
Abstract
Objective
To describe the lived experience of nursing staff and nurse leaders working in COVID-19 devoted units (intensive care or medical unit) prior to vaccine availability.
Research Design
Qualitative phenomenological design with a focus group approach.
Methods
The study team recruited a convenience sample of nursing staff (nurses, and nursing assistants/nurse technicians) and nurse leaders (managers, assistant nurse managers, clinical nurse specialists, and nurse educators) at an academic medical center in the midwestern United States. Focus groups and individual interviews were conducted to encourage participants to describe their (1) experiences as nursing professionals, (2) coping strategies, and (3) perspectives about supportive resources. Moral distress was measured with the moral distress thermometer and qualitative data were analyzed with Giorgi-style phenomenology.
Results
We conducted 10 in-person focus groups and five one-on-one interviews (n = 44). Seven themes emerged: (1) the reality of COVID-19: we are sprinting in a marathon; (2) acute/critical care nurse leaders experience unique burdens; (3) acute/critical care staff nurses experience unique burdens; (4) meaning of our lived experience; (5) what helped us during the pandemic; (6) what hurt us during the pandemic; and (7) we are not okay. Participants reported a moderate level of moral distress (M = 5.26 SD = 2.31). They emphasized that peer support was preferred over other types of support offered by the healthcare organization. Participants expressed positive feedback about the focus group experience and commented that group processing validated their experiences and helped them “feel heard.”
Conclusion
These findings affirm the need for trauma-informed care and grief support for nurses, interventions that increase meaning in work, and efforts to enhance primary palliative communication skills. Study findings can inform efforts to tailor existing interventions and develop new, more comprehensive resources to meet the psychosocial needs of nursing staff and nurse leaders practicing during a pandemic.
Keywords
Introduction/Background
Nurses have experienced psychological trauma while caring for patients who were deteriorating and dying from COVID-19 (Leng et al., 2020; Wang et al., 2020). One of the greatest challenges for nurses caring for COVID-19 patients early in the pandemic was witnessing their extreme hypoxemic respiratory failure which was unresponsive to typical interventions (Hajjar et al., 2021; Leng et al., 2020; Wang et al., 2020). In the first two years of the pandemic, the death rate on many clinical units was double or triple pre-pandemic rates. While nurses worked diligently to provide supportive care to COVID-19 patients, they were demoralized by the high mortality rate (Galehdar et al., 2020; Joo & Liu, 2021). Clinical nursing interventions often did not improve outcomes for seriously ill COVID-19 patients (Deliktas Demirci et al., 2021; Dohrn et al., 2022).
Nurses have been physically and emotionally taxed during COVID-19 (Hall, 2020; Lai et al., 2020; Leng et al., 2020), and have experienced post-traumatic stress symptoms (Dohrn et al., 2022; Greenberg et al., 2021; Guttormson et al., 2022; Leng et al., 2020). The consequences of the high intensity workload and short staffing include overwhelming fatigue, sleep disturbances, eating problems, anxiety, acute stress disorder, and loneliness (Leng et al., 2020; Shechter et al., 2020; Wang et al., 2020). In fact, a high proportion of healthcare professionals may be struggling with their mental health, some with clinically significant symptoms of depression and anxiety (Pappa et al., 2020). In addition to extreme psychological burden, nurses also experienced other psychosocial and even physical burdens, such as social stigma and discomfort from personal protective equipment (PPE) use. The pandemic is contributing to nurses’ moral distress and burnout (American Association of Critical-Care Nurses, 2020). The consequences of unresolved moral distress and burnout include frustration, fractured team cohesion, inadequate communication and collaboration, and disengagement and attrition, exacerbating the workforce shortage (Christianson et al., 2022; McAndrew et al., 2018). Nurses who withstand the unrelenting stress and remain in practice may experience fear and dread regarding the potential for additional surges and new pandemics.
Review of Literature
Nursing literature regarding the COVID-19 pandemic has focused on the experiences and outcomes of nurses (Chegini et al., 2021; Deliktas Demirci et al., 2021; Dohrn et al., 2022; Gunawan et al., 2021; Joo & Liu, 2021; Moradi et al., 2021; Muz & Erdoğan Yüce, 2021; Sun et al., 2020); few have examined the experiences of nurse leaders. At the time of this study there was a limited body of literature on nurses’ perspectives about supportive resources provided by their organization (Shechter et al., 2020). To address these gaps, the research team conducted focus groups and individual interviews to help nursing staff and nurse leaders reflect on their practice; acknowledge their emotions; consider their relationships with patients, families, and colleagues during the pandemic prior to the availability of vaccines; and make meaning of their lived experiences. The study team responded to the Advisory Board's (Advisory Board, 2020) recommendations to create forums in which healthcare professionals can discuss their experiences and identify preferred support that fits into their day-to-day practice.
Methods
Theoretical Framework
Phenomenology was selected as the method of inquiry. The study was guided by the theory meaning reconstruction, a bereavement framework (Gillies & Neimeyer, 2006). This is a novel application of meaning reconstruction to the experiences of nursing staff and nurse leaders who may be grieving the unprecedented loss of patients, as well as the loss of their professional role as they have known it.
During times of profound stress and loss, meaning-making is a way to make sense of the world (Gillies & Neimeyer, 2006; Park, 2010), relieve distress, and promote personal growth (Breitbart, 2016; Frankl, 1946). Sharing stories of one's lived experience can initiate a process of reconstructing meaning through the elements of sense-making, benefit finding, and identity change (Gillies & Neimeyer, 2006; Rolbiecki et al., 2019) (Figure 1).

Conceptual framework.
Design
A qualitative phenomenological design with a focus-group approach was selected for this study. Quantitative data on nurses’ and nurse leaders’ self-reported levels of moral distress were also collected in order to describe aggregate levels of moral distress at the time of participation in the study. This information provided context for the qualitative data.
What was the lived experience of nursing staff (nurses, nursing assistants, and nurse leaders—managers, nurse educators, clinical nurse specialists) working in acute and critical care during the height of COVID-19 and what were their moral distress levels at the time of participation in the study? What are specific interventions and resources that nursing staff and nurse leaders believe supported their well-being during the height of the pandemic or have the potential to support their well-being? How do nurses perceive the meaning-making process used in this study (emotions, experiences, and perspectives are shared and explored in a group setting) and do they believe this process is feasible and acceptable for nurses and nurse leaders?
Setting/Sample
This study took place at a large academic medical center in midwestern United States. The study team recruited a convenience sample of nursing staff (nurses, nursing assistants, or nurse technicians), and nurse leaders (managers, assistant nurse managers, clinical nurse specialists, and nurse educators) who worked in dedicated COVID-19 units (ICU or medical unit). Data collection (January 9, 2021 to February 24, 2021) aligned with the downtrend of the hospital's first surge in COVID-19 patients.
Inclusion Criteria
Nursing staff and nurse leaders eligible to participate were: (1) at least 18 years old (2) English speakers, and (3) currently practicing in a COVID-19 devoted unit directly caring for patients or in leadership.
Ethics
This study was approved by the research site's Institutional Review Board (PRO00039329). All participants engaged in an informed consent process. Those who participated in-person signed a consent form; those who participated via phone or Zoom provided verbal consent which was audio recorded. After participation, nurses were given a handout of resources for supporting well-being offered by the organization.
Instruments
The research team collected demographic and work-related characteristics. Participants completed the moral distress thermometer (MDT) a validated instrument that has been used to measure moral distress among nurses (Wocial & Weaver, 2013). The MDT is a single-item 11-point (0 to 10) scale that describes moral distress (none to worst possible) within the past week (Wocial & Weaver, 2013). The study's conceptual model guided development of the interview guide (Figure 2). Nurses completed open-ended questions about the acceptability (satisfaction) and feasibility (how easy was it to participate) of the focus group via Qualtrics.

Interview guide for focus groups.
Trustworthiness
To ensure trustworthiness in the data collection and analysis process (Lincoln & Guba, 1985), the following actions were taken to address credibility: member checking (nurses provided feedback on results); examining data for the negative case; and study team debriefings about reactions to and interpretations of the data. To address transferability the study analysis team provided rich descriptions of the findings and included participant quotations. For dependability of the research process, members of the team that were not involved in the analytic process provided an inquiry audit. Finally, to address confirmability, the study team created a detailed audit trail of the data collection process and analytic decisions. The study team also engaged in the process of reflexivity in which the background of each researcher was considered and how it may have influenced the research process. Study team members were nurses who had practiced in various specialties, including critical care. The principal investigator (PI) leading the analytic process had not practiced as an ICU nurse during the COVID-19 pandemic.
Procedures
Study advertisements included flyers and emails, as well as hospital newsletters. Focus groups, limited to seven participants, were held after shifts in a conference room. Nurses could attend without pre-registering. If only one participant arrived for a session we conducted an individual interview to allow the participant to share their story. Nurses unable to attend an in-person focus group could participate in a one-on-one interview via Zoom or phone. Leadership teams registered in advance to participate together in the same leadership focus group.
Focus groups help researchers create a milieu in which participants can freely discuss their opinions, experiences, and insights about a phenomenon of interest (Onwuegbuzie et al., 2009). Each focus group began with broad questions and used probes to further explore ideas shared by participants (Finch et al., 2014). Focus groups were led by the PI and an additional research team member served as a co-moderator, observing non-verbal behaviors and recording field notes.
At the conclusion of the focus group discussion participants were asked to share their thoughts about their focus group experience. Nurses were later emailed a brief survey via Qualtrics to further comment on the feasibility and acceptability of this focus group experience. Participants who provided permission for the research team to contact them were invited to review and validate study findings.
Analysis
Participants’ work characteristics were analyzed with frequencies and percentages and responses on the MDT with descriptive statistics (mean and standard deviation). Giorgi's phenomenological method guided the analysis of the qualitative data (Giorgi, 1997). First the study team identified natural meaning units (close to the language of participants). Then the team regrouped and redescribed statements into focal meaning units (moving participant language into researcher language). Exemplary narratives were selected to illustrate themes and subthemes (Giorgi, 1997). The analytic process was initiated by having three research team members read the transcripts of the focus groups and interviews while concurrently listening to the audio-recording. They discussed and logged their initial reactions to the data. Each of these researchers independently coded two focus groups and then collaboratively developed an NVivo codebook. Using this codebook, the researchers independently coded three focus groups and compared their coding to ensure consistency. The research team conducted member checks with three participants to validate the analysis.
Results
Sample Characteristics
A total of 44 nurses and nurse leaders participated in the study (Table 1). The sample consisted of staff nurses (59%), nurse technicians (5%), and nurse leaders (36%) working in the medical ICU, cardiovascular ICU, and acute care units. Clinical experience ranged from six months to 20 years. The majority of participants were prepared at the baccalaureate level (80%) and more than half were 31 years of age or older (56%). The research team held a total of 10 focus groups and five one-on-one interviews ranging from 37 to 96 min (Table 2). Moral distress was moderate across all focus groups (M = 5.26, SD = 2.31).
Participant Characteristics.
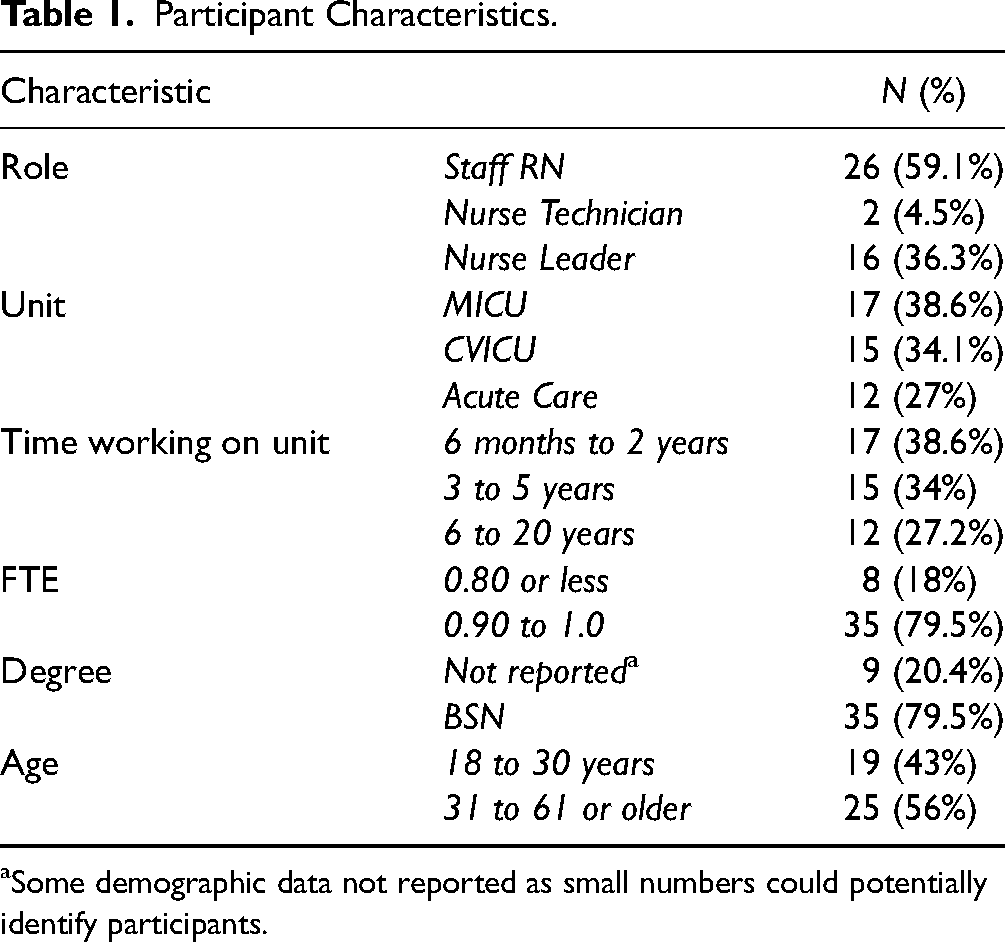
Some demographic data not reported as small numbers could potentially identify participants.
Focus Group/Interview Information and Moral Distress Levels per Moral Distress Thermometer (MDT).

Per MDT, 0 = no distress and 9 = highest distress.
Qualitative Findings
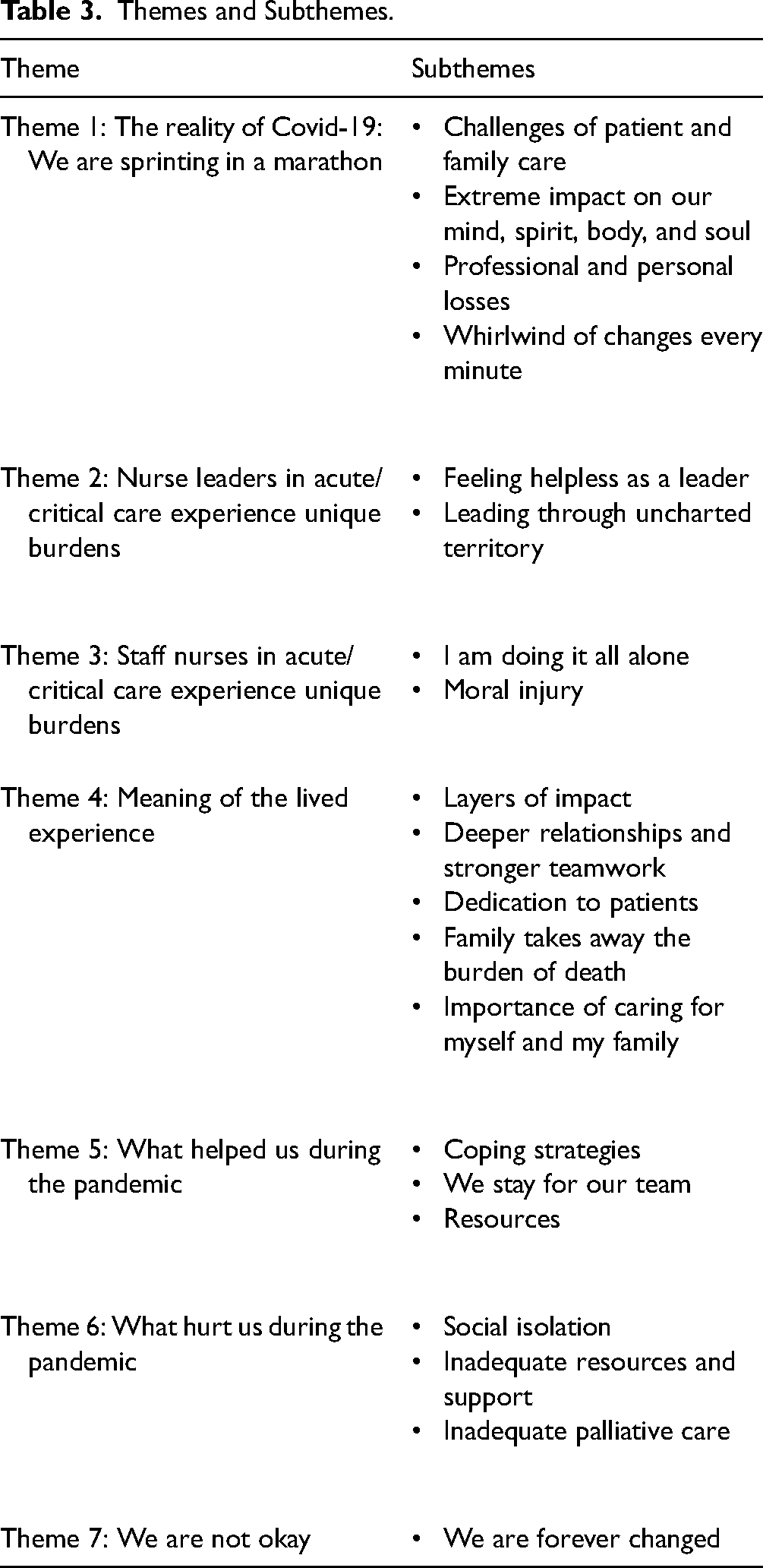
Seven themes were uncovered from analysis of the focus group/interview data (Table 3). Themes 2 and 3 illustrate differences in nurse and nurse leader experiences. All other themes represent a shared nurse and nurse leader lived experience.
Themes and Subthemes.
Theme 1: The Reality of COVID-19—We are Sprinting in a Marathon
One participant described what it was like to be a nurse during the first surge of COVID-19: “I feel like we’re sprinting in a marathon and everyone else is going at a nice pace” (Focus group 5).
Theme 2: Acute/Critical Care Nurse Leaders Experience Unique Burdens
Speaker 2: You can really tell when someone is not doing well because they just explode.
Speaker 1: You can tell they snapped. That their personality kind of shifts (Focus Group 10).
Theme 3: Staff Nurses in Acute/Critical Care Experience Unique Burdens
Nurses were advised to limit the frequency and duration of patient contact, and yet, they still had to complete necessary care and intervene when patients were in distress, thus increasing their exposure time. The required PPE was bulky and hot. “I think about…insane frustration with having to go in rooms wearing all that we wear, when a lot of these patients are very confused and pulling off their oxygen and ‘satting’ at like 60 percent. And you put it all back on again and gather yourself and put their oxygen back on and restrain them, put the mitts on, whatever you have to do. It starts all over again, and it's just exhausting” (Focus Group 6).
Nurses did not want to leave their coworkers without help, so they worked overtime even when they did not want to. Nurses wanted others to understand the difficulty of their jobs. “I just wish everyone could see a day in the life of a Covid ICU nurse and what it is like to have all these patients intubated and paralyzed and flipped up and down” (Focus Group 2).
Speaker 4: If you look at them (patients) in the bed…breathing so heavy and hard that the whole bed is shaking. 50 or 60 a minute…
Speaker 2: Their faces are purple.
Speaker 1: They’re blue.
Speaker 2: It's honestly gruesome to watch.
Speaker 4: We don’t even make eye contact with the patients because that's when you mess up. (Focus Group 8)
There were times when there were so many deaths that the units ran out of body bags. “I literally can’t do anything to help these people and I just stand there and watch them for 12 h of suffering (Focus Group 8).
Theme 4: Meaning of the Lived Experience
Nurses and nurse leaders discussed the meaning of working in their professional roles during the pandemic, and reflected on how the pandemic changed them as a person.
Speaker 1: A nurse came to me this morning because we had a patient that was expected to die. We (two nurses) both were like, “We have to go in and hold their hand quickly.” It's become a thing in the last couple of months, which I like. I went in to hold this patient's hand and another nurse came in to support me. Speaker 4: I used to work in an end of life unit prior to coming here. I think it's always felt like an honor to be someone who can be at someone's side at their worst hour and be there supporting them and their family. But I think it's taken another meaning now with Covid (Focus Group 5).
Speaker 4: We all said, do not put us on ECMO. So if I get Covid and they say I have to cannulate you, No, just withdraw (treatment).
Speaker 2: I think a lot of us have gotten POAs (Power of Attorneys) and paperwork together more urgently than we would of previously (Focus Group 7)
Theme 5: What Helped us During the Pandemic
Despite efforts across the organization to provide support, nurses pointed out that there are still missing components. One nurse leader explained that nurses want to feel more appreciated (Focus Group 4). Another nurse reflected on the need for, “Better training for us as staff to actually notice when people hit their stress points, their limits” (Focus Group 1). Patients’ recovery stories helped nurses see the importance of their work and motivated them to continue to do their difficult job. The thing that kept my mental health strongest was a patient who was one of our first Covid patients who we intubated and put on CVVH. He was up and down and doing better and worse. Then he started getting better and better. I cared for him through the entire course of his stay. I got to bring his wife in to visit him for the first time in three months. And that was beautiful and probably the only thing that kept my head above water for the first few months of dealing with this. I was very blessed to have him as a patient for so many times because that progression kept me going… (Focus Group 3)
Theme 6: What Hurt us During the Pandemic
Nurses and nurse leaders discussed many factors that made their already difficult jobs more challenging professionally and personally.
Theme 7: We are not Okay
Focus Group Acceptability and Feasibility
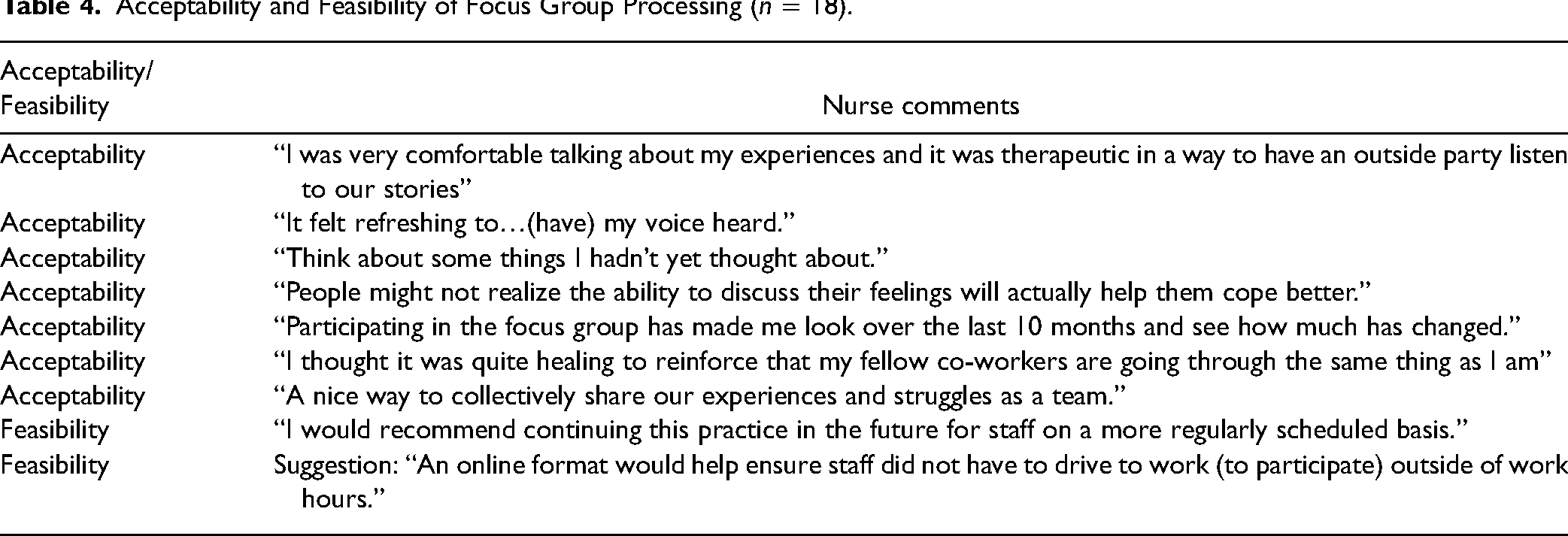
Table 4 highlights comments from nurses who responded to open-ended questions (n = 18) about the feasibility and acceptability of the focus groups. Overall, the comments support the acceptability of group-based processing. While one nurse commented that the discussion “brought back unwanted feelings,” most nurses commented that talking to the group was helpful in working through shared trauma. Although it required a time commitment, nurses shared that participating in the study was useful and feasible.
Acceptability and Feasibility of Focus Group Processing (n = 18).
Discussion
This study described the lived experience of nursing staff and nurse leaders working in COVID-19 devoted units prior to vaccine availability. To our knowledge, this is the first exploratory study of nurses’ experiences caring for patients with COVID-19 that applied a bereavement framework. Coping with loss requires the construction of a new reality in which one's view of the self and the world are vastly different (Gillies & Neimeyer, 2006; O’Connor, 2003). Findings from this study suggest nurses were still in the process of meaning reconstruction during the timeframe of this study. During the focus group discussions, nurses were making sense of bearing witness to so much death. They expressed appreciation for the opportunity to process this with colleagues who understood the intense experience of nursing during a pandemic.
By including nurse leaders, this study makes a unique contribution to the literature on the impact of the COVID-19 pandemic on healthcare professionals. While nurse leaders and staff nurses shared many of the same burdens, nurse leaders faced the challenge of implementing top- down administrative directives while supporting their staff, which tested their leadership. Consistent with emerging literature (Arcadi et al., 2021; Gunawan et al., 2021), nurses participating in this study felt exhausted and overwhelmed by rapid changes to practice. Nurse leaders were protective of nursing staff and determined to ensure that nurses had a voice during continual changes to protocols. They listened and absorbed staff suffering, increasing their own trauma. They deepened their bonds with fellow leaders, as did nurses with their colleagues.
This study was conducted during the downtrend of the first COVID-19 surge. Given the timing, the finding of moderate moral distress levels for nurses and nurse leaders points to the possibility that the pandemic created moral residue (Epstein & Hamric, 2009). Of concern, nurses in this study described experiences of moral injury. Moral injury occurs when one violates their personal or professional ethics in a high stakes situation (Richardson et al., 2020). Nurses felt tremendous guilt about their inability to relieve the immense suffering of their patients. Nurses were traumatized by delivering bad news to families and facilitating tragic telehealth visits between unresponsive patients and their families. Nurses expressed feeling hardened and numb and felt demoralized by being unable to fully provide the palliative and end of life support they felt their patients deserved. Other qualitative studies report similar findings (Dohrn et al., 2022; Galehdar et al., 2020; Gordon et al., 2021). In a study of 595 healthcare professionals, nurses reported the highest incidence (38.1%) of clinically significant moral injury (Rushton et al., 2022). Described as a “soul-ceasing experience,” moral injury often leads to a sense of betrayal (Richardson et al., 2020). This aligns with our findings that while nurses felt supported by their nurse unit leaders, they felt abandoned by the interprofessional team, high level administration, their communities, and society as a whole.
ICU nurses reported higher PTSD symptoms compared to recent veterans or patients after traumatic injury (Guttormson et al., 2022). Although we did not quantitatively measure PTSD or moral injury, nurses in our study described experiencing symptoms of PTSD and moral injury. For these nurses, the continuous exposure to death and the dire situation of limited resources was seared into their memories. Nurses and nurse leaders described their awakening when they acknowledged their post-traumatic stress symptoms. They had not anticipated they would have to consider post-traumatic stress as a daily hazard of their job.
Two systems issues that greatly impacted nurses’ and nurse leaders’ experiences was the lack of preparation for the pandemic and the depletion of resources that were essential to safely caring for the COVID-19 patient population (Chegini et al., 2021; Dohrn et al., 2022; Gunawan et al., 2021; Muz & Erdoğan Yüce, 2021). Across these studies, and captured in our subtheme of “inadequate resources and support,” nurses describe their shock, fear, and anger about how they did not have the tools and resources to do their job adequately and safely. Lack of healthcare system readiness was the root cause of their sense of fear and helplessness. Through pandemic lessons learned, nurses and nurse leaders can provide the roadmap for organizations to ensure that they are fully prepared for such future pandemics and other public health emergencies.
A resounding message from nurses in our study was that talking to other nurses who understood their story was their preferred strategy for coping. Peer-to-peer support program for healthcare professionals is an emerging strategy for health care systems to support their staff. At the time of our study, our hospital system had just launched a new peer-to-peer support training program. In a pilot of a peer support program conducted pre-pandemic, nurses reported their colleagues as the most important source of support, and of the respondents who received the peer support intervention, 100% found it helpful and would recommend it to others (Graham et al., 2019). This aligns with our results suggesting that a peer support intervention would be preferred and valued by nurses who are living through a pandemic.
Our findings suggest that an intervention for nurses that targets emotional distress is warranted. For example, Rosa et al. (2022) are adapting meaning centered psychotherapy (MCP) for healthcare professionals (MCP-HCP) (Rosa et al., 2022). MCP targets spiritual/existential distress by helping participants connect and reconnect to meaning and purpose (Breitbart et al., 2018, 2012, 2010, 2015). Outcomes of MCP include decreased anxiety and depression and increased spiritual well-being and quality of life (Breitbart et al., 2018, 2012, 2010, 2015). To date, there are few interventions that target existential distress among nurses. MCP-HCP could be delivered in a group format, which is responsive to the desire of nurses in our study to process their experiences with fellow nurses. MCP-HCP could also lay the foundation for creating moral communities where nurses can feel like they matter and the work they do makes a difference (Epstein et al., 2020).
Strengths and Limitations
This was a single site study at an academic medical center. The nurse and nurse leader sample reflects a subset of the larger nursing population working with COVID-19 patients at our institution. Self-selection bias likely impacts our results. We made considerable efforts to obtain a representative sample of nurses by extending our recruitment activities until there was no further interest in participation. The study team offered both focus groups and one-on-one interviews to accommodate the burden and stress of the pandemic. Those who participated in one-on-one interviews did not have the opportunity to experience meaning reconstruction with their peers, an aim of the study.
Implications for Clinical Practice
A clear message from our study and the broader literature is the need for systems to create policies and an infrastructure that supports nurses. Nurses in our study suggested that organizations offer training so nurses could recognize mental health crises among their peers. Peer support programs for nurses require further evaluation and testing. When comparing the health of the work environment from 2018 to 2021, there were dramatic decreases across all domains and moral distress ratings doubled (Ulrich et al., 2022). Further, pandemic preparation is a critical priority to ensure that healthcare organizations can provide adequate support to keep their staff safe (e.g., appropriate PPE), as well as address their psychological well-being (trauma-informed care and grief support) (Arabi et al., 2021). As nurses reconstruct meaning in this time of tremendous loss there is opportunity to promote the health of the work environment. A promising strategy is building an ethics infrastructure that supports nurses (Schlak et al., 2022). For example, a moral distress consultation service (Hamric & Epstein, 2017) could help nurses work through the moral injury they have endured, critically reflect on their experiences, and use the lessons they have learned from their experiences to transform healthcare.
Conclusions
We captured the perspectives of both nurses and nurse leaders, and noted that each experienced unique burdens based on their professional role. Nurses had to absorb the suffering of patients and families, while nurse leaders absorbed the suffering of their staff. As nurses and nurse leaders reconstructed the meaning of their experiences, they recognized that their team was a critical source of support that allowed them to continue to do their work. Importantly, nurses and nurse leaders who participated in this study valued the opportunity to process the meaning of their experiences; thus, group-based meaning-making for nurses is an important area for intervention development and testing. Organizations need to partner with nurses and nurse leaders to determine how to meet their ongoing need for support as we recover from one of the most tumultuous times in healthcare.
Footnotes
Acknowledgments
We express our deep appreciation to the nursing professionals who shared their stories and the nurse leaders who supported the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.