
Abstract
Introduction
The COVID-19 pandemic has led to a dramatic loss of human lives worldwide.
Objective
This study aimed to investigate the psychological factors of the COVID-19 pandemic in the community-dwelling older population.
Method
This was a cross-sectional study of older people aged ≥60 years with no mental or psychological illnesses. A total of 193 participants were recruited. The study questionnaire included anxiety- and depression-related questions tailored for the COVID-19 pandemic. The questionnaire was developed through a literature review and expert review. Data was collected from December 2020 to January 2022.
Results
The psychological symptoms of COVID-19 were high in this sample (mean 29.18 ± 3.57). Gender (female) was found to have a strong positive relationship with the psychological symptoms of COVID-19 score (p = 0.003). Chronic illnesses (β = 0.19, p < 0.001), living alone (β = 0.39, p < 0.001), and having a family member or a friend with COVID-19 (β = 0.15, p < 0.001) were also found to have a strong positive relationship with the psychological symptoms of COVID-19 score.
Conclusion
The negative psychological effects of COVID-19 were high among the older population in Oman. In this study, female gender, chronic illnesses, living alone, and having a family member or a friend with COVID-19 were associated with worse COVID-19 psychological symptoms. Older women were affected by COVID-19 more than older men. In addition, those who had chronic illnesses, lived alone, or had a family member or a friend with COVID-19 were more psychologically burdened by the pandemic than those without those characteristics. Particular attention should be given to older adults who have chronic illnesses, live alone, or have a family member or a friend with COVID-19. Support groups and psychological counseling programs are essential for older people during a pandemic.
Introduction
In January 2020, the World Health Organization (WHO) declared an outbreak of a new coronavirus disease, COVID-19, to be a public health emergency internationally (Kodvanj et al., 2020). In March 2020, the WHO assessed that COVID-19 could be characterized as a pandemic (Kodvanj et al., 2020). The COVID-19 pandemic has led to a dramatic loss of human life worldwide and presents a challenge to public health, food systems, and working life, thereby affecting the world economy (Hashem et al., 2020). COVID-19 was responsible for at least 3 million excess deaths in 2020 (Kodvanj et al., 2020; Rossen et al., 2020). The economic and social distractions caused by the pandemic were overwhelming, where tens of millions of people were at risk of deteriorating into poverty. In 2021, the number of undernourished people was expected to rise from 690 million to up to 822 million by the end of the year (Bongaarts, 2021). In Oman, as of April 2023, there were 399,449 cumulative cases and 4,628 cumulative deaths (World Health Organization, 2023). The mean reported age of patients with COVID-19-related mortality was 58 (± 18) years (Al Awaidy et al., 2021). In response to the accelerating pandemic, the WHO issued specific guidelines to reduce, or at least slow, the spread of COVID-19. Among these guidelines were stay-at-home orders, travel bans, and the closure of shops, as well as other essential services in the community, and even places of worship. Also included were avoiding clusters and closed crowded spaces and maintaining social distance of at least 1 m from any other individual (Grover et al., 2020; Karyamsety & Hesham, 2022). These restrictions altogether affected the psychological well-being of older adults.
Literature Review
The occurrence of infectious diseases, such as COVID-19, is closely associated with symptoms of psychological distress and mental illnesses. Past epidemics such as Ebola and SARS have shown that such conditions may cause depression, anxiety, and even suicide (Cheung et al., 2008; Javelot & Weiner, 2021; Matua & der Wal, 2015; Tucci et al., 2017). The fear of infection extends to the entire population, not merely the infected individuals. For example, according to a recent analysis, nearly half of COVID-19 sufferers experienced depressive feelings due to the pandemic. Likewise, previous experiences with infectious diseases have a considerable influence on mental health (Grover et al., 2020). Therefore, the number of people mentally affected by the pandemic exceeds the number of those physically infected (Grover et al., 2020). In Oman, a recent analysis of 830 people from the general affected population showed that 4.2% and 14.9% of the total participants reported depressive or anxiety symptoms, respectively, while 8.7% reported having both depression and anxiety (Al-Jadidi et al., 2022). This might be because of the ongoing pandemic and the uncertainty it has brought on.
Older people were at high risk of depression and anxiety symptoms during the pandemic according to a meta-analysis of 30 studies worldwide (Su et al., 2023). Due to geriatric physiological and psychological changes, older people may have difficulty caring for themselves and may become dependent on their family or caregivers. This can become more challenging in emergencies. The WHO stated that older adults, especially those in isolation and those with cognitive decline such as dementia, might become more anxious, angry, stressed, agitated, and withdrawn during the outbreak or while in quarantine (Al-Jadidi et al., 2022). A meta-analysis of 19 studies investigating the general population found that respondents reported being psychologically affected at a moderate or severe level, with some reporting symptoms of severe depression, anxiety, and stress (Xiong et al., 2020). However, older people were more affected by depression and anxiety during the pandemic (Al-Jadidi et al., 2022).
The mental distress among older people has been worsened further by the prolongation of the pandemic and the strong measures being implemented worldwide to prevent the spread of COVID-19, such as avoiding social activities, social distancing, and isolation. Furthermore, social isolation can increase the risk of cardiovascular, autoimmune, neurological, and mental health problems (Peçanha et al., 2020; Walker et al., 2019). The topic of psychological symptoms of COVID-19 among the older population has not been sufficiently studied in Oman. Therefore, there is a need to shed light on this issue to understand how older people have responded to the pandemic. This study aimed to investigate the factors associated with psychological symptoms of COVID-19 among the community-dwelling older population. It was hypothesized that participants in this study would have higher psychological disturbance.
Methods
Design
This is a cross-sectional study that was performed using an online screening questionnaire in Google Forms through social media groups that included citizens and/or residents of Oman.
Research Questions
What is the level of psychological symptoms of COVID-19 among the community-dwelling older population?
What factors are associated with psychological symptoms of COVID-19 among the community-dwelling older population?
Sample
Convenience sampling was used, and all eligible subjects were approached and recruited for this study. Oman's official definition of older adults (≥60 years) was used in this study. The sample size was calculated using open EPI according to the total number of elders in Oman (182,213 = 6% of the total Omani population). The percentage of elders with depression during the post-SARS period was 32.4%, so at a 95% confidence interval, the sample size was calculated to be 336. A total of 193 participants were recruited because of the low response rate; however, this number was sufficient to reach statistical significance. Older adults living in the community were the target of this study. Patients were approached online by sending invitations on social media, i.e., through Twitter and WhatsApp. In addition, participants were recruited during routine hospital appointments. Participants who responded and agreed to participate were provided with a Google Form link through WhatsApp. Hospitalization is one of the major events that contribute to psychological disturbance and low quality of life in older adults (Su et al., 2023). Therefore, it was decided to focus on older adults living in the community rather than those in hospitals or elderly care facilities.
Inclusion/Exclusion Criteria
Inclusion criteria were older people who were ≥60 years old and had no mental or psychological illnesses. Those who indicated having substance use disorder (SUD), neurocognitive disorders, or a history of mental or psychological illnesses were excluded.
Data Collection Instrument
All factors were measured through a self-administered questionnaire. These factors were chosen based on the most common factors described in the literature. The online questionnaire included several parts. First, the sociodemographic data included age, gender, marital status, education, financial circumstances, and living circumstances. Second, clinical data included history and types of medical and mental illnesses, drug and alcohol use, smoking, and family history of mental illness. The question on mental illness was to ensure that the patient had not been diagnosed with any mental illness, which could affect the results of this study. If the patient had a mental illness and/or depression, the patient would be excluded. However, none of the patients indicated having a mental illness in this study. Third were COVID-19-related questions, which included the COVID-19 quarantine measures and having a family member, friend, and/or neighbor who was diagnosed with COVID-19 or lost for the same reason. Fourth was the assessment of anxiety symptoms that emerged during the COVID-19 pandemic by simple anxiety-related questions and of depressive symptoms by simple depression-related questions.
The study team developed the questionnaire through a literature review and based on the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders (DSM-5) published in 2013 (Sarmiento & Lau, 2020). We sought to develop a tool that was tailored to the COVID-19 situation. When the tool was developed, there were no tools that were specific to the COVID-19 pandemic; only general tools were available, which might not be sensitive enough to measure all symptoms related to the COVID-19 pandemic. It was reviewed by the study team, who were experts in the field, and was piloted on 20 participants before the initiation of the study. The pilot study reported that the questions were clear, readable, and understandable. An analysis of the pilot study showed a good internal consistency of 0.82. No items were deleted or modified from the piloted questionnaire.
The tool consisted of 21 items on a 5-point Likert scale from 0 to 4 asking patients to rate their anxiety and depressive symptoms. A composite score was calculated by adding all points from the 21 questions. The highest possible score was 84, and the lowest possible score was 0; any score above 20 was considered high. The proposed cut-off score of 20 was identified based on similar existing tools on depression and anxiety, modified to reflect the current instrument's scale of 0–4 versus the others’ 1–5. A score of less than 20 indicates a low burden of psychological symptoms, and a score of 20 or higher indicates a high burden of psychological symptoms (Manea et al., 2015; Schalet et al., 2014; Yu et al., 2019). Further studies will need to validate the proposed cut-off point in different populations. We followed the WHO guideline on translation, the tool was originally developed in English and was translated into Arabic, then back translated to English by professional specialists (WHO, 2018). The tool's reliability was calculated using internal consistency (Cronbach's alpha = 0.82). The tool was previously validated successfully (Al-Jadidi et al., 2022). Data was collected from December 2020 to January 2022.
Statistical Analysis
Data were checked for normality, variance, and homogeneity, and all assumptions were tested before statistical analysis. The data was normally distributed. The sample was described using frequencies for categorical data. Bivariate correlation was used to test significant linear relationships between the independent study variables listed in Table 1 and the dependent variable of “psychological symptoms of COVID-19.” The resulting Pearson correlation coefficients using a two-tailed test of significance were examined carefully to choose the variables to enter the linear regression model (significance was set at 0.05). Only significant variables were then entered into the linear regression model, as shown in Table 2. Analysis was done using the Statistical Package for the Social Sciences (SPSS version 23).
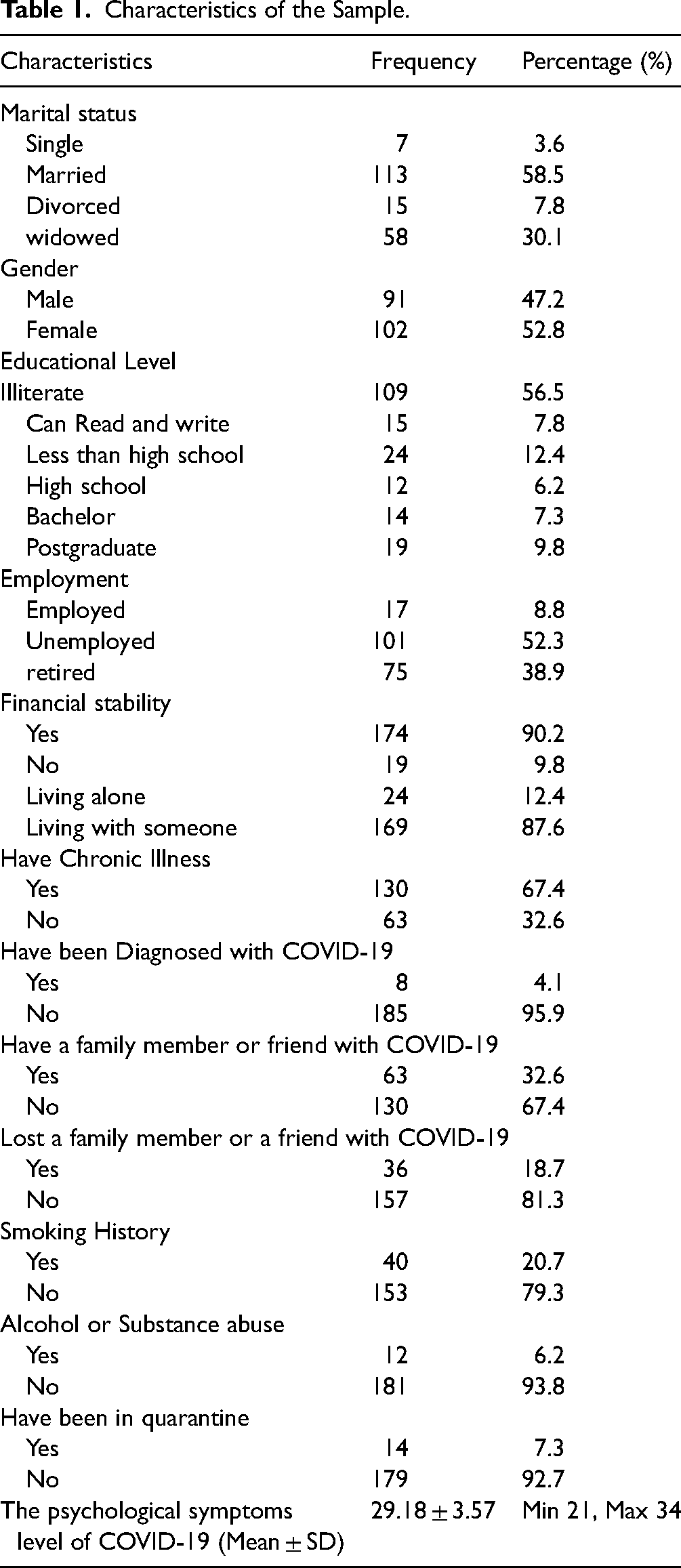
Characteristics of the Sample.
Linear Regression of the Determinants of Psychological Symptoms of COVID-19.

Note: **significant at < .001, * < .01.
aReference group is those with the chronic disease.
bReference group is those who do not have someone with COVID-19.
Ethical Considerations
Consent was obtained from all participants before filling out the questionnaire. Participants were given the option of withdrawing and abstaining from filling out the questionnaire at any time. The questionnaire was designed in a short format to limit the risk of fatigue and exhaustion in older people. All information obtained was treated as anonymous, and confidentiality was practiced in all steps of this study. Ethical approval for this study was obtained from an educational institution in Oman. The study was carried out in accordance with the Declaration of Helsinki, and the institutional ethical committee gave its approval. The STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) Statement was followed in the preparation of this manuscript. All data were managed cautiously and kept on an encrypted device. All those who were identified with high psychological symptoms were referred to psychological counseling through an outpatient clinic.
Results
Sample Characteristics
This sample included 193 participants who were all at least 60 years old. Most of the participants were married (58.5%), female (52.8%), uneducated (56.5%), and unemployed (52.3%). Most of the participants indicated that they were financially stable (90.2%) and were living with someone (87.6%). As expected, most of the participants had more than one chronic illness (67.4%). Most of the participants were not smokers or drinkers: Only 20.7% were smokers and 6.2% were alcohol drinkers. Only 4.1% of the sample had been diagnosed with COVID-19, 7.3% indicated having been quarantined, and 32.6% had a family member or a friend who had COVID-19. All descriptive statistics are provided in Table 1.
Psychological Symptoms Level of COVID-19
The psychological symptoms level of COVID-19 was high in this sample, with a mean score of 29.18 ± 3.57 with a minimum score of 21 and a maximum score of 34, as detailed in Table 1.
Factors Associated with Psychological Symptoms of COVID-19
Gender (female) was found to have a strong positive relationship with psychological symptoms of COVID-19 score (β = 0.13, p = 0.003). Chronic illnesses (β = 0.19, p < 0.001), living alone (β = 0.39, p < 0.001), and having a family member or a friend with COVID-19 (β = 0.15, p < 0.001) were also found to have a strong positive relationship with the psychological symptoms of COVID-19 score. That is, females were more affected than males in this sample. Also, those who were living alone were more affected than those who were living with someone. In addition, those with chronic illnesses were more psychologically disturbed during the COVID-19 pandemic than those who did not have chronic illnesses. Those who had a family member or a friend with COVID-19 were also affected more than others who didn’t, as described in Table 2.
Discussion
This is the first study that investigated the psychological symptoms of the COVID-19 pandemic among older people in Oman and one of very few globally. This study found that the psychological symptoms of COVID-19 were high in older people regardless of whether they had the disease or not. This is consistent with what has been reported globally (Meng et al., 2020) and in Oman as well (Al-Jadidi et al., 2022). This could be mostly related to social isolation and loneliness. Female participants were more prone to be affected than males. Those who had chronic illnesses, lived alone, or had a family member or a friend with COVID-19 were more affected by the pandemic than their counterparts. This could be because females are more expressive than males and may not seek social desirability as much as males (Alkhamees et al., 2020). It may also be because older women have more responsibilities in terms of chores than men at home, and with the pandemic, the responsibility became more difficult. However, our finding is consistent with what has been reported during the COVID-19 pandemic: Females were more affected negatively by the pandemic than men (Ayalon et al., 2020; Briguglio et al., 2020). Our finding that those who were living alone were more affected than those who were living with others was very much expected and supported by literature from other countries (Kalabikhina, 2020; Zeligman et al., 2018; Zhao et al., 2018). Social support plays a major role in coping with illnesses and in mitigating the loneliness that is usually experienced by older adults (Min et al., 2017). It was also found that those with chronic illnesses were more affected by the pandemic than others who did not. This is not surprising given the nature of chronic diseases, such as diabetes and hypertension, and the management that the patient goes through (Chudasama et al., 2020; Kalra & Sharma, 2018; Kopasker et al., 2018). In addition, fear and anxiety may have been higher because they feared that their conditions might worsen if they were infected. Our finding has been supported by the perspectives of others (Chudasama et al., 2020). Finally, having a family member or a friend who had COVID-19 was one of the factors associated with psychological symptoms of the COVID-19 pandemic in older people. This could be due to being emotionally disturbed to receive the news and realizing that they might get it, since their relatives or friends had gotten the disease. In addition, the uncertainty of what would happen to their loved ones and themselves may have been a reason for psychological distress.
Further, people's mental health and well-being were likely to be impacted by their job and financial uncertainty. As such, working from home was linked to emotional exhaustion due to isolation from colleagues (Toscano & Zappalà, 2020). Many people were unable to retain their jobs (Toscano & Zappalà, 2020). Economic insecurity harms mental health, and worries about future finances have the greatest effect (Kopasker et al., 2018). In addition, financial insecurity is linked to an increase in the risk of attempting suicide (Fiksenbaum et al., 2017). During a pandemic, such as COVID-19, emotions such as fear and anger increase the rate and severity of symptoms in vulnerable social groups, such as older people (Torales et al., 2020; Xiong et al., 2020). Although COVID-19 affects all age groups, most of the confirmed cases and deaths were found in older people (Kadambari & Vanderslott, 2021; Wyper et al., 2022). This is because of older people's vulnerability to the virus (Wyper et al., 2022). Additionally, older people are vulnerable to serious infections and death due to reduced immune function and existing health conditions caused by aging (Araújo et al., 2021; Sinclair & Abdelhafiz, 2020). More than 80% of deaths were found in patients aged >65 years, as reported by the U.S. Centers for Disease Control and Prevention (CDC) in March 2020 (Case Studies on the {PHEIC} Declaration, 2021). Likewise, it was reported in China that the incidence of severe infections in the age groups of 50–64, 65–79, and 80 years and above were approximately 19.8%, 43.2%, and 81.3% (Niu et al., 2020). Additionally, the mortality rate of the age groups reached 1.2%, 4.5%, and 18.8%, respectively (Niu et al., 2020). Therefore, more factors should be investigated when trying to describe psychological symptoms.
Strengths and Limitations
This is the first study that investigated the psychological symptoms of the COVID-19 pandemic among older people in Oman and one of very few globally. Our ability to infer causal relationships is limited by the fact that the design was cross-sectional, and data were collected at one point in time. This study did not address how patients might react to the pandemic over time. Future experimental and/or longitudinal studies may help in that regard. Data were collected during the pandemic; findings may be different after the end of the pandemic, as society has gained more clarity about the COVID-19 pandemic and ways to manage it. Moreover, there may have been many more factors that affected older people during the pandemic than were presented here. One main factor could be senescence. Therefore, more factors should be investigated in future research. This study will help clinicians better plan for interventions directed toward caring for older people during infectious disease pandemics.
Implications for Practice
This study is among the few in the world that discussed the symptoms of COVID-19 in older people and the first in Oman. Results from this study may be generalized to nearby countries with the same cultural context and may apply to the broader population of older people. More research is needed in this area, especially using a qualitative approach to understand the factors that may lead to psychological distress during a pandemic in this population. Our results can be very useful to clinicians and healthcare providers when dealing with older people during a pandemic. Older women, those who lived alone, and those with comorbidities were more prone to psychological distress during the pandemic. However, the psychological aspect of care is usually neglected in favor of a focus on physical issues. Also, patients were treated the same using the same approaches without considering factors related to psychological distress. Clinicians should consider enhancing awareness regarding meditation and relaxation techniques to reduce psychological stress (Sidi, 2020). This study has helped to shed light on tailoring interventions for the treatment of older people. Female patients need special attention, as they are more affected. Patients with chronic illnesses and those who have no social support should receive special consideration. Support groups and psychological counseling programs are essential for older people during a pandemic.
Conclusion
In conclusion, all members of the community faced challenging times during the COVID-19 pandemic, yet the older population may have been at the highest risk of psychological distress. This population is at higher risk than others because of the nature of their life in terms of chronic diseases and loss of social support. This study found that female gender, chronic illnesses, living alone, and having a family member or a friend with COVID-19 were associated with worse COVID-19 psychological symptoms. Older women were affected by COVID-19 more than older men. In addition, those who had chronic illnesses, lived alone, or had a family member or a friend with COVID-19 were more affected psychologically by the pandemic than those who didn’t. Better considerations and services should be given to older people during any pandemic. This study will help tailor the interventions or treatments for older patients. Special attention should be given to older adults who have chronic illnesses, live alone, or have a family member or a friend with COVID-19 or with other diseases. Support groups and psychological counseling programs are essential for older people during a pandemic.
Footnotes
Acknowledgement
We acknowledge all the study participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.