
Abstract
Introduction
Despite being initially perceived as a local infectious disease, COVID-19 has emerged as one of the most perilous global health threats, significantly impacting the psychological well-being of individuals worldwide.
Objective
This cross-sectional descriptive study investigates the psychological distress, fear, and coping mechanisms among Thai people residing in Thailand during the COVID-19 pandemic.
Methods
This online cross-sectional survey targeted Thai individuals during the first and third waves of the COVID-19 pandemic. Participants aged 18 and above who provided consent self-reported their responses to the Kessler Psychological Distress Scale, Fear of COVID-19 Scale, and Brief Resilient Coping Scale. Data collection occurred between November 2020 and January 2021 across four regions of Thailand. Univariate and multivariate logistic regression analyses explored associations between contextual factors and the variables of interest.
Results
Out of 498 survey respondents, with an average age of 43.07 (SD = 13.69) years, 81.9% were female, and 61.6% self-identified as healthcare workers, with 47.59% identified as frontline healthcare workers. Findings revealed that 46% of participants experienced moderate-to-very high levels of psychological distress, 14.3% reported high levels of fear of COVID-19, and 35.1% exhibited low resilient coping. Factors such as changes in employment status or financial situations, comorbidities, contact with known or suspected COVID-19 cases, recent healthcare utilization for COVID-19-related stress, and elevated fear of COVID-19 were associated with higher levels of psychological distress. Conversely, being nurses and perceived better mental health status were linked to more effective coping strategies.
Conclusion
These results emphasize the critical importance of government interventions to safeguard the psychological well-being of healthcare workers and the broader Thai population. Urgent measures to bolster resilience among these groups during and after the pandemic are imperative.
Keywords
Introduction
The severity of symptoms leading to death in infectious cases made coronavirus disease-2019 (COVID-19) one of the most dangerous diseases for people globally. Moreover, the variant kept people in fear and worried about “unknown” effects as time passed, while the consequences during and after infection also made life more difficult. Therefore, a study of the psychological impact is still needed despite the repeated occurrence of new waves of infections.
The psychological impact of COVID-19, that is, psychological distress, fear of COVID-19, and resilience in coping, has been studied and has varied based on specific local contextual factors such as health status, employment, and government support across various socioeconomic backgrounds, policies, and healthcare delivery systems. One systematic review including 107 studies across 32 countries with 398,771 participants reported the prevalence of psychological distress, depression, and anxiety at 50.0%, 28.0%, and 26.9% among the general population, respectively (Nochaiwong et al., 2021). A study of healthcare workers also reported distress, depression, and anxiety at 71.5%, 50.4%, and 44.6%, respectively; 41.5% of these workers were frontline healthcare workers (Lai et al., 2020).
It is not the infectiousness that causes people’s suffering; however, the consequences of a pandemic, which compelled people to stay home and sometimes closed the business sector, may cause them to struggle with their daily lives. A study of 78 countries found that mental health decreased while people experienced mandatory lockdowns, especially for those who had trouble with their financial situations and lacked access to basic supplies (Gloster et al., 2020). Contextual factors, therefore, contributed to people’s stress beyond the stress-related effects of infection itself.
Although people in Thailand have been vaccinated with first, second, and third doses at 85.9%, 79.8%, and 37.8%, respectively, infection and mortality rates are still high. It was reported that, on August 4, 2022, there were 34,056 new cases of infection, with the cumulative total of COVID-19-related deaths at 30,143 since the beginning of the pandemic (Workpoint News, 2022). This statistic worried Thai people about the infectiousness of COVID-19 despite the vaccination campaign and the fact that the government had called for the end of the pandemic in July 2022. The self-reported mental status of Thais during COVID-19 via the mental health check-in application of the Mental Health Department, Ministry of Public Health, indicated that 7.16% self-reported high stress, 8.48% were at risk of depression, 4.67% were at risk of suicide, and 4.23% were at risk of burnout (Department of Mental Health, MOPH, n.d.a).
Moreover, the suicide rate among the Thai population increased from 6.64 per 100,000 in 2019 to 7.37 per 100,000 in 2020 during the first and second waves of the COVID-19 pandemic (Department of Mental Health, MOPH, n.d.b). Therefore, how Thais respond to such a pandemic and what contextual factors are associated with their mental health condition will be important information for local governments, healthcare providers, and the Thai healthcare system in order to plan for further assistance.
Review of Literature
The COVID-19 pandemic has markedly escalated levels of psychological distress across various populations, with studies documenting its pervasiveness and intensity. A critical review by Xiong et al. (2020) notes the widespread impact of the pandemic on mental health, citing increased symptoms of anxiety, depression, and psychological distress globally. This is particularly evident in the research of Wang et al. (2020), which found that the immediate psychological responses during the initial phase of the COVID-19 outbreak included high rates of anxiety, depression, and stress among the Chinese population. Similarly, a study conducted in Italy, one of the early European epicenters of the pandemic, by Rossi et al. (2020) reported significant levels of psychological distress, particularly among healthcare workers and individuals with preexisting health conditions. These findings are echoed in a cross-sectional study by Özdin and Bayrak Özdin (2020), highlighting the severe psychological impact and higher stress levels in the Turkish population during the pandemic. Collectively, these studies underscore the urgent need for effective mental health strategies and interventions to address the growing psychological distress caused by COVID-19.
Furthermore, the pervasive fear associated with the COVID-19 pandemic has been a significant psychological phenomenon affecting individuals globally. Ahorsu et al. (2020) developed the Fear of COVID-19 Scale (FCV-19S), capturing the various dimensions of fear related to the pandemic. Their findings highlighted the extensive psychological impact of this fear on daily functioning and mental health. Concurrently, coping strategies have emerged as critical in managing this fear and the related stress. A study by Cheng et al. (2020) emphasized the role of positive coping strategies, such as seeking social support and engaging in problem-solving, in reducing the negative psychological impact of the pandemic. Bäuerle et al. (2020) explored online-based interventions as effective means for stress reduction and coping enhancement in the general population. Furthermore, frontline healthcare workers have been found to benefit from specific coping strategies, like mindfulness and resilience training, as shown in research by Pollock et al. (2020). These studies collectively suggest that understanding and fostering effective coping mechanisms are vital for mitigating the fear and psychological distress caused by the COVID-19 pandemic.
The concept of resilience coping has gained significant attention in the context of the COVID-19 pandemic, especially among frontline healthcare workers and the general population. A pivotal study by Labrague and De Los Santos (2020) emphasizes the resilience of healthcare workers during the pandemic, highlighting coping mechanisms that mitigate stress and burnout. This resilience is not limited to healthcare professionals; research by Polizzi et al. (2020) explores resilience strategies in the general population, emphasizing the importance of adaptive coping skills in maintaining mental health during the pandemic. Similarly, a study by Killgore et al. (2020) underscores the role of social support and adaptive coping strategies in fostering resilience among American adults. In the context of frontline workers, Walton et al. (2020) identified specific resilience-building strategies, including peer support and psychological first aid, as crucial for managing the extraordinary stressors faced by this group. These studies collectively underscore the importance of resilience and coping strategies in navigating the unprecedented challenges posed by the COVID-19 pandemic.
Contextual factors, which serve as either buffers or stressors, impact how people deal with the COVID-19 pandemic. A study of the psychological impact of the COVID-19 pandemic across 17 countries found that 69% of people experienced psychological distress at moderate-to-very high levels. Gender, employment status, and comorbidity with mental health were highly associated with psychological distress and fear of COVID-19 (Rahman et al., 2021). This study also revealed that the careers of healthcare workers, such as doctors, reported higher psychological distress among healthcare providers but less fear of COVID-19. In contrast, nurses reported being more resilient in coping with its consequences. Financial issues are an inevitable stressor associated with higher psychological distress, such as fear, anxiety, depression (Rahman et al., 2021), insomnia, frustration, and anger (Brooks et al., 2020). Based on Lazarus and Folkman’s (1984) stress appraisal model, individuals will utilize their personal resources, such as coping ability and social support, to anticipate a stressful event, which, in this circumstance, was the COVID-19 pandemic and the related situation impacts, such as a mandatory lockdown. Contextual conditions, including personal and social support resources, are vital in individuals’ interaction with the anticipated situation (Lazarus & Folkman, 1984). If one's coping ability and other external support resources are enough to control a stressful life event, one will be more adaptive and experience less distress. The studies on specific contextual factors, that is, personal context related to psychological distress, fear of COVID-19, and coping ability of individuals in each country, will help to tailor specific interventions for their actual needs and problems. Therefore, this study aimed to explore the psychological distress, fear of COVID-19, and resilience coping of Thai people living in Thailand and facing the COVID-19 pandemic during the first to third waves.
Methods
Design
As a component of a larger international collaborative research endeavor investigating the psychological distress experienced by healthcare workers and individuals across 17 countries, as detailed in Rahman et al. (2021), this study focuses on participants residing in Thailand. Data were gathered from Thai residents within Thailand between November 2020 and January 2021 using a cross-sectional online survey method deemed appropriate for the lockdown context. The survey covered geographical regions, including the North, Northeast, Central, and South of Thailand.
Research Questions
What are the psychological distress, fear of COVID-19, and coping strategies among Thai people living in Thailand during the COVID-19 pandemic?
What are the contextual factors influenced by those three variables?
Sample
The sample size was calculated using OpenEpi. The study population and estimated prevalence of stress varied across participating countries (17 countries). Therefore, keeping the population size at 100,000,000, assuming 50% prevalence of stress globally, 95% confidence intervals (CIs), and 80% power, the estimated minimum sample size was 385 for each country. Therefore, the sample size for this study was required to be at least 385. Snowball sampling was used to select the study participants. All Thai participants, at least 18 years old and willing to participate in the study, were included.
Inclusion Criteria
All Thai residents who were at least 18 years old and consented to participate in this study were eligible for this study.
Institute Review Board Approval
Ethics approval was obtained from the research ethics committees of the PI's institute, with the approval number 125/2020. Each participant read the consent form provided with a plain language summary and ticked their consent on the online form before they entered to answer the questionnaire with anonymity. The privacy and confidentiality of the collected data were maintained.
Data Collection
An online link was created using a structured survey questionnaire via Google Forms. The plain language information statement (PLIS) and the consent form appeared on the first screen. Only the participants who provided consent and agreed to participate in the study could move to the next screen, which contained a single eligibility criterion requiring them to be at least 18. The subsequent screens contained the full study questionnaire. All the responses were anonymous. The bilingual experts translated the English version of the PLIS, the consent form, and the study questionnaire into Thai using the back-translation procedure to ensure meaning equivalence. An invitation with the online survey link and a quick response (QR) code was shared on social media platforms, online community networks, and by email. Text messages using SMS and the Line application were also shared. In addition, flyers containing the QR codes were distributed and posted in university/healthcare settings. Any questionnaires which were completed in less than 1 min were excluded.
Study Tools
The structured survey questionnaire was adopted from a previous study conducted in Australia (Rahman et al., 2020). Psychological distress was measured using the 10 items of the Kessler Psychological Distress Scale (K-10) (Furukawa et al., 2003), fear was measured using the FCV-19S (Ahorsu et al., 2022), which has seven items, and coping was measured using the Brief Resilient Coping Scale (BRCS) (Sinclair & Wallston, 2004) which has four items. For this study, psychological distress (based on the K-10 scoring) was categorized into low (score 10–15) and moderate-to-very high (score 16–50); fear of COVID-19 (based on the FCV-19S scoring) was categorized into low (score 7–21) and high (score 22–35); and coping (based on the BRCS scoring) was categorized into low (score 4–13) and medium-to-high (score 14–20). The reliability of those tools in the English version was examined in the Australian study and was 0.92, 0.87, and 0.66, respectively. Moreover, it was found that these tools work indifferently for migrants and nonmigrants (Rahman et al., 2021). All instruments were back-translated into Thai by two bilingual experts to ensure meaning equivalence and were pilot-tested with 30 Thai participants for reliability testing. The Cronbach's alpha coefficients of the instruments were 0.91, 0.86, and 0.78, respectively.
Statistical Analyses
The database was downloaded from the Google platform, and Stata statistical software Stata/SE V.15.0 for Windows (StataCorp, College Station, USA, 2017) was used for data analyses. Descriptive statistics, including frequencies and percentages, were generated for categorical variables; mean and standard deviation (SD) were generated for continuous variables. Participants who took <1 min to complete the questionnaire were excluded from the analyses.
Univariate and multivariate logistic regression analyses examined the association between contextual factors and each of the three variables. The results are presented with odds ratios (ORs) and 95% CIs. In addition, multivariate analyses were conducted by adjusting age, gender, living status, education, and employment status. Finally, adjusted ORs (AORs) with 95% CIs were reported.
Results
Sample Characteristics
A total of 498 people who met the inclusion criteria and completed the survey were included in the study. The mean age (±SD) of the participants was 43.07 (±13.69) years, and the majority (81.9%) were females. Most lived with their family members (76.1%) and had completed a bachelor’s degree or higher (88.0%). In total, 81.5% had jobs adversely affected by COVID-19, with 34.1% reporting a moderate to a great deal of perceived distress due to a change in employment status. More than half (61.6%) self-identified as healthcare workers, while most were nurses (52.2%). About two-thirds of the participants (59.6%) reported that COVID-19 had impacted their financial situation. The majority (90%) had never been smokers, and 23.6% reported drinking alcohol in the 4 weeks prior to data collection. However, 38.1% had a history of comorbidities such as cardiac disease, stroke, hypertension, diabetes, cancer, hyperlipidemia, or chronic respiratory illness. Most (66.9%) participants did not know whether they had been exposed to COVID-19, with 33.4% of participants still visiting healthcare providers in person (Table 1).
Characteristics of the Sample.

Cardiac disease/stroke/hypertension/diabetes/cancer/hyperlipidemia/chronic respiratory illness.
Research Question Results
Psychological Distress, Fear of COVID-19, and Resilient Coping
Nearly half of the study participants (n = 229; 46%) experienced moderate-to-very high levels of psychological distress, 14.3% (n = 71) had high levels of fear of COVID-19, and 323 (64.9%) exhibited moderate-to-high resilient coping (Table 2).
Level of Psychological Distress (K-10), Fear of COVID-19 (FCV-19S), and Resilient Coping (BRCS) (n = 498).

Factors Associated with Psychological Distress
It was found that jobs affected by COVID-19 (having an income source), moderate-to-high perceived distress due to change of employment status, COVID-19-impacted financial status and change in financial status, having other physical comorbidities, direct contact with known/suspected case of COVID-19, self-identification as a patient and visiting a healthcare provider within 6 months, use of healthcare service to overcome COVID-19-related stress in the last 6 months, and high levels of fear of COVID-19 were associated with moderate-to-very high levels of psychological distress while being older (60+ years) and having a better perception of the status of one's own mental health were associated with lower psychological distress (Table 3).
Associated Factors for High Psychological Distress among the Study Population (Based on the K-10 Score).
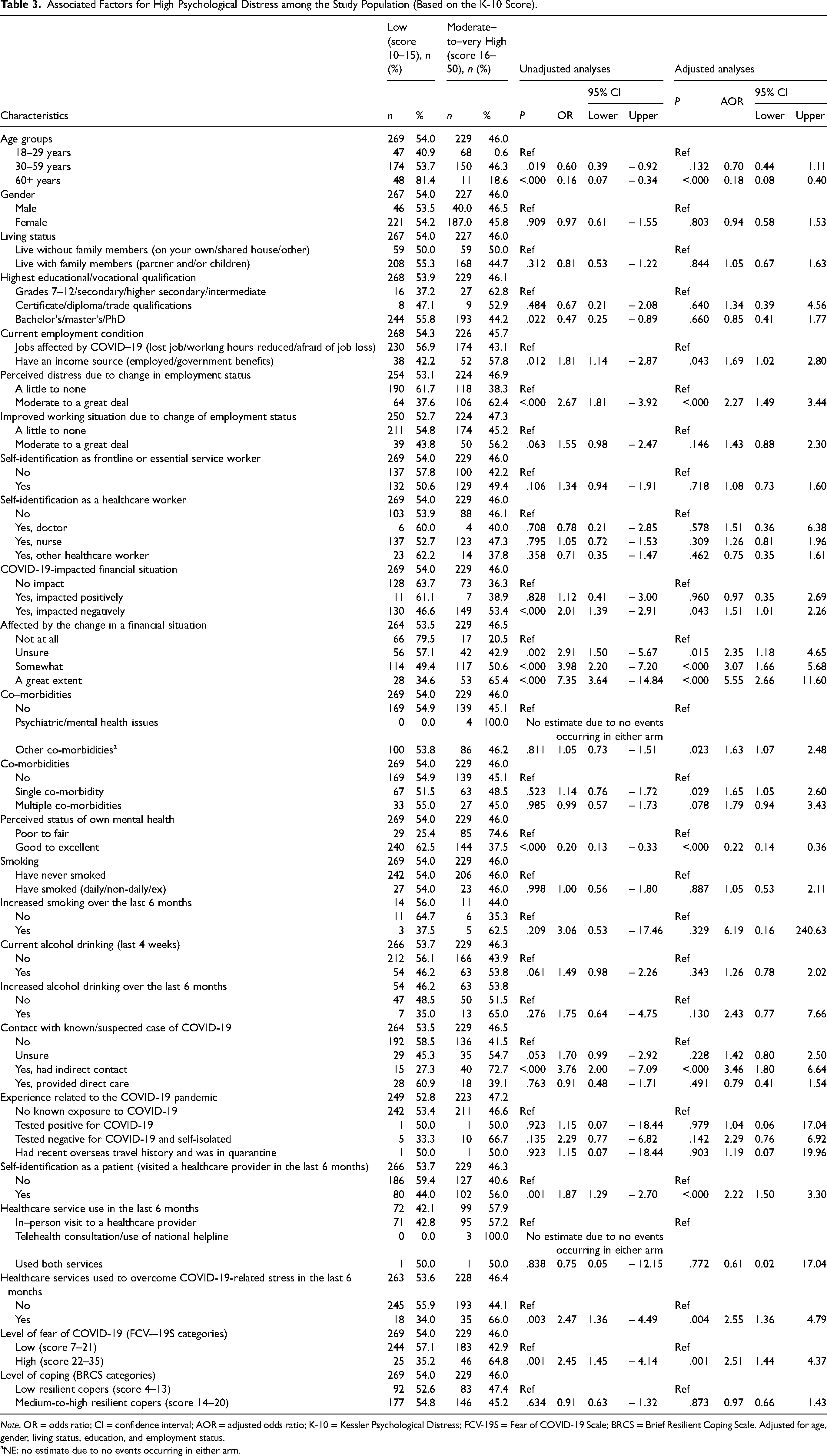
Note. OR = odds ratio; CI = confidence interval; AOR = adjusted odds ratio; K-10 = Kessler Psychological Distress; FCV-19S = Fear of COVID-19 Scale; BRCS = Brief Resilient Coping Scale. Adjusted for age, gender, living status, education, and employment status.
NE: no estimate due to no events occurring in either arm.
Factors Associated with Fear of COVID-19
Table 4 shows that jobs affected by COVID-19 (having an income source), moderate-to-high perceived distress due to change in employment status, moderate to a great deal of improvement in working situation due to change in employment status, COVID-19-impacted financial situation (both positive and negative), affected by the change in financial situation, single comorbidity, healthcare service used to overcome COVID-19-related stress in the last 6 months, and moderate-to-highly perceived psychological distress were associated with high levels of fear of COVID-19 while a better-perceived status of one's own mental health and medium-to-highly resilient copers were associated with lower levels of fear of COVID-19 (Table 4).
Associated Factors for Fear of COVID-19 among the Study Population (Based on the FCV-19S Score).

Note. OR = odds ratio; CI = confidence interval; AOR = adjusted odds ratio; K-10 = Kessler Psychological Distress; FCV-19S = Fear of COVID-19 Scale; BRCS = Brief Resilient Coping Scale. Adjusted for age, gender, living status, education, and employment status.
NE: no estimate due to no events occurring in either arm.
Factors Associated with Resilient Coping
Table 5 shows that living with family members, jobs affected by COVID-19 (having an income source), moderate-to-high perceived distress due to change in employment status, and a high level of fear of COVID-19 were associated with less resilient coping. However, when adjusting the confounders, having an income source and employment status were not statistically significant. On the other hand, being a nurse and having a better-perceived status of one's own mental health resulted in better resilient coping (Table 5).
Associated Factors for Coping among the Study Population (Based on the BRCS Score).

Note. OR = odds ratio; CI = confidence interval; AOR = adjusted odds ratio; K-10 = Kessler Psychological Distress; FCV-19S = Fear of COVID-19 Scale; BRCS = Brief Resilient Coping Scale. Adjusted for age, gender, living status, education, employment status.
NE: no estimate due to no events occurring in either arm.
Discussion
This study was one of the first studies to explore psychological distress, fear of COVID-19, and resilient coping among Thai people who lived in Thailand during the pandemic of COVID-19 (first to third waves). The present study revealed that 46% of study participants experienced moderate-to-very high levels of psychological distress, 14.3% had high levels of fear of COVID-19, while resilient coping was moderate-to-high at 64.7%.
These results align with other studies that reported psychological distress, including stress, anxiety, and depression in people around the globe, such as in China (Qiu et al., 2020), Malaysia (Bahar Moni et al., 2021), Australia (Rahman et al., 2021), Italy (Mazza et al., 2020; Moccia et al., 2020), the UK (Smith et al., 2020), Columbia (Pedrozo-Pupo et al., 2020), Japan (Ueda et al., 2020), and the USA (Liu et al., 2020) although the measurement tools were different. When considering similar tools to measure psychological distress, this study found that Thai participants experienced the lowest levels of psychological distress when compared to other countries who participated in this collaborative study, especially compared with 10 countries where it was reported at a high level, that is, Hong Kong, Oman, Libya, Kuwait, Saudi Arabia, UAE, Jordan, Syria, Palestine, and Egypt (Rahman et al., 2021). When compared to other studies using similar measurements, it was also found that participants in this study reported less psychological distress when compared with those in Malaysia (Bahar Moni et al., 2021) (46% and 62.1%, respectively) and lower fear of COVID-19 (14.3% and 27.1%, respectively). Interestingly, results were very similar for resilience coping (64.9% and 65.1%, respectively). However, the present study did not find that gender was associated with psychological distress, although there were more female participants, similar to the Malaysian study. This was also different from other studies, which found that being female was more likely to result in higher psychological distress (Qiu et al., 2020; Rahman, Hoque et al., 2020; Rahman, Islam et al., 2021).
Interestingly, participants in this study with an income source were more likely to have higher psychological distress, more fear of COVID-19, and less resilience coping. However, this could be because the pandemic could threaten their security, making them feel more vulnerable. The financial hardship and fear of COVID-19 were also found in another qualitative study in Thailand during an early pandemic. The sociocultural way of coping, such as turning to religion, practicing acceptance, being kind, being generous, and sharing, was the coping that Thais employed to ease their stressful life event (Naemiratch et al., 2022).
Notably, nurses in Thailand demonstrated remarkable resilience despite the intense workload and stress of the pandemic. The healthcare workers were over half of this study sample, accounting for 61.6%. Among this, with 260 nurses responding to the survey, accounting for 52.2% of the sample, the robustness of the findings is evident. This high participation rate is attributed to effective communication channels facilitated by connections with nurse educators, universities, and hospitals. Their participation in the survey likely served as a platform to voice their burdensome workload and stress. Nurses served as the majority of frontline workers during the pandemic. A systematic review conducted by Alnajjad et al. (2022) and a scoping review by Allobaney et al. (2020) emphasize nurses’ pivotal role in addressing the challenges of the COVID-19 pandemic. Alnajjad specifically highlights that nurses represent the majority of frontline workers.
Additionally, Wahyuningsih et al. (2020) underscore the multitude of challenges experienced by nurses, such as fatigue, discomfort, anxiety, and stress, emphasizing the necessity for resilience and professionalism in caring for COVID-19 patients. These findings resonate with a study conducted in Nepal, which revealed elevated stress levels among nurses amid the pandemic (Neupane et al., 2020). Moreover, US nurses experienced considerable stress, particularly concerning workplace issues, as evidenced by research conducted by Arnetz et al. (2020). Collectively, these findings suggest that although nurses in Thailand may have exhibited better coping mechanisms, the pandemic's global impact has significantly affected nurses’ mental well-being worldwide.
Interestingly, living with family members resulted in a higher fear of COVID-19. This might be because people worry about either getting infected or transmitting the virus to their loved ones, and ironically, this living condition is also associated with less coping. Therefore, living with family members may not serve as a support resource in this circumstance. Another Thai study found that healthcare workers employed problem-focused coping and positive attitudes to deal with stress during the COVID-19 pandemic. Marital status and having children were also found to be associated with their choice of coping strategies (Yubonpunt et al., 2022), while personal characteristics were found to have a direct effect on the psychological well-being of frontline workers in Thailand (Wuttiphan, 2022). Resilience is an important personal resource for all Thais, including older people (Soonthornchaiya, 2020).
The factors associated with a high level of psychological distress and a very high level of fear of COVID-19 were job status and financial situation, which were also associated with a low level of coping. Although the Thai government established a project for financial aid during the pandemic to promote traveling and support daily expenses for the general population, this should be tailored to specific conditions, such as for those who have financial problems or received the impact of COVID-19 on their business. Based on this study, the people who perceived moderate to a great deal of stress from changing their employment and financial status were the most vulnerable group.
Lastly, people with comorbidities were also more likely to have higher psychological distress and higher fear of COVID-19. This is especially true when, nowadays, people who die when infected by COVID-19 or after getting the vaccine are mostly people who have another comorbid condition. Therefore, enhancing the resilience coping for people who have noncommunicable diseases and integrating care between mental and physical diseases should be considered as another care model during this pandemic.
Strengths and Limitations
This study stands out as one of the pioneering investigations into the psychological distress, fear of COVID-19, and coping mechanisms among Thai individuals during the first to third waves of the COVID-19 pandemic. It sheds light on the contextual factors influencing these variables. Specifically, it highlights the contextual elements linked to heightened psychological stress and fear of COVID-19, as well as reduced coping abilities.
However, the study’s utilization of an online survey method implies its main reach was individuals possessing internet-enabled devices. Also, as discussed earlier, healthcare workers are overrepresented, accounting for 61.6% of this study sample. Consequently, there is a potential for underrepresentation among Thai populations in general, especially those in remote areas or lacking internet access, particularly those undergoing quarantine in government facilities due to COVID-19 infection. This limitation could hinder the applicability of the findings to the broader population. Furthermore, carrying out a cross-sectional study during a pandemic introduces challenges related to contextual factors, demanding careful interpretation of any identified correlations.
Implication for Practice
Resilience, the buffer against psychological distress, is worth developing for all healthcare providers to serve as an important personal resource to cope with work stress, especially during a pandemic. Mental health practitioners across the country need to promote this coping for all Thai people, especially for those who have physical comorbidity and those who have had financial and work changes impacted by the COVID-19 pandemic.
Conclusions
This study found that employment, financial status, and comorbidity were associated with higher psychological distress. On the other hand, the perceived status of one’s own mental health as excellent and resilience coping can serve as a buffer against psychological distress and fear of COVID-19. Therefore, in addition to financial aid projects, interventions/projects/efforts to improve Thai people's mental health resilience should be initiated and promoted.
Footnotes
Acknowledgments
The authors thank Dr. Patompong Khaw-on, Faculty of Nursing, Chiang Mai University, for his expertise consultation in statistical analysis.
Authors’ Contributions
MAR conceived the study. PB performed the statistical analyses and drafted the manuscript. PB, SI, SN, RT, CS, and MAR contributed to the planning, data collection, preparation, and critical review of the manuscript. All authors read and approved the final manuscript.
Consent to Participate
Each participant read the consent form provided with a plain language summary and ticked their consent on the online form before they entered to answer the questionnaire with anonymity.
Consent for Publication
All the responses were anonymous.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Thanks to the Faculty of Nursing, Chiang Mai University, for grant support.
Ethical Considerations
The Research Ethics Committees at the Faculty of Nursing, Chiang Mai University, approved our research project (approval: 125/2020) from December 7, 2020 to December 6, 2021.