
Abstract
Introduction
Nurses play pivotal roles in various facets of managing the COVID-19 epidemic, encompassing tasks such as identifying potential cases with infections, managing suspected patients, conducting patient assessments, and providing critical care to individuals afflicted with COVID-19.
Objective
The objective of this study was to assess the level of COVID-19 fear among nurses who care for infected or suspected COVID-19 patients in pandemic hospitals.
Methods
A cross-sectional study was conducted on 260 nurses employed at COVID-19 hospitals in Palestine. The Fear of COVID-19 Scale (FCV-19S) was employed to measure participants’ fear levels. The scale's potential values range from 7 to 35, with higher scores indicating a greater fear of COVID-19. Independent t-tests and ANOVA tests were utilized to evaluate differences between the variables.
Results
The analysis revealed that the mean total fear score of the nurses was 25.22 ± 5.07 (ranging from 7 to 35), indicating a high level of fear. Married nurses exhibited a fear mean score of 27.0 ± 4.9 (p < 0.05). Similarly, nurses with children scored a mean fear level of 29.0 ± 4.6 (p < 0.05). Additionally, nurses engaged in rotating shift work reported a fear mean score of 27.9 ± 4.4 (p < 0.05). Furthermore, nurses who received COVID-19 training exhibited a fear mean score of 24.6 ± 4.8 (p < 0.05). Likewise, nurses who experienced patient loss due to COVID-19 reported a fear mean score of 23.2 ± 4.5 (p < 0.05).
Conclusion
The study confirmed that nurses in Palestine exhibit a significant level of fear concerning COVID-19. Marital status, having children, working schedule, experiencing the loss of a patient due to COVID-19, and receiving training related to COVID-19 were identified as factors associated with the fear of COVID-19 among nurses.
Introduction
At the end of 2019, the spread of COVID-19, which was originally noticed in Wuhan City, China, had severe impacts on society globally (Wang et al., 2020; Zhu et al., 2020). The epidemic of COVID-19 has resulted in a considerable worldwide in the global economy. Some nations where COVID-19 was first detected gave insight on the pandemic's consequences on the healthcare professionals and healthcare system (Alfieri et al., 2020; Armocida et al., 2020; Oliva et al., 2020).
Beyond the rapid transmission of cases, the evolving understanding of COVID-19 and reports of elevated morbidity and mortality rates have instilled widespread fear and concern (Bao et al., 2020; Shigemura et al., 2020). Moreover, stress-inducing factors such as the heightened risk of infection, financial setbacks, the threat of viral spread, quarantine measures, implementation of social distancing protocols, and increased mortality rates have collectively contributed to heightened levels of fear and anxiety among the populace (Ayed & Zabn, 2021; Brooks et al., 2020; Harper et al., 2021).
Nurses, tasked with extended work hours and additional shifts to accommodate the care needs of COVID-19 patients and their families, face heightened health risks (Nie et al., 2020). Throughout the pandemic, nurses attending to COVID-19 patients have grappled with severe physical and emotional exhaustion, alongside persistent worries and fears (Aqtam et al., 2023).
Since the declaration of a state of emergency in response to the first COVID-19 cases in Palestine, the Ministry of Health (MOH) has asserted its readiness to provide comprehensive services to COVID-19 patients. Many private hospitals have proven effective in delivering care and monitoring COVID-19 patients, equipped with ventilators and staff trained to manage COVID-19 cases (MOH, 2020).
Review of Literature
Fear and worry stemming from potential illness can exact a significant and detrimental psychological toll, leading to mental health issues, weakening of the immune system, and a decreased ability of the body to fend off diseases (Belash et al., 2021). Fear and anxiety represent complex psychological and physiological states characterized by emotional, cognitive, and behavioral factors (Shen et al., 2021). Based on the context, these negative emotions may serve as motivators or cause to reluctance in adhering to protective measures. Suppressing the expression of these feelings can exacerbate their intensity or, if left unaddressed, lead to emotional strain (Ayed & Amoudi, 2020; Malinowska-Lipień et al., 2021). A study conducted among nurses caring for COVID-19 patients in Pakistan during the pandemic revealed that 92.3% of the nurses experienced moderate to severe anxiety (Alwani et al., 2020). Similarly, a study in China reported that 71.5% of healthcare personnel attending to COVID-19 patients expressed worry, while 44.6% reported feelings of anxiety (Lai et al., 2020).
Previous studies investigating fear levels among nurses during the COVID-19 pandemic have revealed a spectrum of responses, ranging from moderate to high levels of fear. A study conducted in Saudi Arabia highlighted the presence of high levels of perceived stress and fear among nurses while caring for patients afflicted with COVID-19 (Tayyib & Alsolami, 2020). Similarly, another study involving nurses working across public and private hospitals in Saudi Arabia reported moderate levels of fear regarding COVID-19 (Moussa et al., 2021). Furthermore, an Indonesian study found that a substantial portion, approximately 70.7%, of nurses expressed fear related to COVID-19 (Huda et al., 2023). Notably, nurses reported experiencing particularly heightened levels of fear in close proximity to COVID-19 patients (Moradi & Sharififar, 2023), and fear levels were notably elevated among nurses working in intensive care units (Diğin et al., 2022). These findings underscore the multifaceted nature of nurses’ responses to the challenges caused by the COVID-19 pandemic, reflecting varying degrees of apprehension and concern within different contexts of care delivery.
Nurses predominantly working in high-risk wards caring for COVID-19 patients are more susceptible to both physical and mental effects compared to those in lower risk environments. Psychological reactions such as fear can significantly influence individuals’ behaviors, leading to impaired cognitive function, heightened panic, and increased risk of burnout. Therefore, it is imperative to assess the psychological responses of healthcare professionals to the COVID-19 pandemic (Ahorsu et al., 2022; Taylor et al., 2020; Wu et al., 2020). Studies have indicated that higher levels of fear regarding COVID-19 are associated with various factors, including inadequate training about the infection, experiencing patient loss due to COVID-19, possessing more job experience, and being older (Ünver & Yeniğün, 2021). Additionally, gender and staffing shortages have been identified as contributing factors to nurses’ fear of working during the COVID-19 pandemic (Savsar & Karayurt, 2023).
Given the personalized nature of nursing care and the paramount importance of patient safety in delivering high-quality care (Mihdawi et al., 2020; Vaismoradi et al., 2020), it becomes imperative to evaluate the fear levels of nurses working in pandemic units during the COVID-19 crisis. As a result, the objective of this study was to assess the level of COVID-19 fear among nurses who care for infected or suspected COVID-19 patients in pandemic hospitals.
Methods
Design
A cross-sectional study was conducted from June to August 2020.
Research Questions
What is the fear level of COVID-19 among nurses?
What are factors related to the fear of COVID-19 among nurses?
Sample
This study was conducted at all COVID-19 hospitals across Palestine, which include Hugo Chavez Hospital in Ramallah Governorate, Red Crescent Hospital in Hebron Governorate, Military Hospital, Red Crescent Hospital in Nablus Governorate, Dora Hospital for COVID, Red Crescent in Tulkarm, Omar Al-Qasim Hospital in Qalqilya Governorate, and Turkish Friendship Hospital in the southern governorates. These hospitals have been meticulously equipped with ventilators, and the medical staff have undergone comprehensive training to handle COVID patients with the utmost proficiency and care (MOH, 2020).
The study included a convenience of nurses who are working in COVID-19 hospitals. The sample size was determined using the Raosoft program with a population of 625, a confidence level of 95%, a margin of error of 5%, and an estimated response rate of 50% (Raosoft, 2008). Initially, the calculated sample size was determined to be a minimum of 239 nurses. To account for potential attrition, the sample size was increased to 270 nurses. However, the final number of nurses who completed the questionnaires were 260 nurses
Inclusion/Exclusion Criteria
The inclusion criteria were being willing to participate in this study, working in a pandemic hospital, and handling infected or suspected COVID-19 patients. Exclusion criteria were nurses working part time.
Instruments
The questionnaire comprised three parts. The first part covered demographic characteristics (7 items) such as age, gender, educational status, marital status, having a child, working schedule, and years of experience. The second part covered experience with COVID-19 (5 items), including the status of receiving training related to COVID-19, losing patients because of COVID-19, had a relative diagnosed with COVID-19, being diagnosed with COVID-19, and having or losing a relative diagnosed with COVID-19.
The last part addressed the fear of COVID-19. The Fear of COVID-19 Scale (FCV-19S), created by Ahorsu et al. (2022), was used. This 7-item scale was rated on a 5-point Likert scale ranging from strongly disagree to strongly agree. The potential values range from 7 to 35, with a higher score suggesting a higher fear of COVID-19 (Ahorsu et al., 2022; Stahel, 2020; Satici et al., 2021). In addition, the degree of fear was characterized as low (score 7-21) or high (scoring 22-35) (Ahorsu et al., 2022; Belash et al., 2021). Previous studies found that the scale has strong predictive validity and reliability (Ahorsu et al., 2022; Gritsenko et al., 2021). In the present study, Cronbach's alpha value was found to be 0.92.
Data Collection
Because collecting data face-to-face was challenging during the epidemic, nurses were recruited for the research using a social media platform (WhatsApp) that is utilized at the hospital and contains the mobile phone numbers of all hospital nurses. The questionnaire was generated on Google Drive, and the link was sent to the target nurses via email. The questionnaire was designed so that it would not be displayed a second time once the user had filled it in, and it was protected from editing after submission. At the beginning of the survey form, each nurse electronically provided informed consent.
Ethical Considerations
The study had been approved by Arab American University. Only the researchers have access to the study forms. Participants received an electronic consent form. Participation in this study was entirely optional, and participants’ personal information was not requested.
Data Analysis
The data were analyzed using the Statistical Package for the Social Sciences (SPSS, version 23). Descriptive statistics, including frequency, percentages, means, and standard deviations, were utilized to describe the characteristics of the study variables. Furthermore, independent t-tests and ANOVA tests were employed to assess the differences between the variables.
Results
Sample Characteristics
Two hundred and sixty out of 270 nurses participated in this study, with a response rate of 96.3%. The analysis revealed that 180 (69.2%) were aged 20–29 years. The majority of the participants, 187 (71.9%), were male, and 170 (65.4%) were single. Additionally, 69 (76.6%) of the married nurses had a child. Moreover, 190 (73.1%) held a bachelor's degree, and 181 (69.6%) had less than 5 years of experience. Most of them, 238 (91.5%), worked rotating shifts, as seen in Table 1.
Description of Nurses’ Characteristics (N = 260).

The analysis revealed that 177 (68.1%) received training related to COVID-19. Additionally, 42 (16.2%) reported that they were diagnosed with COVID-19, and 109 (41.9%) reported having a relative diagnosed with COVID-19. Moreover, 16 (6.2%) reported that they lost a relative because of COVID-19, and 118 (45.4%) reported losing a patient because of COVID-19, as seen in Table 2.
Description of Nurses’ Experience of COVID-19 (N = 260).

Research Questions Results
The analysis revealed that the mean total fear score of the nurses was found to be 25.2 ± 5.1 (range 7–35), indicating a high level of fear. Furthermore, item analysis of the fear scale revealed that the highest mean scores were for “I am most afraid of coronavirus-19” and “It makes me uncomfortable to think about coronavirus” (4.1 (SD = 0.9) and 3.8 (SD = 0.87), respectively), as seen in Table 3.
Item Scores Received from the Fear of COVID-19 Scale.

An independent t-test and ANOVA test were utilized to assess the differences between mean scores of fear and participants’ characteristics. The analysis revealed statistically significant differences between fear scores and marital status, having a child, and working schedule (p < 0.05). Married nurses had a fear mean score of 27.0 ± 4.9, which was higher than that of single nurses (24.3 ± 4.9). Additionally, nurses who had a child had a fear mean score of 29.0 ± 4.6, which was higher than that of those who didn't have a child (26.4 ± 4.9). Furthermore, nurses with rotating shift work had a fear mean score of 27.9 ± 4.4, which was higher than that of nurses who worked day shifts (25.0 ± 5.1), as seen in Table 4.
Differences Between Mean Scores of Fear and Partcipants’ Characteristics (N = 260).

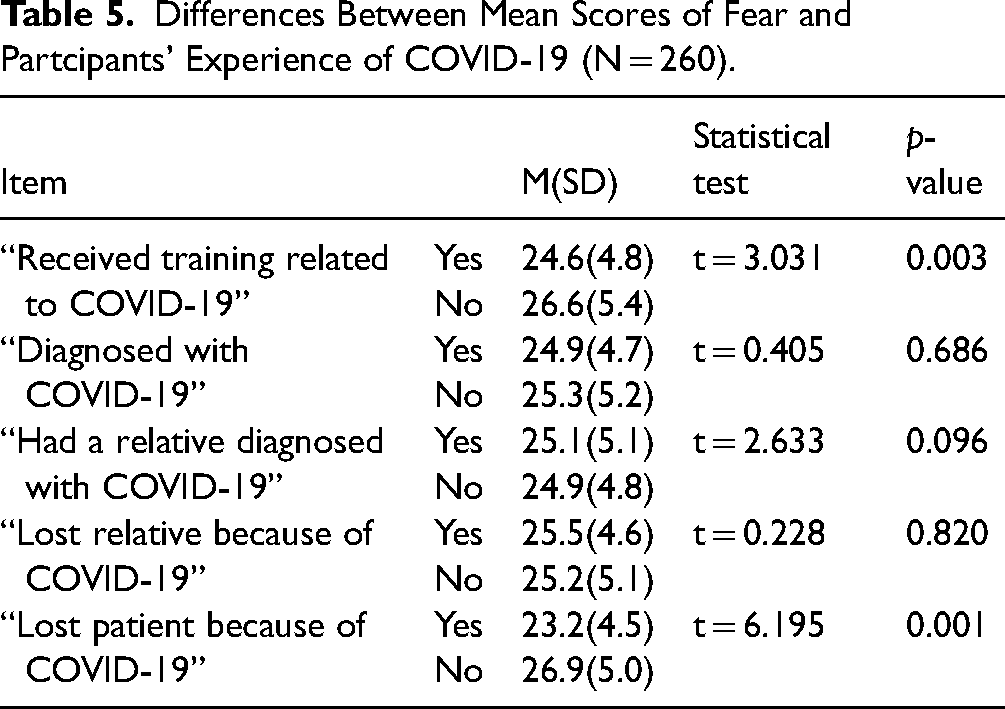
Moreover, an independent t-test was conducted to assess the differences between mean fear scores and participants’ experiences of COVID-19 as seen in Table 5. The analysis revealed statistically significant differences between fear scores and both receiving training related to COVID-19 and losing patients because of COVID-19 (p < 0.05). Nurses who received training related to COVID-19 had a fear mean score of 24.6 ± 4.8, which was lower than that of those who didn't (26.6 ± 5.4). Similarly, nurses who lost patients because of COVID-19 had a fear mean score of 23.2 ± 4.5, which was lower than that of those who didn't (26.9 ± 5.0). This could potentially be attributed to potential desensitization and a heightened sense of control gained through firsthand experience, fostering coping mechanisms and resilience.
Differences Between Mean Scores of Fear and Partcipants’ Experience of COVID-19 (N = 260).
Discussion
The current study was conducted during the peak of the COVID-19 pandemic when fear of the virus was particularly intense.
According to the findings, nurses who handle COVID-19 patients reported a strong fear of the disease. This could be explained by the challenges nurses face in new situations, fear of infection, job burnout due to long hours and protective equipment, difficulty handling patient conditions, and managing relationships in these stressful situations. However, there exists a range of perspectives in the literature regarding the severity of COVID-19-related fear among nurses (Alnazly et al., 2021; Çalışkan & Kargın, 2021; Çayır Yılmaz & Uysal, 2021; Çelik & Dağlı, 2021; Baysal et al., 2022; Hu et al., 2020; Moussa et al., 2021; Ünver & Yeniğün, 2021; Labrague & de Los Santos, 2021). Some studies, such as those by Çayır Yılmaz and Uysal (2021) and Moussa et al. (2021), have reported moderate levels of fear among nurses, findings that are consistent with the current study. Conversely, other research, including that conducted by Alnazly et al. (2021), Çalışkan and Kargın (2021), and Hu et al. (2020), have identified a higher degree of fear among nurses. Additionally, a multinational study involving nurses from Spain, Italy, Brazil, and Turkey found that nurses exhibited anxiety levels beyond the moderate range concerning COVID-19 (Baysal et al., 2022). Overall, nurses appear to be particularly vulnerable to experiencing fear, anxiety, and depression as a result of the pandemic, compared to other healthcare professionals. This heightened vulnerability has been noted in various studies across different countries, including Spain, Italy, Brazil, and Turkey (Aksoy & Koçak, 2020; Apisarnthanarak et al., 2020; Kackin et al., 2021; Saracoglu et al., 2020).
Also, the study found that nurses who received COVID-19 training had lower fear scores than those who did not. COVID-19 fear was observed to be higher among nurses who had not received COVID-19 training (Labrague & de Los Santos, 2021; Ünver & Yeniğün, 2021). Nurses’ COVID-19 fears can be reduced by having better information and knowledge to handle emergency scenarios (Mubarak et al., 2021). Cui et al. (2020) found that attending infection prevention training significantly improved nurses’ stress coping abilities, leading to a decrease in fear levels. Similarly, Labrague and de Los Santos (2021) observed that frontline nurses who received COVID-19 training exhibited lower levels of fear compared to those who did not receive such training. Moreover, the findings by Alwani et al. (2020) further support the notion that educating nurses about COVID-19 can positively impact their emotional well-being by reducing feelings of fear.
The current study highlights the significant impact of patient deaths due to COVID-19 on nurses’ fear levels. Nurses who have experienced the loss of a patient due to COVID-19 express less levels of fear compared to those who have not encountered such situations. This may indicate that nurses who have directly experienced the loss of patients due to COVID-19 may have become desensitized to the fear associated with the pandemic over time. Continuous exposure to challenging and distressing situations can lead individuals to develop coping mechanisms and resilience, thereby reducing their overall fear levels. Also, it may be that nurses who have encountered patient loss have undergone a process of psychological adjustment, wherein they have come to terms with the realities of the pandemic and accepted the associated risks and uncertainties. This acceptance may lead to a reduction in fear as they develop a more realistic perspective on the situation. However, this finding is inconsistent with previous research by Alharbi et al. (2020) and Pappa et al. (2020), which suggests that witnessing patient deaths from COVID-19 can induce fear among healthcare professionals. The fear experienced by nurses is compounded by the distressing nature of COVID-19 deaths, as noted by Galehdar et al. (2020). Furthermore, Galehdar et al. (2020) found that nurses caring for COVID-19 patients perceive these deaths as particularly painful, especially when younger patients are involved. This emotional connection with patients is further emphasized by the strong empathy that nurses develop towards those under their care, as identified by Nelson and Lee-Winn (2020). Qualitative studies, such as the one conducted by Kackin et al. (2021), shed light on the multifaceted nature of nurses’ fears. Nurses not only fear for their own health but also express distress over the potential loss of family members. Moreover, concerns about the handling of deceased patients, including the sealing of bodies, contribute to nurses’ apprehension and distress. Spoorthy et al. (2020) summarize the cumulative impact of patient deaths on nurses, highlighting how these experiences contribute to their fear and stress levels.
There were statistically significant associations between fear and marital status, having a child, and a working schedule. These findings align with previous research conducted by Fu et al. (2021), which identified married nurses with children as having higher levels of fear compared to unmarried counterparts. One plausible explanation for the elevated fear levels among married nurses with children is the concern about transmitting the infection from their workplace to their homes. As primary caregivers, these nurses may feel a heightened sense of responsibility for the health and safety of their families, thereby increasing their anxiety about potential exposure to COVID-19 in the healthcare setting. Research by Majumdar et al. (2020) indicates that working irregular shifts can lead to poor sleep quality and compromised physical and mental health. The irregularity in work schedules disrupts the body's natural circadian rhythm, contributing to fatigue, stress, and overall deterioration in well-being among nurses.
Limitations of the Study
There are certain limitations to this study that should be noted. First, consider that a cross-sectional design study cannot demonstrate causality and express views at a point in time. Also, this study was self-administered, which may have resulted in bias. Finally, only nurses with an internet connection were eligible to participate in the study. As a result, the current study suggests that more research be conducted to investigate the factors that impact pandemic fear in nurses at different times, as well as the effects of training programs on nurses’ fear levels.
Implications for Practice
It is interesting to study the fear consequences of the COVID-19 outbreak on nurses. Furthermore, psychological care and counseling for nurses is crucial in order to enhance their mental health and help them to handle the problems offered by pandemics.
Conclusion
The study confirmed that that nurses in the region experience a notable level of fear regarding COVID-19. Several factors were identified as being associated with this fear among nurses, including marital status, having children, working schedule, experiences of losing patients due to COVID-19, and receiving training related to COVID-19. To minimize mental health challenges or psychological harm, healthcare administrators should prioritize assessing the degree of fear and stress among nurses working during the COVID-19 pandemic. Also, healthcare administrators should provide training session to nurses on how to handle fear. The conclusion of our study enriches the existing literature by offering a nuanced understanding of fear during the COVID-19 pandemic. This knowledge can inform evidence-based interventions and policies aimed at effectively managing the ongoing threat posed by the virus and its associated impacts on society.
Footnotes
Acknowledgements
The authors would like to express their thanks to the nurses who participated in the study
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.