier of attitudes, and women who had antenatal care follow-up had a negative attitude towards short birth interval (Abate et al., 2015).
Limitation of the Study
The cross-sectional nature of the study design might not possible to infer the cause and effect relationship between women's knowledge, attitude, and associated factors towards short birth interval. As knowledge and attitude of short birth interval not well studied, we didn’t find enough studies to compare and contrast our findings with others, and it makes our discussion lightly shallow. Despite these limitations, our findings provide important information about rural women's knowledge and attitude towards short birth interval.
Conclusion
Two-thirds (66.4%) of study participants had good knowledge towards short birth interval and less than half (45.9%) participants had a positive attitude towards short birth interval. In multiple logistic regression: marital status, ANC follow-up, maternal occupation, and wealth status were significantly associated with a good level of knowledge. In addition, maternal occupation and ANC follow-up were significantly associated with a positive attitude towards short birth interval. Interventions should be done to optimize women's knowledge and attitude towards short birth interval by enhancing antenatal care utilization and by intensifying programs that improve the socioeconomic status of disadvantaged women.
Footnotes
Acknowledgments
We would like to thank university of Gondar for Ethical approval. We would also like to extend our gratitude to each college administrative officials, data collectors, supper visors and study participants.
Abbreviations and Acronyms
Authors’ Contributions
MBA involved in the conception and design of the study, participated in data collection, analyzed the data, drafted the manuscript, and approved the final version of the manuscript. WZT, KTA, and TZD approved the proposal with some revisions, participated in data analysis, and revised subsequent drafts of the manuscript and approved the last version of the manuscript. All authors have read and approved the manuscript.
Ethical Approval
Ethical clearance was obtained from the school of midwifery under the delegation from the Ethical Review Board (IRB) of the University of Gondar. A formal letter of cooperation was written to each selected kebeles by the Dembecha district health bureau.
Consent to Publish
Not applicable.
Informed Consent to Participate
Written informed consent was obtained from study participants after they had been informed about the objective of the study. In the consent, statements about the potential risk, benefit, and confidentiality were included.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Competing Interests
The authors declare that they have no competing interests.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.